Prokinetics: Restoring the Peristaltic Rhythm Post-Treatment
Prokinetics are agents that stimulate the Migrating Motor Complex to prevent the recurrence of bacterial overgrowth. Understanding the timing of these agents is the difference between a temporary fix and a permanent cure.
Overview
The human gastrointestinal tract is not merely a passive tube for the transit of nutrients; it is a sophisticated, oscillating biological engine regulated by an intricate series of electrical pulses and muscular contractions. For those navigating the treacherous waters of Small Intestinal Bacterial Overgrowth (SIBO), the focus is almost universally placed upon the "kill phase"—the eradication of pathogenic or displaced commensal bacteria through antibiotics or herbal antimicrobials. However, biological research increasingly reveals that the eradication of bacteria is a secondary concern. The primary failure in SIBO—and the reason for its staggering recurrence rates—is a profound disruption of the Migrating Motor Complex (MMC), the gut’s intrinsic "housekeeping" rhythm.
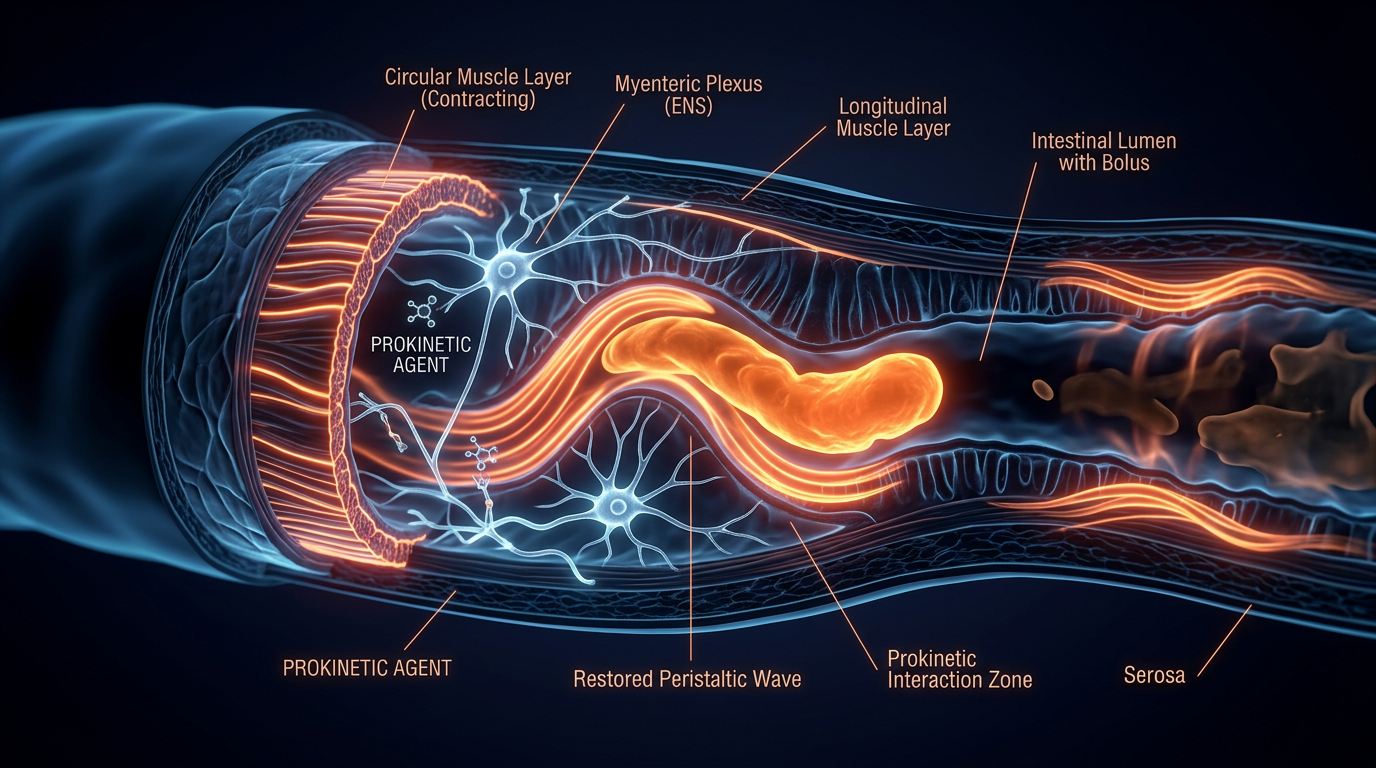
Prokinetics represent the bridge between temporary symptomatic relief and a permanent physiological cure. These are not laxatives; they are kinetic catalysts designed to restore the peristaltic rhythm that prevents the stasis of luminal contents. In the absence of a functioning MMC, the small intestine becomes a stagnant pond, an environment where bacterial colonisation is not only possible but inevitable. When we talk about prokinetics, we are talking about the restoration of biological sovereignty over the internal environment.
The "rhythm" we refer to is the periodic, coordinated movement that sweeps through the stomach and small intestine during periods of fasting. It is the body’s natural defence mechanism against the encroachment of colonic bacteria into the nutrient-rich sanctuary of the small bowel. Without this wave, the most potent antibiotics in the world are merely a stay of execution. This article will dissect the molecular, cellular, and systemic importance of prokinetic therapy, exposing the critical timing and mechanisms that the mainstream medical narrative frequently overlooks.
##
The Biology — How It Works
To understand prokinetics, one must first master the mechanics of the Migrating Motor Complex (MMC). Unlike the peristalsis that occurs during and immediately after eating—which is designed to mix food with enzymes and move it slowly for absorption—the MMC is a distinct electromechanical programme that only initiates in the interdigestive state (fasting). It is the "janitor" of the gut, clearing out undigested food particles, cellular debris, and, most importantly, excess bacteria.
The MMC operates in four distinct phases, cycling approximately every 90 to 120 minutes:
- —Phase I: A period of relative quiescence with rare, irregular contractions. This is the "reset" phase.
- —Phase II: A period of increasing electrical activity and irregular contractions that grow in frequency.
- —Phase III: The "Propulsive Peak." This is a short, intense burst of rhythmic, high-amplitude contractions that sweep from the stomach down to the terminal ileum. This is the critical "cleansing wave" that prevents bacterial stasis.
- —Phase IV: A brief transition period returning the system to Phase I.
Prokinetics function by artificially or naturally stimulating the onset of Phase III. In a healthy individual, the hormone motilin—produced by M-cells in the duodenal mucosa—triggers this wave. In the SIBO patient, this hormonal and electrical signal is often muted or entirely absent. This absence is frequently caused by damage to the enteric nervous system (ENS) or a lack of synchronisation between the brain and the gut.
The timing of prokinetic administration is the single most important variable in recovery. If a prokinetic is taken with food, its effect is negated by the "fed state" signals that override the MMC. To restore the rhythm, these agents must be introduced when the system is in a fasting state—typically at bedtime, at least four hours after the final meal. This allows the agent to stimulate the MMC during the long nocturnal fast, ensuring the small intestine is thoroughly "scrubbed" before the next day's caloric intake.
##
Mechanisms at the Cellular Level
The sophistication of gut motility is managed at the microscopic level by a specialised group of cells known as the Interstitial Cells of Cajal (ICC). Often referred to as the "pacemakers of the gut," these cells bridge the gap between the enteric nerves and the smooth muscle cells of the intestinal wall. They generate the slow-wave electrical activity that provides the baseline for contractions.
When we introduce a prokinetic agent, we are interacting with specific receptor sites on these cells and the surrounding neural network:
5-HT4 Receptors and Serotonin
Approximately 95% of the body’s serotonin is located in the gut. The 5-HT4 receptors, located on the pre-synaptic terminals of primary afferent neurons, are the primary targets for many pharmaceutical prokinetics like Prucalopride. When these receptors are stimulated, they trigger the release of acetylcholine, the primary neurotransmitter responsible for stimulating smooth muscle contraction. Without sufficient 5-HT4 activation, the "order" to contract never reaches the muscle.
Motilin Agonism
Motilin is the endogenous conductor of the MMC. Certain agents, such as low-dose Erythromycin, act as motilin agonists. They bind to motilin receptors in the stomach and duodenum, mimicking the natural "hunger" signal that initiates the Phase III wave. This is a biochemical bypass; it forces the gut to perform its housekeeping duties even if the natural signalling pathways are compromised.
The Cholinergic Pathway
Acetylcholine is the "on switch" for intestinal movement. Prokinetics often work by either increasing the release of acetylcholine or inhibiting its breakdown. This ensures that the electrical signal generated by the ICCs is successfully translated into a physical contraction. In many cases of chronic SIBO, the cholinergic tone is depleted, often due to chronic stress or neuroinflammation, leaving the gut in a state of functional paralysis.
UK FACT: Chronic digestive complaints, often misdiagnosed as generic "IBS," cost the UK economy an estimated £3 billion per year in lost productivity and healthcare resources, primarily because the underlying motility failures are never addressed.
##
Environmental Threats and Biological Disruptors
The modern environment is fundamentally hostile to the peristaltic rhythm. We are currently witnessing an epidemic of "lazy gut syndrome," which is not a failure of the individual’s biology, but a rational response to an irrational environment.
The first and most pervasive threat is the disruption of the circadian rhythm. The MMC is deeply tied to the body's internal clock. The pervasive use of artificial blue light and late-night snacking inhibits the transition from the sympathetic (fight or flight) to the parasympathetic (rest and digest) nervous system. If the body never feels truly "safe" and "at rest," it will never initiate the MMC.
Glyphosate and Agricultural Chemicals: The heavy use of glyphosate in the UK's conventional grain supply is a direct neurotoxin to the enteric nervous system. Glyphosate has been shown to disrupt the Shikimate pathway in gut bacteria, but its impact on the host is equally devastating. It can lead to the degradation of the mucosal lining and interference with the delicate signalling between the ICCs and the vagus nerve.
Ultra-Processed Foods (UPFs): The British diet is now comprised of over 50% UPFs. These "food-like substances" are engineered for hyper-palatability but lack the structural integrity to stimulate natural motility. Furthermore, the emulsifiers used in these products—such as polysorbate 80 and carboxymethylcellulose—have been shown to erode the protective mucus layer of the gut, exposing the ENS to inflammatory triggers that shut down the MMC.
Pharmaceutical Interference: The over-prescription of Proton Pump Inhibitors (PPIs) and opioids in the UK has created a generation of "static guts." PPIs reduce stomach acid, which is a key trigger for downstream motility. Without the acidic bolus entering the duodenum, the signal to initiate the MMC is significantly weakened. Opioids, on the other hand, directly bind to mu-opioid receptors in the gut, effectively freezing the peristaltic wave.
##
The Cascade: From Exposure to Disease
The path to SIBO recurrence is a predictable biological cascade. It often begins with an episode of acute gastroenteritis—food poisoning. In the UK, *Campylobacter*, *Salmonella*, and *E. coli* are the usual suspects. While the acute infection may pass, it can leave behind a devastating legacy: Cytolethal Distending Toxin B (CdtB).
The body produces antibodies to fight CdtB, but through a process known as molecular mimicry, these antibodies begin to attack a protein in the human gut called Vinculin. Vinculin is a critical "glue" protein found in the Interstitial Cells of Cajal and the enteric nerves. When the immune system attacks vinculin, it effectively dismantles the gut’s pacemaker system.
This leads to a specific sequence:
- —Autoimmunity: Anti-vinculin antibodies damage the ICCs.
- —Motility Failure: The MMC becomes infrequent, weak, or absent.
- —Stasis: Food remnants and bacteria linger in the small intestine.
- —Overgrowth: Bacteria from the colon migrate upward, and those coming down from the mouth proliferate in the stagnant environment.
- —Fermentation: Bacteria ferment carbohydrates, producing hydrogen, methane, or hydrogen sulphide gases.
- —Symptom Manifestation: Bloating, pain, malabsorption, and altered bowel habits.
If a patient undergoes an antimicrobial "kill phase" but does not address the anti-vinculin damage or the motility failure with prokinetics, the overgrowth will return within weeks. This is why SIBO is often called a "relapsing-remitting" condition. It is not that the bacteria are "stronger" than the antibiotics; it is that the "janitor" is still on strike.
ALARMING STAT: Recent studies suggest that up to 60% of people diagnosed with IBS in the UK actually have SIBO, and of those, a significant portion test positive for anti-vinculin antibodies, indicating a post-infectious autoimmune motility disorder.
##
What the Mainstream Narrative Omits
The conventional medical approach to gut health is fundamentally reactive rather than proactive. In the UK, the NHS model for "IBS" typically involves the "FODMAP diet" and perhaps an antispasmodic like Mebeverine. This approach is not only outdated; it is biologically counter-productive for the SIBO patient.
The Antispasmodic Fallacy: Antispasmodics are designed to stop the gut from cramping. In a patient with SIBO/motility failure, the gut isn't contracting *too much*; it’s contracting *ineffectively*. Giving an antispasmodic to a SIBO patient is like giving a sedative to someone who is already struggling to wake up. It further slows the MMC, worsening the bacterial stasis.
The "Kill Phase" Myopia: Doctors are trained to view bacteria as the enemy. In SIBO, the bacteria are merely a symptom of an underlying mechanical failure. The mainstream narrative focuses on "eradicating the bugs" with Rifaximin or Neomycin. While necessary, this is a temporary fix. The narrative completely omits the "Prokinetic Phase," which should ideally last for 3 to 6 months post-treatment to "re-train" the ENS.
The Myth of "Small Meals": Conventional advice often suggests "eating small, frequent meals" to manage bloating. Biologically, this is the worst possible advice for SIBO recovery. Every time a morsel of food is consumed, the MMC is instantly shut down to allow for digestion. By eating frequently, the patient ensures their MMC never has the chance to initiate. The "grazing" culture is a primary driver of SIBO persistence.
The Role of the Vagus Nerve: The mainstream model largely ignores the Gut-Brain Axis. The vagus nerve is the superhighway that carries the "go" signal from the brainstem to the gut. Chronic stress, cervical spine misalignment, and even poor posture can "kink" this signal. Prokinetics work best when the vagus nerve is also supported, yet this holistic integration is virtually non-existent in standard gastroenterology.
##
The UK Context
The United Kingdom presents a unique set of challenges for the SIBO patient. The structure of the NHS, while providing universal care, is not designed for the complex, multi-factorial management required for motility disorders.
The Diagnostic Lag
The average SIBO patient in the UK consults with five different GPs and waits an average of three years before receiving an accurate diagnosis. During this time, they are often told their symptoms are "psychosomatic" or "just stress." This delay allows the autoimmune damage (anti-vinculin antibodies) to become more ingrained, making the restoration of the peristaltic rhythm significantly harder.
The Prescription Barrier
Many of the most effective prokinetics are difficult to access via the NHS. Prucalopride (Resolor), for instance, is often restricted by NICE guidelines only to those with "chronic constipation where at least two laxatives from different classes have been tried." This ignores the millions of "IBS-D" (diarrhoea-predominant) or "IBS-M" (mixed) patients who have SIBO and desperately need prokinetic support, not laxatives.
The British "Tea and Toast" Culture
The UK's dietary reliance on refined carbohydrates and frequent "cuppas" with milk and sugar provides a constant substrate for bacterial fermentation. The cultural habit of "biscuits with tea" between meals ensures that the MMC is perpetually suppressed. Breaking this cultural cycle is as much a part of the cure as the prokinetic itself.
Environmental Toxicity in the UK
The UK’s heavy industrial past and current agricultural practices mean that British citizens are exposed to high levels of heavy metals and pesticides. These substances act as "endocrine and neural disruptors" that specifically target the delicate enteric nervous system. Without a detoxification strategy alongside prokinetic therapy, the biological rhythm remains muffled by toxic noise.
UK STAT: Public Health England reports that digestive diseases are the third most common cause of death in the UK, yet funding for research into motility and the microbiome remains disproportionately low compared to cardiovascular and oncology research.
##
Protective Measures and Recovery Protocols
Restoring the peristaltic rhythm is a marathon, not a sprint. It requires a disciplined, multi-layered approach that combines pharmacology, nutraceuticals, and lifestyle modifications. The goal is to move the gut from a state of "static inflammation" to "dynamic flow."
1. Strategic Prokinetic Timing
The most effective time to take a prokinetic—whether it is pharmaceutical (Prucalopride, Low-Dose Erythromycin, Low-Dose Naltrexone) or natural (Ginger, Artichoke)—is at bedtime.
- —The Fasting Window: Ensure there is a minimum of 4 hours between your last meal and the prokinetic dose.
- —Water Only: After taking the prokinetic, do not consume anything but plain water until the morning. This ensures the MMC has an 8-12 hour window to complete multiple Phase III cycles.
2. Natural Prokinetic Agents
For those who cannot access prescriptions or prefer a botanical approach, certain compounds have shown significant efficacy:
- —Ginger (Zingiber officinale): Acts as a 5-HT3 antagonist and 5-HT4 agonist, stimulating gastric emptying and the MMC. High-dose ginger (1000mg+) is required for prokinetic effects.
- —Artichoke Leaf Extract (Cynara scolymus): Enhances bile flow and stimulates the small intestine's motor activity.
- —Iberogast: A multi-herb tincture that has been clinically studied for its ability to regulate gastric and intestinal motility.
3. The "Inter-Digestive" Fast
To allow the prokinetic to do its job, the patient must adopt a meal-spacing strategy.
- —No Snacking: A minimum of 4 to 5 hours between breakfast, lunch, and dinner.
- —Eliminate "Hidden" Calories: Milk in tea, sugary drinks, or even small snacks will reset the MMC timer. The gut needs silence to perform its housekeeping.
4. Vagus Nerve Stimulation
The "signal" for the MMC must come from the top down. Supporting the vagus nerve is non-negotiable.
- —Gargling and Singing: Vigorous gargling or loud singing stimulates the pharyngeal muscles, which are innervated by the vagus nerve.
- —Cold Exposure: Brief cold showers or splashing ice-cold water on the face can trigger the "diving reflex," which activates the parasympathetic nervous system.
- —Diaphragmatic Breathing: Deep, belly-focused breathing signals to the brain that the body is in a "rest and digest" state.
5. Managing Autoimmunity
If SIBO is post-infectious (CdtB/Vinculin positive), the focus must also include calming the immune system.
- —Low-Dose Naltrexone (LDN): While technically a prokinetic by way of reducing inflammation in the ENS, LDN’s primary benefit is its ability to modulate the immune response and reduce the production of auto-antibodies.
- —Omega-3 and Curcumin: High-quality, bioavailable anti-inflammatories help reduce the neuroinflammation that "gums up" the electrical signalling in the gut wall.
##
Summary: Key Takeaways
The restoration of the peristaltic rhythm via prokinetics is the "missing link" in modern gastroenterology. Without it, SIBO is a revolving door of infection, treatment, and relapse. By shifting our perspective from "killing bacteria" to "restoring movement," we empower the body to heal itself.
- —Prokinetics are Housekeepers: Their job is to stimulate the MMC, not to act as a laxative. They clear the small intestine of the debris that feeds overgrowth.
- —Timing is Everything: Prokinetics must be taken during the interdigestive (fasting) state, ideally at bedtime, to be effective.
- —The MMC is the Guardian: A functioning Phase III wave is the only permanent way to prevent bacteria from the large intestine from migrating into the small intestine.
- —The UK System is Failing Patients: The lack of access to motility testing and specialized prokinetics means patients must become their own researchers and advocates.
- —Autoimmunity is the Root: For many, SIBO is a neurological/autoimmune consequence of food poisoning. Addressing the anti-vinculin damage is essential for long-term health.
- —Lifestyle is the Foundation: Meal spacing, stress management, and the avoidance of environmental toxins like glyphosate are necessary to maintain the rhythm once it is restored.
In the final analysis, the health of the human gut is not defined by the absence of bacteria, but by the presence of a strong, rhythmic, and unstoppable cleansing wave. The "Peristaltic Rhythm" is the heartbeat of the digestive tract. When it stops, disease begins. When it is restored, life flourishes. This is the path to INNERSTANDING.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Vegan Essential Amino Acids – Plant-Powered Protein Building

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper