Vitamin D Crisis: The 51st Parallel Problem
Living at British latitudes prevents natural Vitamin D synthesis for over half the year, compromising immune and skeletal integrity. We explore the physiological necessity of supplementation when sunlight-driven cholecalciferol production fails.
Overview
The 51st parallel north is more than a geographical coordinate; it is a biological threshold. For the inhabitants of the British Isles, this line represents a demarcation between physiological sufficiency and chronic, systemic failure. As a senior biological researcher for INNERSTANDING, I have observed a disturbing trend: the normalization of a profound nutritional void that compromises every major organ system in the human body.
The "Vitamin D Crisis" is not merely a matter of "getting enough sun." It is a fundamental mismatch between our ancient evolutionary requirements and our modern, high-latitude existence. Humans evolved in the equatorial sun, where UVB radiation is abundant year-round. Our migration to the grey, overcast reaches of Northern Europe was a recent event in evolutionary time—one for which our biochemistry has not yet fully compensated.
In the United Kingdom, particularly those living above the 51st parallel (which runs just south of London), the sun’s angle is insufficient to trigger the synthesis of cholecalciferol (Vitamin D3) for more than half the year. We are currently living through a biological "dark age," where a lack of this seco-steroid hormone—erroneously labelled a vitamin—is driving a hidden epidemic of autoimmune disease, cognitive decline, and skeletal disintegration.
This article serves as an exposé of the "51st Parallel Problem." We will dissect the molecular machinery that fails when the sun disappears, the environmental factors that exacerbate this deficit, and the systemic failures of public health guidelines that keep the population in a state of sub-clinical deficiency.
CRITICAL STATISTIC: Over 60% of the UK population is clinically deficient in Vitamin D during the winter months, with over 15% reaching levels associated with severe bone pathology.
---
The Biology — How It Works
To understand the crisis, one must first understand the elegant, yet fragile, mechanism of cutaneous synthesis. Vitamin D is the only nutrient that is produced through a photochemical reaction in the skin rather than being primarily derived from the diet.
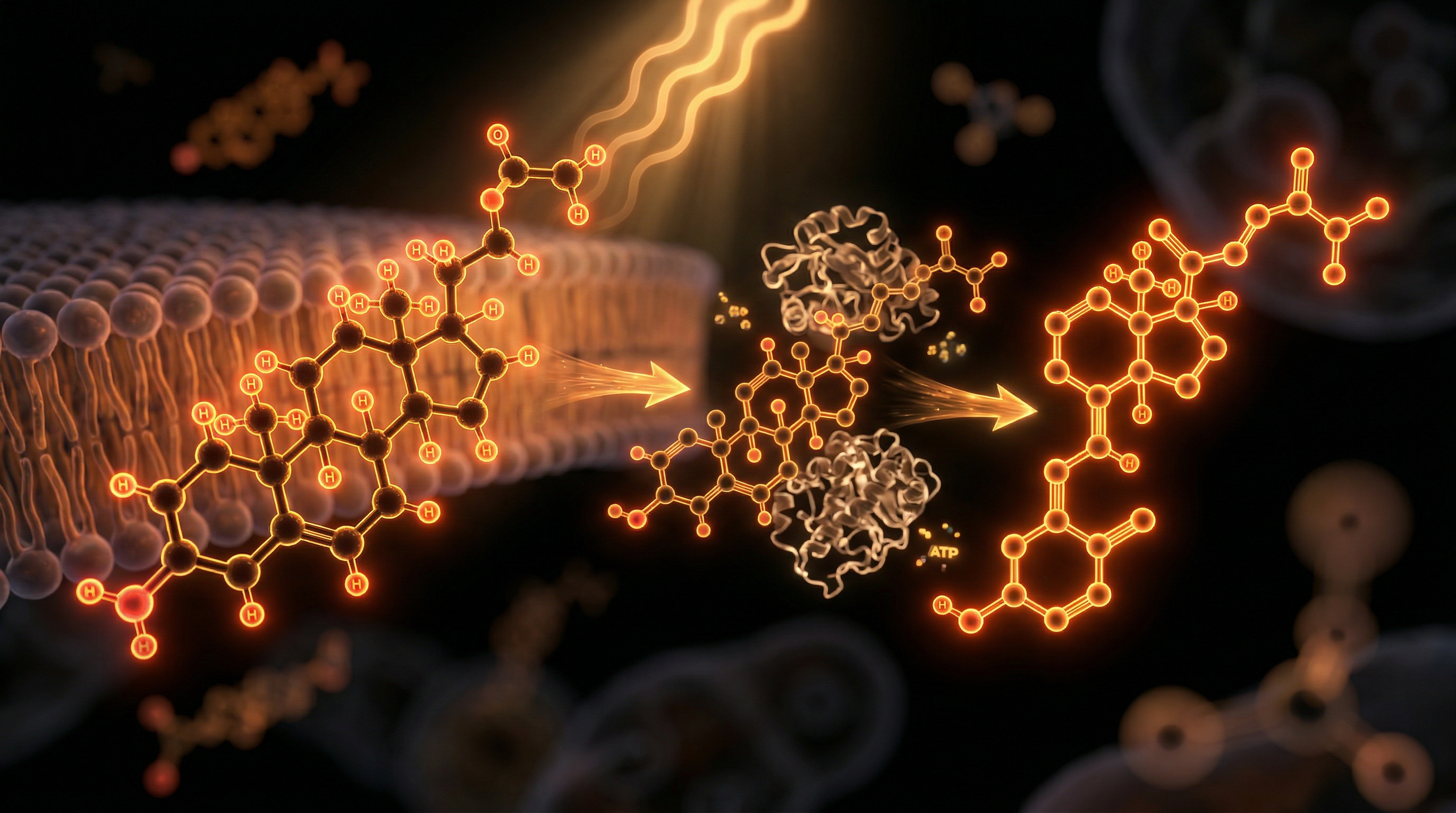
The Photochemical Cascade
The process begins with 7-dehydrocholesterol, a precursor molecule found in the plasma membranes of skin cells. When the skin is exposed to Ultraviolet B (UVB) radiation—specifically wavelengths between 290 and 315 nanometres—the B-ring of this cholesterol precursor is broken, forming pre-vitamin D3.
Within hours, through a process of thermal isomerisation (driven by body heat), this unstable pre-vitamin D3 is converted into cholecalciferol (Vitamin D3). It is then picked up by the Vitamin D Binding Protein (VDBP) and transported to the liver.
The Two-Stage Activation
Vitamin D3 in itself is biologically inert. It must undergo two hydroxylations to become the "master key" of the human genome:
- —In the Liver: The enzyme CYP2R1 adds a hydroxyl group to create 25-hydroxyvitamin D [25(OH)D], also known as calcidiol. This is the form measured in blood tests to determine status.
- —In the Kidneys: The enzyme CYP27B1 performs the final conversion into 1,25-dihydroxyvitamin D [1,25(OH)2D], known as calcitriol. This is the active, hormonal form that exerts systemic effects.
The Physics of the 51st Parallel
The "51st Parallel Problem" is rooted in atmospheric physics. For UVB photons to reach the skin, they must pass through the Earth's atmosphere. When the sun is high in the sky (the zenith), the path is direct. However, at latitudes above 51°N, the sun stays low on the horizon during the winter months (October to March).
At these angles, the UVB photons must travel through a much thicker layer of the ozone layer. Due to Rayleigh scattering, the atmosphere effectively filters out almost 100% of the UVB radiation before it reaches the ground. Even on a "sunny" day in a British January, you could stand outside naked for eight hours and produce zero Vitamin D.
---
Mechanisms at the Cellular Level
While mainstream medicine focuses on calcium absorption, the reality of Vitamin D is far more profound. It acts as a seco-steroid hormone, similar in structure to oestrogen or testosterone, and its receptors (VDR) are located in the nuclei of almost every cell in the human body.
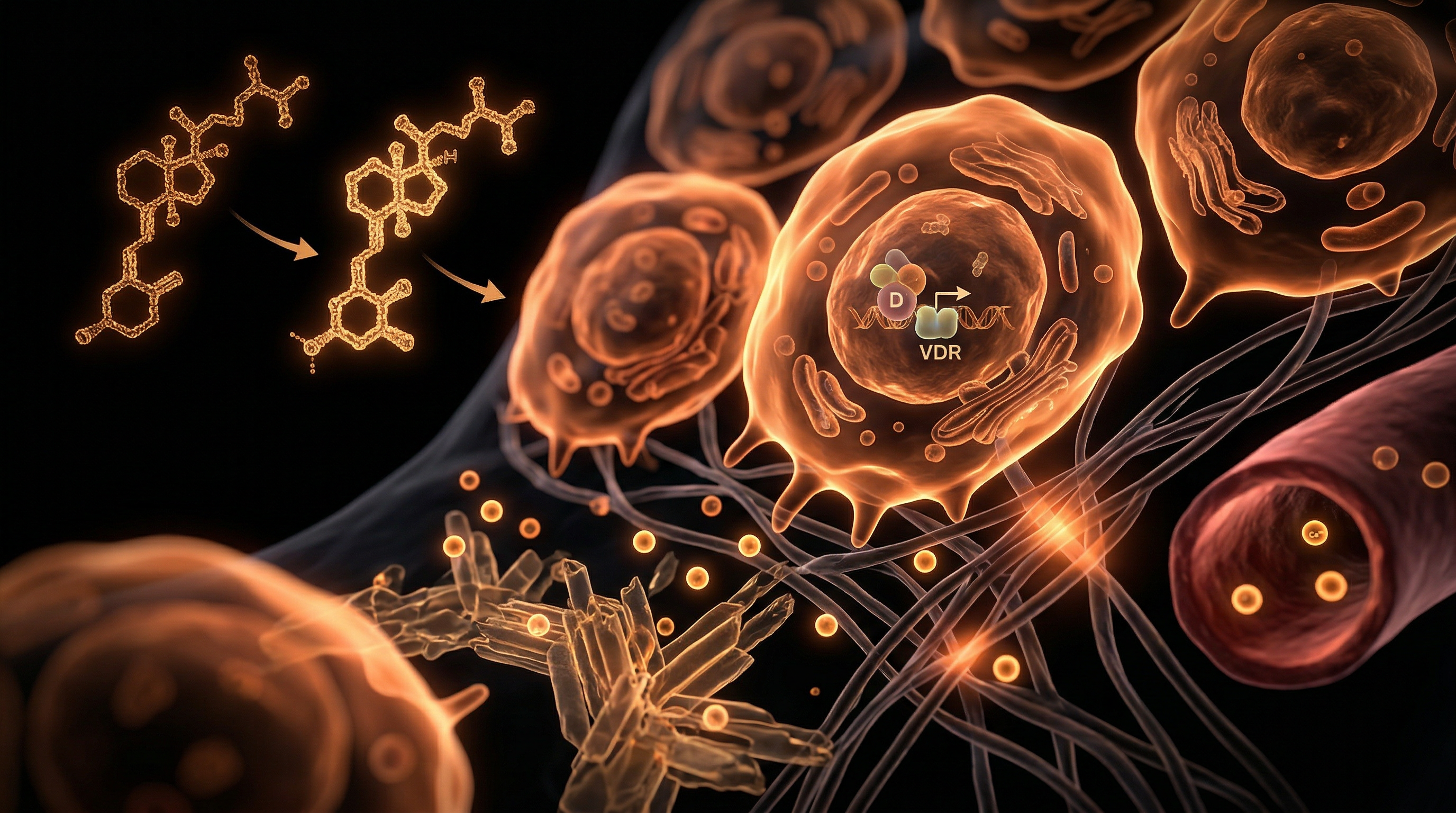
Genomic Governance
Once calcitriol binds to the VDR, it forms a complex with the RXR (Retinoid X Receptor). This complex then moves into the cell nucleus and binds to specific DNA sequences called Vitamin D Response Elements (VDREs).
- —Vitamin D is estimated to directly or indirectly regulate the expression of over 2,000 genes.
- —This represents roughly 10% of the entire human genome.
- —It controls genes involved in cell proliferation, differentiation, and apoptosis (programmed cell death).
The Immune Sentinel
Perhaps the most critical cellular mechanism is the role of Vitamin D in the innate immune system. Our white blood cells—specifically macrophages and monocytes—possess the enzyme necessary to convert 25(OH)D into the active hormonal form *locally*.
When a pathogen is detected, Vitamin D triggers the production of cathelicidins and defensins. These are endogenous antimicrobial peptides—essentially "natural antibiotics"—that can puncture the membranes of bacteria and the envelopes of viruses. Without sufficient Vitamin D, the immune system is essentially "unarmed" against respiratory infections.
Autocrine vs. Endocrine
Crucially, we now know that Vitamin D metabolism is not just a "kidney-to-blood" system (the endocrine pathway). Most tissues, including the breast, colon, and prostate, have their own local machinery to activate Vitamin D (the autocrine pathway). This suggests that maintaining high circulating levels of 25(OH)D is vital for preventing the "biological glitches" that lead to malignancy.
KEY TERM: Calcitriol. The most potent steroid hormone in the human body, capable of switching off pro-inflammatory cytokines and preventing "cytokine storms."
---
Environmental Threats and Biological Disruptors
The 51st parallel geography is the primary antagonist, but several modern environmental factors act as "force multipliers" for the deficiency.
The "Indoor Ape" Phenomenon
Humans are biologically designed to be outdoors. The modern shift to an indoor-centric lifestyle—offices, gyms, and climate-controlled homes—means that even during the "Vitamin D Summer" (May to August), many British citizens remain deficient. Glass windows are a major culprit; they allow UVA radiation through (which ages the skin and can cause cancer) but block UVB radiation entirely.
The Adipose Trap
The UK is currently facing an obesity epidemic. Because Vitamin D is lipophilic (fat-soluble), it is easily sequestered in adipose tissue. In overweight or obese individuals, Vitamin D produced in the skin or taken as a supplement is "sucked up" by fat cells and stored, preventing it from entering the bloodstream to be used by the liver and kidneys. This means obese individuals may require 2 to 3 times the standard dose to achieve the same blood levels as a lean person.
Air Pollution and Aerosols
In urban centres like London, Birmingham, and Manchester, atmospheric pollutants such as nitrogen dioxide and particulate matter further scatter UVB rays. Furthermore, the "urban heat island" effect does nothing for Vitamin D synthesis, as it is light, not heat, that drives the reaction.
The Magnesium Co-factor
A silent disruptor of the Vitamin D pathway is the widespread deficiency in Magnesium. All the enzymes that metabolise Vitamin D (CYP2R1, CYP27B1) require magnesium as a co-factor. If you are magnesium-deficient—common in the UK due to soil depletion—you cannot activate the Vitamin D you are taking. It remains stored and "clogs" the system, potentially leading to calcium deposits in the arteries rather than the bones.
---
The Cascade: From Exposure to Disease
When Vitamin D levels fall, the body enters a state of "metabolic emergency." The consequences are not immediate; they are a slow, eroding cascade that manifests as chronic illness.
Skeletal Integrity: The Tip of the Iceberg
The most well-known effect is secondary hyperparathyroidism. When Vitamin D is low, the body cannot absorb calcium from the gut. To keep blood calcium levels stable (which is essential for heart function), the parathyroid glands secrete hormones that "strip" calcium from the bones.
- —In children, this causes Rickets (bowed legs).
- —In adults, it causes Osteomalacia (soft bones) and eventually Osteoporosis.
- —Chronic "aching bones" and lower back pain are often misdiagnosed when they are actually symptoms of osteomalacia.
The Autoimmune Connection
There is a direct correlation between latitude and the prevalence of Multiple Sclerosis (MS). The further one lives from the equator, the higher the risk. Vitamin D is essential for the development of T-Regulatory cells, the "peacekeepers" of the immune system that prevent it from attacking the body’s own tissues. Deficiency leads to an "unregulated" immune system, contributing to:
- —Rheumatoid Arthritis
- —Type 1 Diabetes
- —Crohn’s Disease
- —Hashimoto’s Thyroiditis
Cognitive and Mental Health
The "Winter Blues" or Seasonal Affective Disorder (SAD) is often dismissed as a psychological response to grey weather. In reality, it is a neurochemical response to Vitamin D deficiency. Vitamin D receptors are concentrated in the hippocampus and the cerebellum. Vitamin D is a key regulator of the enzyme tryptophan hydroxylase, which converts the amino acid tryptophan into serotonin—the "feel-good" neurotransmitter. Without it, the brain literally cannot produce enough serotonin to maintain a stable mood.
---
What the Mainstream Narrative Omits
As a researcher for INNERSTANDING, it is my duty to expose the gaps in the official narrative. Public health guidelines in the UK are not just conservative; they are arguably negligent.
The RDA Scam
The current UK Recommended Dietary Allowance (RDA) for Vitamin D is a paltry 400 IU (10 micrograms) per day. This figure was originally designed to prevent the most extreme cases of rickets in children. It was never intended to support optimal immune function, genomic stability, or cancer prevention.
- —Research has shown that a "statistical error" in the original calculations for the RDA resulted in a recommendation that is nearly 10 times lower than what is actually required for the average adult to reach healthy blood levels.
The Toxicity Myth
There is a persistent fear-mongering regarding "Vitamin D toxicity" (Hypervitaminosis D). While it is possible to take too much, toxicity is extremely rare and usually requires doses exceeding 50,000 IU daily for months. By keeping the RDA low under the guise of "safety," authorities ensure the population remains in a state of sub-optimal health, making them more reliant on pharmaceutical interventions for the diseases that deficiency causes.
Big Pharma and the "Symptom Economy"
If the British population were to achieve optimal Vitamin D status (above 100 nmol/L), the economic impact on the pharmaceutical industry would be catastrophic.
- —Sales of anti-depressants would plummet.
- —The burden of chronic respiratory infections would diminish.
- —The incidence of certain cancers (colorectal, breast) could be reduced by up to 50%.
Vitamin D is off-patent, cheap, and cannot be branded as a "blockbuster drug." There is no financial incentive for the "Mainstream Medical Industrial Complex" to promote its widespread use at therapeutic doses.
CALLOUT FACT: A study published in the *British Medical Journal* estimated that Vitamin D supplementation could prevent over 3 million cases of the common cold and flu in the UK each year.
---
The UK Context
The UK’s unique combination of latitude, climate, and demographics creates a "perfect storm" for Vitamin D deficiency.
The Scottish Extremity
While the 51st parallel is a problem for London, those in Scotland (55°N to 60°N) face an even more dire situation. Scotland has some of the highest rates of MS and bowel cancer in the world. The "Vitamin D Winter" in Aberdeen or the Shetland Islands can last up to seven months.
Melanin: The Double-Edged Sword
One of the most suppressed aspects of the UK's Vitamin D crisis is its impact on BAME (Black, Asian, and Minority Ethnic) communities. Melanin is a natural sunscreen; it evolved to protect humans in equatorial regions from *too much* UV radiation. In the low-UV environment of the UK, melanin acts as a barrier to synthesis. A person with dark skin may require 3 to 5 times longer in the sun to produce the same amount of Vitamin D as a fair-skinned person. Consequently, deficiency rates among Black Britons are staggering, contributing significantly to health inequalities, particularly in cardiovascular and maternal health.
The "British Summer" Fallacy
Even during the summer, the UK’s weather is notoriously fickle. Cloud cover can reduce UVB intensity by 50% to 90%. Furthermore, the national obsession with "sun safety"—encouraged by dermatologists who focus solely on skin cancer while ignoring systemic hormone health—means that many people cover up or apply high-SPF sunscreens the moment the sun appears, effectively halting any chance of Vitamin D synthesis.
---
Protective Measures and Recovery Protocols
If you live at or above the 51st parallel, you cannot rely on "nature" to provide your Vitamin D. You must take an active, scientific approach to your endocrine health.
1. Know Your Numbers
Do not guess. A 25(OH)D blood test is essential.
- —NHS "Normal": Often 50 nmol/L (This is the bare minimum to prevent bone disease).
- —INNERSTANDING Optimal: 100 nmol/L to 150 nmol/L (This is the range where immune and genomic protection is maximised).
- —Note on Units: Ensure you are reading nmol/L (UK standard) and not ng/mL (US standard). (To convert ng/mL to nmol/L, multiply by 2.5).
2. Strategic Supplementation
For most adults in the UK, 400 IU is useless. Depending on your baseline, a daily dose of 2,000 IU to 5,000 IU of Vitamin D3 (Cholecalciferol) is often required to maintain optimal levels.
- —Avoid Vitamin D2 (Ergocalciferol): This is the plant-based version often prescribed by GPs. It is significantly less bioavailable and less effective at raising long-term blood levels than D3.
3. The Synergy: D3 + K2 + Magnesium
Never take Vitamin D in isolation. It works as part of a biological triad:
- —Vitamin K2 (MK-7): This is the "traffic cop" for calcium. Vitamin D increases calcium absorption; K2 ensures that calcium goes into the bones and teeth and stays *out* of the arteries and soft tissues (preventing calcification).
- —Magnesium: As discussed, magnesium is required to activate Vitamin D. Take 300-400mg of a highly bioavailable form like Magnesium Glycinate or Malate.
4. Maximising the "Solar Window"
During the months of May to August, the sun is high enough.
- —The Shadow Rule: If your shadow is shorter than you are, the sun is high enough to produce Vitamin D. If your shadow is longer, the UVB is being filtered out.
- —Exposure: Aim for 15-20 minutes of sun on large areas of skin (arms, back, legs) *without* sunscreen during midday hours. Once the skin begins to turn the slightest shade of pink, synthesis has peaked, and you should cover up or apply protection.
5. Diet is Not Enough
It is a common misconception that you can get enough Vitamin D from oily fish or fortified cereals. You would need to eat roughly 10-15 eggs or several cans of sardines *every single day* to meet even a modest requirement. In the UK, supplementation is not an "option"—it is a physiological necessity for survival.
---
Summary: Key Takeaways
The 51st Parallel Problem is a silent architect of British ill-health. We have moved from being sun-drenched primates to "biologically starved" indoor dwellers in a matter of centuries, and our bodies are paying the price.
- —The Solar Deficit: Between October and March, Vitamin D synthesis in the UK is physically impossible due to the angle of the sun and atmospheric scattering.
- —Genomic Regulation: Vitamin D is a seco-steroid hormone that controls over 2,000 genes. Deficiency is not just a "vitamin low"—it is a systemic "software failure" in our DNA.
- —The Immune Crisis: Without Vitamin D, the body cannot produce cathelicidin, leaving us vulnerable to viruses and autoimmune dysfunction.
- —The Latitude Risk: The further north you live (e.g., Scotland), and the more melanin your skin contains, the greater the threat to your health.
- —Optimal Protocol: Move beyond the 400 IU RDA. Aim for blood levels of 100-150 nmol/L through D3 supplementation, always paired with Vitamin K2 and Magnesium.
The "Vitamin D Crisis" is perhaps the most easily solved problem in modern medicine, yet it remains unaddressed because the solution—sunlight and a cheap supplement—offers no profit to the powers that be. To live healthily above the 51st parallel is to live in defiance of the current environmental and institutional status quo.
It is time to take control of your own biochemistry. The sun may be missing from our skies, but its biological proxy is within our reach.
*
"References & Further Reading:"
- —*Holick, M. F. (2007). Vitamin D deficiency. New England Journal of Medicine.*
- —*Heaney, R. P. (2013). Vitamin D: criteria for sufficiency. Scientific World Journal.*
- —*Martineau, A. R., et al. (2017). Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis. BMJ.*
- —*Scientific Advisory Committee on Nutrition (SACN) - Vitamin D and Health Report.*
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Vitamin D Crisis: The 51st Parallel Problem"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper