
The Low FODMAP Diet for SIBO: A Phase-Based Approach to Long-Term Healing
A comprehensive guide on using the low FODMAP diet as a therapeutic tool for SIBO management, focusing on elimination, reintroduction, and maintenance.
# The Low FODMAP Diet for SIBO: A Phase-Based Approach to Long-Term Healing
The modern landscape of gastroenterology is undergoing a paradigm shift. For decades, patients presenting with chronic bloating, abdominal pain, and erratic bowel habits were relegated to the catch-all diagnosis of Irritable Bowel Syndrome (IBS)—a functional label that often served as a clinical dead-end. However, emerging research indicates that up to 78% of IBS cases are, in fact, driven by Small Intestinal Bacterial Overgrowth (SIBO).
To truly "innerstand" the pathology of the small intestine is to recognise that the problem is not necessarily the presence of bacteria, but their location. When the delicate microbial balance of the large colon migrates upwards into the small intestine, the resulting fermentation creates a cascade of physiological disruption. The Low FODMAP diet has emerged as the gold standard for managing this overgrowth, yet it is frequently misunderstood and misapplied as a permanent lifestyle.
This research piece explores the biological mechanisms of SIBO, the environmental disruptors facilitating its rise, and a clinical, phase-based protocol for genuine intestinal restitution.
The Biological Mechanisms: A Failure of Containment
The small intestine is anatomically designed for nutrient absorption, not bacterial fermentation. Unlike the large intestine, which houses trillions of microbes, the small intestine should be relatively sterile. SIBO occurs when the mechanisms that maintain this sterility fail.
The Migrating Motor Complex (MMC)
The primary "housekeeper" of the small intestine is the Migrating Motor Complex. This cyclical, electromechanical wave occurs during fasting states, sweeping undigested food and excess bacteria toward the colon. When the MMC is impaired—often due to post-infectious autoimmunity (anti-cytolethal distending toxin B antibodies) or chronic stress—bacteria remain in the small bowel, where they proliferate.
Fermentation and Gas Dynamics
When we consume Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols (FODMAPs), these short-chain carbohydrates are rapidly fermented by the misplaced bacteria in the small intestine. This process produces various gases:
- —Hydrogen: Associated with diarrhoea-predominant SIBO (SIBO-D).
- —Methane: Produced by archaea (Methanobrevibacter smithii), leading to constipation (SIBO-C/IMO).
- —Hydrogen Sulfide: Often associated with "rotten egg" gas and visceral hypersensitivity.
These gases do more than cause discomfort; they alter intestinal pH, damage the microvilli (the brush border), and can lead to increased intestinal permeability, commonly known as "leaky gut."
Environmental Disruptors: The Modern Gut Under Siege
The rise of SIBO is not an evolutionary fluke; it is a direct consequence of the modern environmental and dietary landscape.
According to the British Society of Gastroenterology, IBS-type symptoms affect between 10% and 20% of the UK population, with a significant proportion of these individuals remaining undiagnosed or mismanaged by conventional protocols.
The Ultra-Processed Food (UPF) Trap
The British diet is currently the most ultra-processed in Europe. UPFs are stripped of natural fibres and loaded with emulsifiers (such as polysorbate 80 and carboxymethylcellulose) and artificial sweeteners. These additives have been shown to degrade the colonic mucus layer and alter the enteric nervous system, effectively slowing motility and creating a breeding ground for overgrowth.
Glyphosate and Agricultural Residue
The widespread use of glyphosate-based herbicides in UK wheat production acts as a potent antibiotic. By disrupting the shikimate pathway in beneficial gut bacteria, glyphosate promotes the survival of pathogenic, opportunistic species, further tilting the scales toward dysbiosis.
The Over-Sanitisation Paradox
The "Hygiene Hypothesis" suggests that our lack of exposure to diverse environmental microbes has weakened our immune system’s ability to regulate the gut microbiome. When coupled with the over-prescription of Proton Pump Inhibitors (PPIs) in the UK—which neutralise the stomach acid that acts as a first-line defence against bacterial ingress—the small intestine becomes highly vulnerable to colonisation.
The Low FODMAP Diet: A Tool, Not a Destination
The Low FODMAP diet was developed at Monash University as a therapeutic intervention. In the context of SIBO, its purpose is to "starve" the overgrowth by removing its primary fuel source. However, long-term adherence to a strict Low FODMAP protocol can lead to a reduction in beneficial Bifidobacteria and a loss of microbial diversity. Therefore, a phase-based approach is essential.
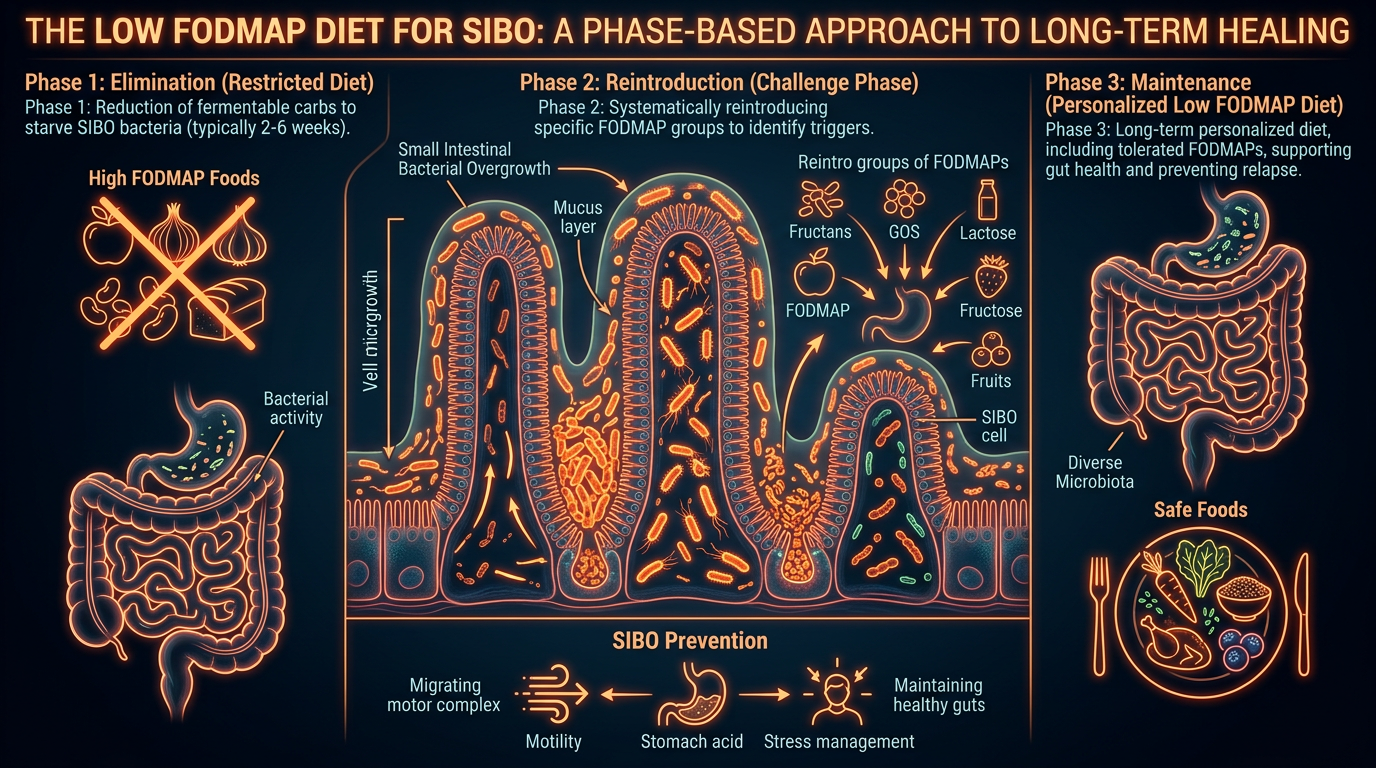
Phase 1: The Elimination Phase (The "Reset")
"Duration: 2–6 Weeks"
In this phase, all high-FODMAP foods are removed. The goal is rapid symptom reduction and the arrest of bacterial fermentation.
- —Focus: Removing fructans (wheat, onions, garlic), GOS (legumes), lactose (dairy), fructose (certain fruits), and polyols (sorbitol, mannitol).
- —Biological Intent: To lower the osmotic pressure in the small intestine and reduce the volume of gas produced. This allows the intestinal lining to begin the process of repair.
- —The "Truth-Exposing" Reality: Many practitioners stop here. However, starving the bacteria does not address the *root cause* (motility). Without moving to the next phases, SIBO is almost certain to recur.
Phase 2: Reintroduction and Challenge (The "Data Collection")
"Duration: 6–8 Weeks"
Once symptoms have stabilised, foods are reintroduced systematically to identify specific triggers.
- —Methodology: Testing one FODMAP group at a time (e.g., testing fructose with honey) over three days, increasing the dose daily.
- —The Goal: To determine individual thresholds. Most SIBO patients are not reactive to *all* FODMAPs; they may tolerate polyols but react violently to fructans.
- —Innerstanding Connection: This phase is about regaining autonomy. It shifts the patient from a "fear of food" mindset to one of physiological awareness.
Phase 3: Personalisation and Integration (The "Healing")
"Duration: Ongoing"
The final phase involves expanding the diet to include the maximum variety of foods tolerated.
- —Focus: Rebuilding the microbiome. This involves introducing "safe" prebiotics and diverse plant fibres to feed the beneficial bacteria in the large colon.
- —Supportive Therapies: This is where prokinetic agents (natural or pharmaceutical) are introduced to stimulate the MMC, ensuring that the overgrowth does not return.
The Pillars of Long-Term Healing
Diet alone is rarely sufficient to resolve SIBO permanently. A high-authority approach must address the underlying physiological infrastructure.
1. The Acid/Bile Nexus
Stomach acid (HCl) and bile are the body’s natural disinfectants. If the liver is congested or stomach acid is low (Hypochlorhydria), the small intestine loses its protection.
- —Protocol: Incorporating bitter herbs (digestive bitters) before meals to stimulate natural secretion.
- —Observation: Chronic PPI use must be reviewed under medical supervision to ensure the gut can defend itself against microbial translocation.
2. The Vagus Nerve and the Gut-Brain Axis
The MMC is governed by the Enteric Nervous System, which communicates directly with the brain via the Vagus nerve. Chronic "fight or flight" states (sympathetic dominance) inhibit the MMC.
- —Mechanism: Stress causes the body to divert blood flow away from the digestive tract, stalling motility.
- —Intervention: Diaphragmatic breathing, cold-water immersion, and mindful eating are not "fringe" therapies; they are biological imperatives for SIBO recovery.
3. Structural Integrity and the Ileocecal Valve
The Ileocecal Valve (ICV) acts as a physical barrier between the small and large intestines. If this valve is "stuck open" due to inflammation or mechanical issues, colonic bacteria can backflow into the small bowel.
- —Protocol: Manual visceral manipulation and reducing systemic inflammation through the elimination of industrial seed oils and refined sugars.
The SIBO Recovery Protocol: A Summary
For those seeking to navigate the path from dysbiosis to health, the following protocol serves as a scientific roadmap:
- —Initial Testing: Utilise a Trio-Smart or Quintron breath test to identify the specific gas profile (Hydrogen vs Methane).
- —Dietary Restriction: Implement the Low FODMAP diet for 4 weeks to reduce the bacterial load and calm the immune system.
- —Antimicrobial Intervention: Where necessary, use herbal antimicrobials (such as Allicin, Berberine, or Neem) to further reduce pathogenic populations.
- —Prokinetic Support: Crucially, introduce a prokinetic (e.g., Ginger root, 5-HTP, or Prucalopride) at bedtime to stimulate the MMC during the overnight fast.
- —Meal Spacing: Leave 4–5 hours between meals and avoid snacking to allow the MMC to complete its cleaning cycles.
- —Reintroduction: Gradually bring back high-fibre foods to foster a resilient, diverse microbiome.
"A 2021 study published in the *Journal of Gastroenterology and Hepatology* found that patients who utilised a prokinetic agent following SIBO treatment remained in remission significantly longer than those who relied on dietary changes alone."
Conclusion: Beyond Symptom Management
The journey through SIBO is often one of frustration and cyclical relapse. However, by adopting a phase-based approach to the Low FODMAP diet, we move beyond the simplistic "kill" mentality of conventional medicine and toward a model of "restoration."
True "Innerstanding" of SIBO requires us to see the overgrowth not as an invading force, but as a symptom of a systemic breakdown—a breakdown exacerbated by an environmental landscape that prioritises convenience over biological compatibility. By restoring motility, respecting the phases of dietary intervention, and addressing the environmental disruptors of the modern age, long-term healing is not just possible; it is the natural outcome of a body returned to its proper ecological balance.
The small intestine is the site of our greatest vulnerability and our greatest vitality. To heal it is to heal the very core of our being.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.