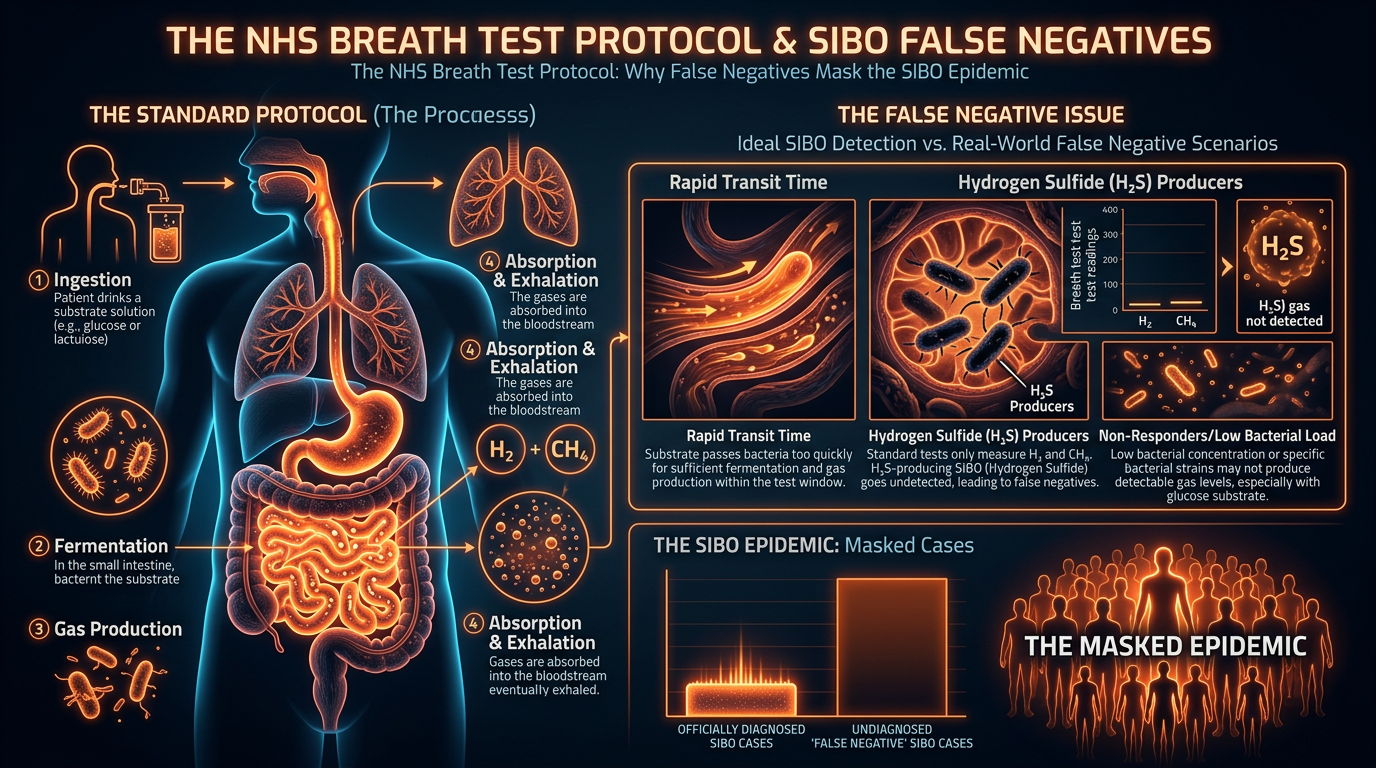
The NHS Breath Test Protocol: Why False Negatives Mask the SIBO Epidemic
Current diagnostic standards in the UK often rely on outdated glucose breath tests which fail to reach the distal end of the small intestine. This systematic failure leaves thousands of patients misdiagnosed with generic IBS.
Overview
The United Kingdom is currently weathering a silent, gastrointestinal storm. For decades, millions of patients have presented to General Practitioners with a constellation of debilitating symptoms: chronic bloating, unpredictable bowel habits, systemic fatigue, and cognitive impairment. The standard clinical response has been the assignment of a "wastebasket" diagnosis—Irritable Bowel Syndrome (IBS). However, modern biological research suggests that up to 80% of these IBS cases are, in fact, symptomatic of Small Intestinal Bacterial Overgrowth (SIBO). Despite this, the National Health Service (NHS) continues to rely on diagnostic protocols that are not only outdated but biologically flawed, leading to a staggering rate of false negatives that leave patients trapped in a cycle of chronic illness.
The fundamental crisis lies in the choice of substrate used during breath testing. While the international functional medicine community has shifted toward the Lactulose Breath Test (LBT) to capture the full landscape of the small intestine, the NHS largely adheres to the Glucose Breath Test (GBT). On the surface, this choice appears scientifically sound—glucose is a sugar that bacteria ferment, producing gases we can measure. However, the biological reality of human digestion renders glucose almost useless for detecting overgrowth in the distal (lower) portions of the small intestine. Because glucose is rapidly absorbed in the proximal duodenum, it never reaches the jejunum or ileum—the very areas where the majority of SIBO cases reside.
UK STATISTIC: It is estimated that over 10 million people in the UK suffer from IBS-related symptoms, yet fewer than 5% are ever offered a SIBO breath test. Of those who are tested within the NHS, the use of glucose-only protocols may result in a false-negative rate as high as 40-50% for distal overgrowths.
This article serves as a comprehensive interrogation of the NHS breath test protocol. We will examine the cellular mechanisms of SIBO, the physiological failure of glucose as a diagnostic marker, and the systemic environmental factors in the UK that are driving this epidemic. For the senior researcher and the informed patient alike, understanding the gap between current NHS policy and biological reality is the first step toward reclaiming metabolic and gastrointestinal health.
##
The Biology — How It Works
To understand why the NHS protocol fails, one must first understand the delicate architecture of the small intestine. Unlike the large intestine (colon), which is home to trillions of bacteria essential for fermentation and vitamin synthesis, the small intestine is designed to be relatively sparse in microbial life. Its primary function is the enzymatic breakdown and absorption of nutrients. SIBO occurs when the "migrating motor complex" (MMC)—the electrical wave that sweeps the small intestine clean during fasting—fails, allowing bacteria from the colon to migrate upwards or allowing oral bacteria to colonise the small bowel.
When these misplaced bacteria encounter carbohydrates, they ferment them prematurely. This fermentation process produces gases—primarily hydrogen ($H_2$), methane ($CH_4$), and hydrogen sulfide ($H_2S$). These gases do not remain in the gut; they diffuse across the intestinal wall into the bloodstream, where they are transported to the lungs and exhaled. This is the biological premise of the breath test: by measuring the concentration of these gases in parts per million (ppm) over a three-hour window, we can infer the presence and location of bacterial overgrowth.
The Substrate Dilemma: Glucose vs. Lactulose
The choice of "fuel" for this test determines its diagnostic reach. Glucose is a monosaccharide that is highly bioavailable to humans. Under normal physiological conditions, the human body is exceptionally efficient at absorbing glucose via the sodium-glucose cotransporter-1 (SGLT1) located in the brush border of the proximal small intestine. Consequently, when a patient drinks a glucose solution, the sugar is typically absorbed within the first few feet of the small intestine. If the bacterial overgrowth is located further down in the ileum, the glucose will never reach those bacteria, and the test will return a "normal" result despite the patient being severely symptomatic.
In contrast, Lactulose is a synthetic disaccharide that humans lack the enzymes to digest. It travels the entire length of the small intestine, from the duodenum through the jejunum and into the ileum, before finally reaching the colon. This ensures that any bacteria present along the *entire* 20-foot span of the small intestine have an opportunity to ferment the substrate. By favouring glucose for its perceived "specificity," the NHS protocol systematically ignores the distal small intestine, where a significant portion of SIBO cases—particularly those associated with chronic constipation and methane production—are located.
##
Mechanisms at the Cellular Level
The pathophysiology of SIBO extends far beyond the mere presence of gas. It is a state of cellular siege. When bacteria overpopulate the small intestine, they compete with the host for nutrients, particularly Vitamin B12 and iron. More critically, they begin to deconjugate bile acids. Bile acids are essential for the emulsification and absorption of dietary fats and fat-soluble vitamins (A, D, E, and K). When bacteria deconjugate these acids, the fats cannot be absorbed, leading to steatorrhea (fatty stools) and a slow-onset deficiency in fat-soluble vitamins that are crucial for immune function and bone health.
The Impact on the Brush Border
The lining of the small intestine is covered in microscopic, finger-like projections called villi, which are themselves covered in microvilli, forming the "brush border." This is where the final stage of digestion occurs via enzymes like lactase, sucrase, and maltase. In a SIBO environment, bacterial metabolic by-products and the bacteria themselves can physically damage these microvilli. This leads to:
- —Enzyme Deficiencies: The loss of brush border enzymes causes secondary food intolerances (e.g., lactose or fructose intolerance), which are often mistaken for the primary issue.
- —Inflammatory Signalling: The presence of Lipopolysaccharides (LPS)—endotoxins found in the cell walls of Gram-negative bacteria—triggers an immune response. This activates Toll-like Receptor 4 (TLR4) on the intestinal epithelial cells, initiating a cascade of pro-inflammatory cytokines such as TNF-alpha and IL-6.
- —Mitochondrial Stress: The enterocytes (intestinal cells) require immense amounts of ATP to maintain the mucosal barrier. LPS and excessive hydrogen sulfide can interfere with mitochondrial respiration, weakening the "tight junctions" that hold the intestinal cells together.
Methanogens: The Archaea Factor
A critical oversight in the standard NHS narrative is the role of *Methanobrevibacter smithii*. This is not a bacterium but an Archaeon. It does not produce hydrogen; it *consumes* it to produce methane. Patients with Intestinal Methanogen Overgrowth (IMO) often suffer from severe, treatment-resistant constipation because methane acts as a paralytic agent on the gut's smooth muscle, slowing transit time. Many NHS tests only measure hydrogen, meaning a patient with high methane levels could be told their test is "negative" because the methane-producing archaea have "eaten" all the hydrogen.
##
Environmental Threats and Biological Disruptors
The UK's rising SIBO rates are not accidental; they are a direct consequence of an environment that systematically undermines gut motility and microbial balance. To understand the "why" behind the epidemic, we must look at the biological disruptors prevalent in British society.
The Pharmaceutical Burden
The UK has one of the highest rates of Proton Pump Inhibitor (PPI) prescriptions in Europe. PPIs, used to treat acid reflux, significantly raise the pH of the stomach. Gastric acid is the body’s first line of defence against ingested bacteria. By neutralising this acid, we create an "open door" policy for oral bacteria to migrate into the small intestine. Furthermore, the frequent use of broad-spectrum antibiotics for minor infections disrupts the delicate balance of the microbiome, often killing off beneficial species that prevent the overgrowth of opportunistic pathobionts.
Glyphosate and the Modern Food Chain
The British diet, increasingly reliant on processed grains and industrialised farming, is a significant contributor. Glyphosate, the active ingredient in many herbicides used in UK wheat and oilseed rape production, has been shown to act as a potent antimicrobial. However, it preferentially kills "beneficial" bacteria like *Lactobacillus* and *Bifidobacterium*, while allowing more pathogenic, SIBO-associated strains like *E. coli* and *Salmonella* to thrive. Glyphosate also interferes with the Shikimate pathway, which, although absent in humans, is present in our gut microbes, leading to a profound dysbiosis that sets the stage for SIBO.
The Stress-Vagus Nerve Axis
The modern British lifestyle is characterised by chronic, low-grade sympathetic nervous system activation (the "fight or flight" response). The Vagus nerve, which governs the "rest and digest" parasympathetic state, is the primary regulator of the Migrating Motor Complex (MMC). When we are stressed, Vagal tone drops, and the MMC—the "housekeeping wave"—ceases to function. Without this clearing mechanism, bacteria that should be pushed into the colon remain in the small intestine, where they anchor and multiply.
##
The Cascade: From Exposure to Disease
The progression from initial microbial imbalance to systemic SIBO is a predictable biological cascade. It rarely happens overnight; it is the result of a cumulative breakdown of the body’s protective barriers.
Phase 1: The Failure of the Barriers
The process begins with the erosion of the "Big Five" barriers: gastric acid, pancreatic enzymes, bile flow, the Ileocecal Valve (ICV), and the MMC. If any of these are compromised—whether by stress, PPIs, or a poor diet—the small intestine becomes vulnerable to colonisation.
Phase 2: Fermentation and Gas Entrapment
Once bacteria take up residence, they begin to ferment dietary fibres and sugars. In the confined space of the small intestine, the resulting gas cannot escape easily. This leads to "visceral hypersensitivity," where the intestinal walls are stretched, sending pain signals to the brain. This is why SIBO patients often look "six months pregnant" by the end of the day, a phenomenon known as "diurnal bloating."
Phase 3: The Systemic Breach (Leaky Gut)
As the inflammation persists, the tight junctions between enterocytes fail. This is the transition from a localised gut issue to a systemic disease. Large molecules—undigested food proteins, LPS, and bacterial debris—leak into the bloodstream. This is known as "Intestinal Permeability."
ALARMING FACT: Once LPS enters the systemic circulation, it can cross the blood-brain barrier, triggering "neuro-inflammation." This explains the "brain fog," anxiety, and depression that are almost universally reported by SIBO sufferers in the UK.
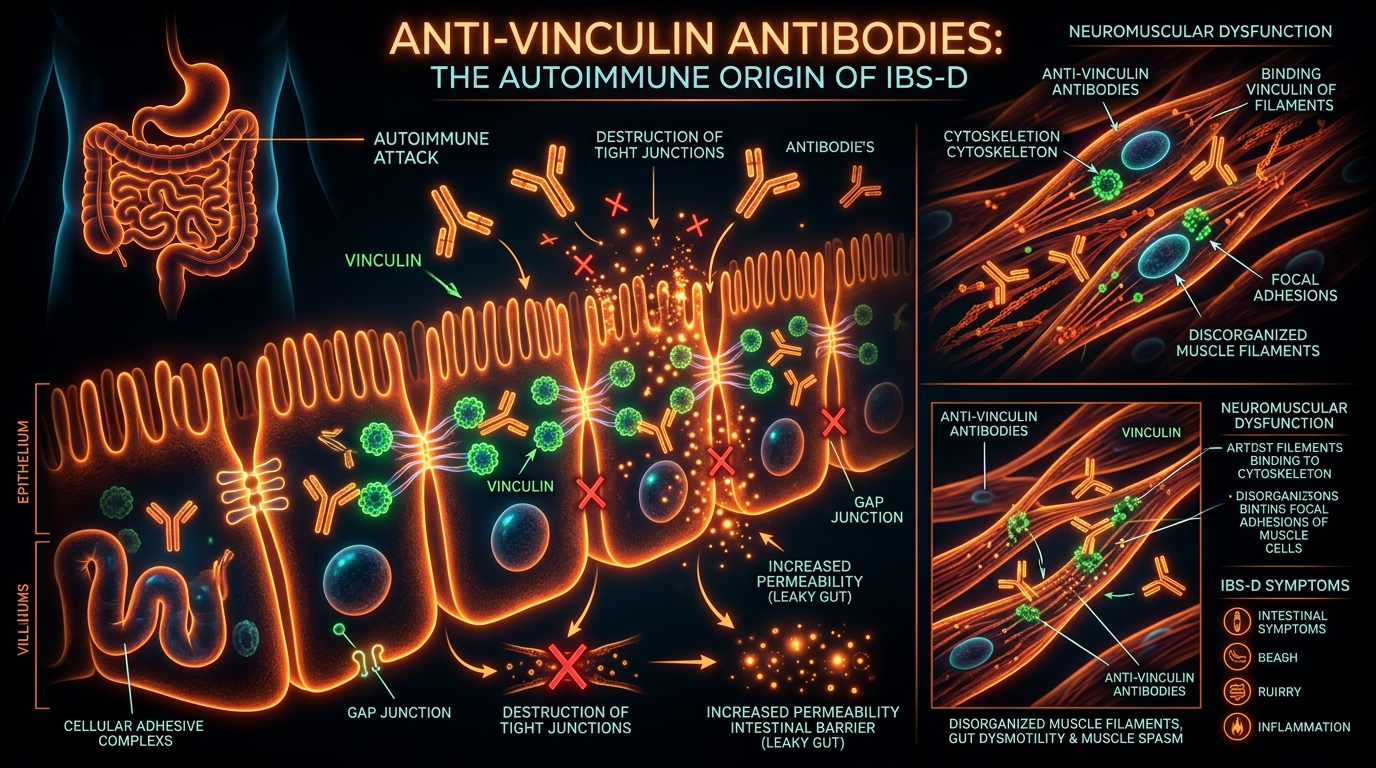
Phase 4: Autoimmune Mimicry
In some cases, particularly following an episode of food poisoning (post-infectious SIBO), the body produces antibodies against bacterial toxins like Cytolethal Distending Toxin B (CdtB). Due to a process called "molecular mimicry," these antibodies can begin to attack Vinculin, a protein essential for the function of the MMC. The body essentially begins to attack its own gut-clearing mechanism, leading to a permanent state of SIBO susceptibility.
##
What the Mainstream Narrative Omits
The NHS and broader mainstream medical community often treat SIBO—when they acknowledge it at all—as a "secondary" condition, a mere symptom of some other underlying pathology. This "bottom-up" approach misses the "top-down" biological reality.
The Myth of "IBS" as a Final Diagnosis
In the UK, IBS is frequently treated as a functional disorder, implying that the gut looks normal but isn't working correctly. This is a diagnostic failure. IBS is not a disease; it is a description of symptoms. By labelling a patient with IBS and failing to test for SIBO using a Lactulose Breath Test, the clinician is essentially ignoring a detectable, treatable bacterial overgrowth. The mainstream narrative omits the fact that "functional" symptoms often have a very real, measurable bacterial origin.
The Methane and Hydrogen Sulfide Oversight
Most NHS trusts that do offer breath testing only measure hydrogen. This is scientifically negligent. As previously mentioned, methanogens consume hydrogen. If you only measure hydrogen, you will see a flatline (a "negative" result) while the patient is actually suffering from a massive methane overgrowth. Furthermore, the third gas, Hydrogen Sulfide ($H_2S$), is almost never measured in the UK. $H_2S$ SIBO is associated with "rotten egg" smelling gas, bladder pain, and extreme fatigue, yet because the NHS lacks the triple-gas sensor technology (like the Trio-Smart test available in the US), these patients are told their gut is perfectly healthy.
The Post-Antibiotic Vacuum
When the NHS does treat SIBO, it often relies on a single course of Neomycin or Metronidazole. While these can be effective, the mainstream narrative fails to address the "post-antibiotic vacuum." Without a prokinetic (a substance to stimulate the MMC) and a comprehensive dietary "re-boot," the bacteria simply grow back within weeks. The NHS protocol lacks the nuance of long-term motility management, leading to a high rate of relapse that doctors then use as evidence that SIBO "isn't the real problem."
##
The UK Context
The failure to properly diagnose and treat SIBO in the UK is inextricably linked to the structural and financial pressures of the NHS. The "Postcode Lottery" is a very real phenomenon in gastrointestinal health.
The NICE Guidelines and Economic Rationing
The National Institute for Health and Care Excellence (NICE) provides the guidelines that govern NHS treatment. Currently, there is a lack of clear, centralised directives for the universal adoption of Lactulose Breath Testing for SIBO. Because Glucose tests are cheaper to procure and simpler to interpret (due to the lack of "double peaks" often seen in Lactulose), they remain the default. This is economic rationing disguised as clinical best practice.
The Private-Public Divide
Increasingly, UK patients are forced to seek private healthcare for a SIBO diagnosis. Private labs such as Healthpath or Gastrolife offer the Lactulose Breath Test and triple-gas testing, but these can cost hundreds of pounds—a price many cannot afford. This creates a two-tier system where those with financial means can access the "biological truth" of their condition, while the rest are left with a generic IBS diagnosis and a prescription for anti-spasmodics that do nothing to address the underlying bacterial overgrowth.
The GP Knowledge Gap
The average GP in the UK receives very little training in nutritional science or the intricacies of the microbiome. The rapid evolution of SIBO research over the last decade has outpaced the medical school curriculum. Many GPs still view the small intestine as a "sterile" environment or believe that SIBO only occurs in patients with "blind loop syndrome" or post-surgical complications. This outdated view prevents the early intervention that could save the NHS millions in long-term care for chronic GI conditions.
##
Protective Measures and Recovery Protocols
Recovery from SIBO in an environment that is "pro-SIBO" requires a multi-faceted biological strategy. One cannot simply "kill" the bacteria and expect health to return; one must restore the underlying physiological barriers.
Phase 1: The Antimicrobial Reset
The first step is reducing the bacterial load. While the NHS might offer Rifaximin (a non-absorbable antibiotic that stays in the gut), many researchers now advocate for herbal antimicrobials. Agents such as Allicin (from garlic), Berberine, and Neem have been shown in clinical trials to be as effective as Rifaximin but with a broader spectrum of action against both bacteria and archaea.
Phase 2: Restoring Motility (The Prokinetic Phase)
This is the most critical and most frequently omitted step in the UK. To prevent relapse, the MMC must be stimulated. This can be achieved through:
- —Pharmacological Prokinetics: Low-dose Erythromycin or Prucalopride (Resolor), which act on serotonin receptors in the gut.
- —Natural Prokinetics: Ginger and 5-HTP are effective at stimulating the migrating motor complex when taken on an empty stomach before bed.
- —Meal Spacing: Allowing 4-5 hours between meals to give the MMC time to complete its "clearing waves."
Phase 3: Structural and Vagal Support
The physical position of the gut and the tone of the Vagus nerve must be addressed.
- —Visceral Manipulation: Specialized physiotherapy can help ensure the Ileocecal Valve (the gate between the small and large intestine) is functioning correctly and not "stuck open."
- —Vagus Nerve Stimulation: Techniques such as cold water immersion, gargling, and deep diaphragmatic breathing can help shift the body from a sympathetic (SIBO-promoting) to a parasympathetic (healing) state.
Phase 4: Diet as a Management Tool, Not a Cure
The Low FODMAP diet is often touted as the "cure" for SIBO in the UK. This is incorrect. The Low FODMAP diet is a symptom management tool; it starves the bacteria, but it also starves the beneficial microbes in the colon. Long-term use of restrictive diets can lead to a loss of microbial diversity. The goal should always be to treat the overgrowth and then systematically reintroduce a wide variety of plant fibres to rebuild a resilient microbiome.
##
Summary: Key Takeaways
The current NHS approach to SIBO is a relic of 20th-century gastroenterology, failing to account for the complex, distal nature of bacterial overgrowth and the distinct role of methanogens. For the millions of UK citizens suffering under the "IBS" label, the path to health requires a rejection of the glucose-only protocol and a demand for more nuanced, biologically accurate diagnostics.
- —The Glucose Failure: Glucose breath tests are biologically incapable of detecting distal SIBO because the substrate is absorbed too early in the digestive tract.
- —The Lactulose Necessity: Lactulose is the only substrate that can traverse the entire small intestine, providing a complete diagnostic picture.
- —The Methane Trap: Failing to test for methane (and hydrogen sulfide) leads to significant false negatives, particularly in patients with chronic constipation.
- —SIBO is Systemic: The breakdown of the intestinal barrier leads to LPS translocation, causing neuro-inflammation, fatigue, and systemic immune activation.
- —Motility is Key: SIBO is primarily a motility disorder. Without addressing the Migrating Motor Complex (MMC), relapse is almost certain.
- —The Environmental Context: The UK’s high use of PPIs, glyphosate-heavy diet, and chronic stress levels create a "perfect storm" for SIBO development.
The "SIBO Epidemic" in the UK is a crisis of diagnostics as much as it is a crisis of health. Until the NHS aligns its protocols with the reality of intestinal biology, the "IBS" wastebasket will continue to overflow, leaving patients to suffer in silence while the true cause of their illness remains hidden in the distal reaches of the small intestine. It is time for a radical shift in how we perceive, test, and treat the British gut.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper