The Central Sensitization Myth: Why the NHS Fails Chronic Pain Patients
Modern pain science reveals that the nervous system can become trapped in a loop of high alert, a biological process known as central sensitization. Conventional UK treatments often ignore these neurological shifts, opting instead for symptomatic relief that fails to address the underlying neural plasticity.
Overview
The landscape of British healthcare is currently haunted by a silent epidemic, one that traditional diagnostic frameworks are patently ill-equipped to handle. We are witnessing the catastrophic failure of the biomedical model in the face of chronic primary pain. While the National Health Service (NHS) remains tethered to an antiquated "structural-pathology" mindset—searching for a slipped disc, a torn ligament, or a degenerating joint to explain every agony—modern biological research has moved decades ahead. We now know that in millions of patients, the source of pain is no longer in the tissues of the body, but in the maladaptive plasticity of the nervous system.
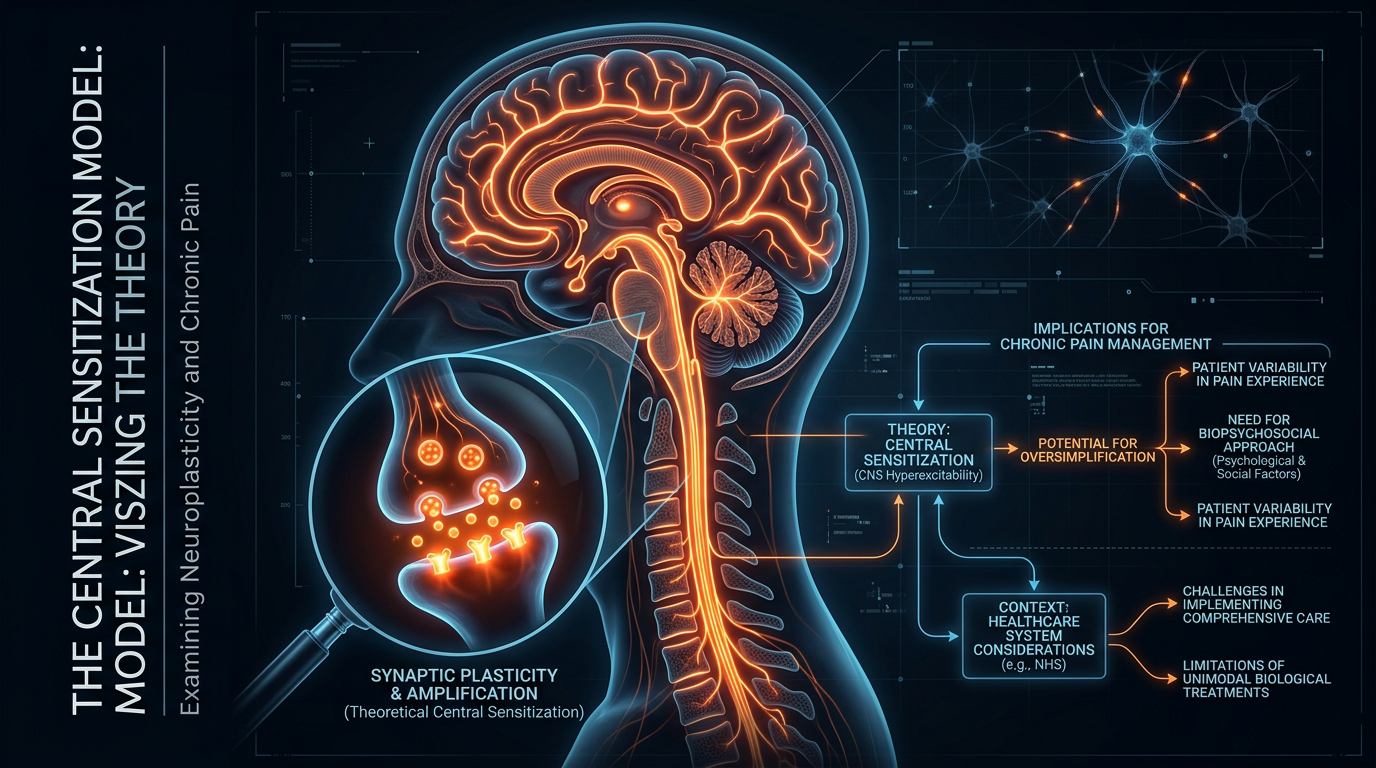
This phenomenon is known as Central Sensitization (CS). It is a state where the central nervous system (CNS) remains in a persistent state of high reactivity. The "alarm system" of the body has not only been triggered; the alarm has broken, the volume is stuck at maximum, and the threshold for activation has plummeted.
According to the British Pain Society, approximately 28 million adults in the UK are living with chronic pain, yet the average GP receives less than 12 hours of specific pain management training during their entire medical education.
The "Myth" mentioned in our title refers not to the existence of Central Sensitization—which is a robustly documented biological fact—but to the myth of the "Broken Body" that the NHS continues to propagate. By focusing on symptomatic relief via analgesics and surgical interventions, the mainstream narrative ignores the underlying neural circuitry. This article serves as a comprehensive interrogation of why the UK’s approach to chronic pain is fundamentally flawed and how a deeper understanding of neuroplasticity offers the only viable path to recovery.
##
The Biology — How It Works
To understand Central Sensitization, one must first distinguish between nociception and pain. Nociception is the physiological process of encoding noxious stimuli (mechanical, thermal, or chemical threats). Pain, however, is a conscious experience—a subjective output of the brain intended to protect the organism. In a healthy system, these two are coupled: you burn your hand, nociceptors fire, the brain interprets the signal as a threat, and you feel pain.
In the sensitized patient, this coupling is severed. Central Sensitization represents a functional change in the somatosensory system. When the nervous system is subjected to prolonged stress or repeated injury, it undergoes a process of "wind-up." The neurons in the spinal cord begin to respond more vigorously to every incoming signal.
The Amplification Loop
Imagine a guitar amplifier. In a normal state, the gain is set to 3. You pluck a string (a minor injury), and a moderate sound comes out. In a state of Central Sensitization, the "gain" of the nervous system is turned up to 11. Now, even a light breeze across the strings produces a deafening, distorted roar. This is the biological reality for the chronic pain sufferer: the brain has become exquisitely sensitive to inputs that it would previously have ignored.
The Breakdown of Thresholds
There are two primary clinical hallmarks of this biological shift:
- —Hyperalgesia: An increased response to a stimulus that is normally painful. A small pinch feels like a knife wound.
- —Allodynia: Pain due to a stimulus that does not normally provoke pain. The touch of clothing on the skin or a cool breeze becomes excruciating.
The NHS typically treats these symptoms as "unexplained" or "psychosomatic" when scans fail to show tissue damage. In reality, they are the predictable outcomes of a neuroplastic system that has over-learned the lesson of protection.
##
Mechanisms at the Cellular Level
As a researcher, one must look beneath the surface of the skin and into the synaptic clefts of the dorsal horn of the spinal cord. This is where the tragedy of chronic pain is written at a molecular level.
Long-Term Potentiation (LTP)
Much like the process of forming a memory, the nervous system "remembers" pain through Long-Term Potentiation. When nociceptive pathways are repeatedly activated, the synaptic connections between the peripheral nerves and the spinal cord neurons are strengthened. This involves an increase in the number of receptors on the postsynaptic membrane, making it easier for future signals to cross the gap.
The Role of Glutamate and NMDA Receptors
The primary excitatory neurotransmitter involved in this process is glutamate. In a sensitized state, there is an excessive release of glutamate, which binds to NMDA (N-methyl-D-aspartate) receptors. Under normal conditions, these receptors are blocked by a magnesium ion. However, during sustained firing, the magnesium is dislodged, allowing a flood of calcium into the neuron. This calcium influx triggers a cascade of intracellular events that permanently alter the neuron's gene expression, making it "hyperexcitable."
Glial Cell Activation: The Dark Horse of Pain
For decades, we believed neurons were the only players in pain. We were wrong. Microglia and astrocytes—the immune cells of the brain—play a pivotal role. When the system is under threat, these cells activate and release pro-inflammatory cytokines such as IL-1β, IL-6, and TNF-alpha. These chemicals bathe the neurons, further lowering their firing threshold.
Scientific Fact: Research indicates that activated glia can increase the sensitivity of pain-transmitting neurons by up to tenfold, effectively turning a localized injury into a systemic neurological condition.
This "neuro-inflammation" is rarely, if ever, measured or addressed in a standard NHS pain clinic. Instead, patients are given Ibuprofen, which targets peripheral inflammation but does absolutely nothing to calm the "cytokine storm" happening within the central nervous system.
##
Environmental Threats and Biological Disruptors
Central Sensitization does not occur in a vacuum. It is the result of a biological system being pushed beyond its allostatic load—the wear and tear on the body which accumulates as an individual is exposed to repeated or chronic stress.
The Modern British Lifestyle as a Sensitizer
The UK environment is uniquely conducive to nervous system dysregulation. Several factors act as biological disruptors:
- —Circadian Mismatch: The prevalence of blue light and shift work in the UK workforce disrupts melatonin production. Melatonin is a potent antioxidant and neuroprotector; its absence leaves the CNS vulnerable to oxidative stress and sensitization.
- —Dietary Inflammagens: The high consumption of ultra-processed foods (UPFs) in the UK—accounting for over 50% of the national diet—drives systemic inflammation. This systemic state "primes" the microglia, making Central Sensitization more likely.
- —Sedentary Behaviour: Movement is a natural "top-down" inhibitor of pain. The UK’s increasingly sedentary lifestyle removes the mechanoreceptor input that helps the brain "gate" or suppress pain signals.
Psychological Stress as Biological Input
We must move past the "it's all in your head" vs. "it's all in your body" dichotomy. The brain is an organ of the body. Psychosocial stressors—job insecurity, social isolation, and the "cost of living" crisis—are processed by the amygdala and the anterior cingulate cortex. These brain regions are directly wired into the pain-processing centres. If the brain perceives the *environment* as unsafe, it will maintain the nervous system in a state of high alert, perpetuating the sensitization loop.
##
The Cascade: From Exposure to Disease
The progression from an acute injury to a chronic, sensitized state is a predictable biological cascade that the NHS fails to interrupt.
Stage 1: The Inciting Incident
It begins with a peripheral insult—a back strain, a post-viral syndrome, or even a period of intense emotional trauma. At this stage, the pain is purely "nociceptive."
Stage 2: Peripheral Sensitization
The area around the injury becomes tender. Inflammatory mediators like prostaglandins and bradykinin lower the threshold of the local nerve endings. This is a normal part of healing.
Stage 3: The "Wind-Up" Phenomenon
If the threat is not resolved—either because the injury is persistent or because the patient is under high stress—the spinal cord begins to "wind up." This is the transition from peripheral to central sensitization. The spinal cord starts sending signals to the brain even in the absence of a strong peripheral stimulus.
Stage 4: Cortical Remapping
In the final and most devastating stage, the brain itself changes. In chronic pain patients, the somatosensory cortex undergoes "smudging." The distinct areas of the brain dedicated to different body parts begin to overlap. If the brain "smudges" the map of the back, it loses the ability to precisely locate sensations, resulting in a diffuse, spreading ache that is difficult for the patient to describe.
Evidence from functional MRI (fMRI) studies shows that in patients with chronic low back pain, the grey matter density in the prefrontal cortex—the area responsible for emotional regulation and decision-making—actually decreases, a process often referred to as "brain shrinking."
##
What the Mainstream Narrative Omits
The NHS narrative regarding chronic pain is built on a foundation of structuralism. If you have back pain, they give you an X-ray. If the X-ray shows a bulging disc, they blame the disc. If the X-ray is clear, they imply you are "making it up" or suffering from "low mood."
Both of these conclusions are scientifically bankrupt.
The MRI Deception
Large-scale studies have shown that 30% of 20-year-olds and 80% of 50-year-olds with *no pain at all* have disc bulges or "degenerative changes" on their MRIs. These are normal "wrinkles on the inside." By attributing pain to these structural findings, the NHS inadvertently increases the patient's sensitization. The patient is told their spine is "crumbling" or "unstable." This induces a "Nocebo" effect—the biological opposite of a placebo—where the fear of movement further sensitizes the nervous system.
The Failure of the Pharmacological Hammer
The primary "tools" used by the NHS are:
- —NSAIDs (Ibuprofen): Ineffective for central sensitization.
- —Opioids (Morphine, Codeine): Not only are they ineffective for CS, but they can cause Opioid-Induced Hyperalgesia (OIH), where the drug actually makes the nervous system *more* sensitive over time.
- —Gabapentinoids (Pregabalin/Gabapentin): Often prescribed as a "catch-all" for nerve pain, they have significant side effects and a high "number needed to treat" (NNT), meaning they fail for the vast majority of patients.
The mainstream narrative omits the fact that chronic pain is a learning disorder of the nervous system. You cannot fix a software problem (central sensitization) by trying to replace the hardware (surgery) or by pouring chemicals over the keyboard (medication).
##
The UK Context
The failure of the NHS in this arena is not merely a scientific error; it is a systemic, structural failure of the British medical establishment.
The 10-Minute Consultation
The GP system is designed for acute issues—infections, broken bones, and straightforward diagnoses. A 10-minute slot is insufficient to unravel the complex web of biological, psychological, and social factors that maintain Central Sensitization. Consequently, GPs reach for the prescription pad as the fastest way to "help" the patient out of the door.
The Waiting List Crisis
When a patient is referred to a pain clinic, the wait can be anywhere from 18 months to two years. During this time, the neural pathways of pain are being reinforced. Every month that passes without effective intervention allows the Central Sensitization to become more "hard-wired."
A 2022 report found that in some parts of the UK, the wait for a multidisciplinary pain management programme exceeds 1,000 days. In biological terms, this is a death sentence for the patient's chances of a swift recovery.
The North-South Pain Divide
There is a stark geographic disparity in chronic pain outcomes. The "Rust Belt" of Northern England—areas with higher levels of deprivation and industrial decay—has significantly higher rates of opioid prescriptions and chronic disability. This highlights that Central Sensitization is as much a sociological issue as a biological one. The NHS, however, is not structured to treat social isolation or economic despair, even though these are direct drivers of nervous system "high alert" states.
##
Protective Measures and Recovery Protocols
If the NHS is failing, how does one actually treat a sensitized nervous system? Recovery requires a shift from "Managing Pain" to "Retraining the Nervous System."
1. Pain Neuroscience Education (PNE)
The first step in recovery is understanding that "Pain does not equal damage." When a patient truly understands that their pain is a result of a sensitive alarm system rather than a "broken" body, their threat level drops. This cognitive shift can actually dampen the activity of the amygdala and reduce the output of the "danger" signals.
2. Graded Motor Imagery (GMI)
To address the "smudging" of the brain maps, we use GMI. This involves three stages:
- —Laterality Training: Identifying left vs. right limbs to re-engage the brain's maps.
- —Explicit Imagery: Imagining movement without actually moving, which activates the motor cortex without triggering the pain-sensing neurons.
- —Mirror Therapy: Using a mirror to "trick" the brain into seeing a painful limb moving comfortably.
3. Sensory Desensitization
For patients with allodynia (pain from touch), we use a protocol of graduated textures. Starting with something very soft (like silk) and moving toward rougher textures (like wool or a brush), the patient "re-teaches" the nervous system that these stimuli are safe.
4. Vagus Nerve Stimulation and Lifestyle Medicine
The Vagus nerve is the "brake" of the nervous system. By utilizing deep diaphragmatic breathing, cold water immersion, and specific nutritional protocols (high-DHA omega-3s to resolve neuro-inflammation), we can shift the body from a sympathetic ("fight or flight") state to a parasympathetic ("rest and digest") state.
5. Movement as Medicine
The goal is Graded Exposure. We find the "edge" of the patient's tolerance—the point where they feel sensation but not a "flare-up"—and slowly expand that boundary. This is not "No Pain, No Gain." It is "Know Pain, No Fear."
##
Summary: Key Takeaways
The current NHS approach to chronic pain is a relic of 20th-century medicine being applied to 21st-century neurological crises. We must move beyond the "Myth of the Broken Body" and embrace the "Reality of the Plastic Brain."
- —Central Sensitization is a Real Biological Change: It involves the literal rewiring of the spinal cord and brain, making the system hyperexcitable.
- —The NHS Model is Flawed: Its reliance on structural imaging (MRIs) and symptomatic medication (opioids) often makes the problem worse by inducing fear and OIH.
- —Neuroplasticity is the Key: Just as the nervous system can learn pain, it can "unlearn" it through targeted, evidence-based interventions.
- —Holistic Biology is Required: We cannot ignore the impact of the UK's environment—diet, stress, and lifestyle—on the sensitivity of our immune and nervous systems.
- —The Patient is Not Broken: The pain is real, but it is an "output" of a system that is trying to protect the individual. The goal of modern medicine should be to signal safety, not to perform more surgeries.
The failure of the NHS is a failure of education and systemic inertia. For the 28 million Britons suffering, the path forward lies in the very science the mainstream ignores: the incredible, adaptable, and ultimately healable nature of the human nervous system. We do not need more painkillers; we need Neuroplastic Rehabilitation. It is time to turn down the volume.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
RABBIT HOLE
Follow the biological thread deeper