The Hidden Epidemic of Subclinical Hypothyroidism and Why UK Labs Miss It
Millions of people suffer from thyroid symptoms while being told their blood tests are 'normal.' This article explains the flaws in standard thyroid testing and how to identify true thyroid dysfunction.

Overview
The modern landscape of British healthcare is haunted by a silent, invisible spectre: the epidemic of subclinical hypothyroidism. Across the United Kingdom, millions of individuals—predominantly women, though men are increasingly affected—are trapped in a biological purgatory. They present to their GPs with a debilitating constellation of symptoms: chronic fatigue that no amount of sleep can cure, unexplained weight gain, thinning hair, cognitive "brain fog," brittle nails, and a pervasive sensitivity to the cold. Yet, after a standard blood test, they are dismissed with a clean bill of health.
"Your results are within the normal range," is the standard refrain. This sentence has become a death knell for vitality in the UK.
At INNERSTANDING, we do not accept the "normal" label when the biological reality dictates otherwise. The truth is that the current diagnostic framework for thyroid health in the UK is fundamentally flawed, outdated, and scientifically reductive. It relies almost exclusively on a single biomarker—Thyroid Stimulating Hormone (TSH)—while ignoring the complex intracellular machinery that actually dictates metabolic rate. By focusing on the messenger (TSH) rather than the message (T3 levels at the cellular receptor), mainstream medicine misses the vast majority of thyroid dysfunction.
This article serves as a comprehensive exposé on the systemic failure to diagnose thyroid conditions. We will peel back the layers of endocrine physiology, explore the environmental toxins poisoning our British soil and water, and reveal why the "normal" reference ranges used by the NHS are not a measure of health, but a statistical average of an increasingly sick population. This is the hidden epidemic of the subclinical, and it is time for the biological truth to be heard.
Statistics suggest that as many as 1 in 4 people in the UK may be suffering from some form of thyroid dysregulation, yet only a fraction receive an accurate diagnosis or effective treatment.
##
##
The Biology — How It Works

Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin
A high-potency 12% Lugol’s Iodine solution designed to support thyroid health, metabolic energy, and cognitive clarity. This traditional aqueous blend provides both iodine and potassium iodide to ensure your body has the essential elements needed for hormonal balance and healthy skin.
Vetting Notes
Pending
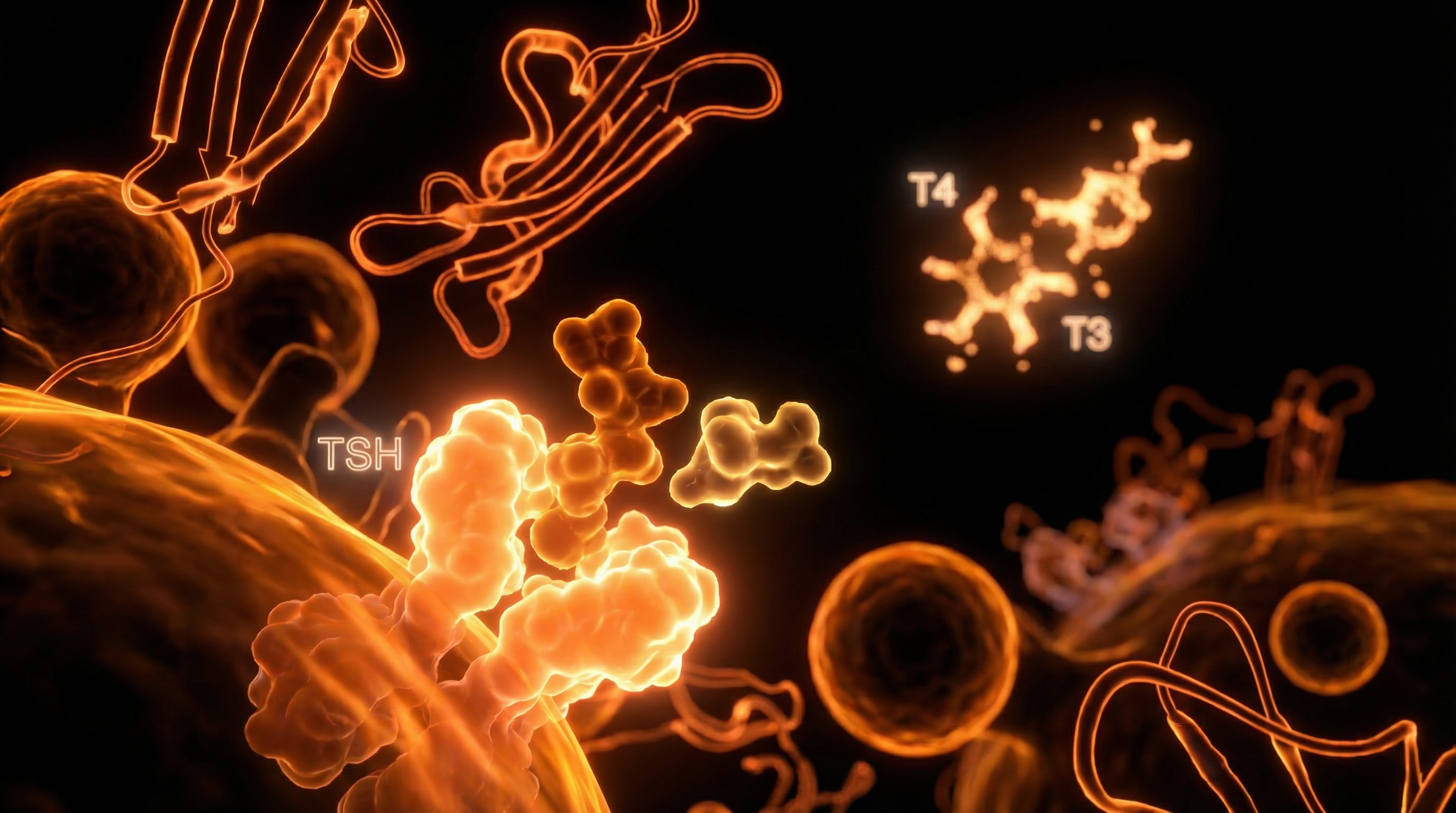
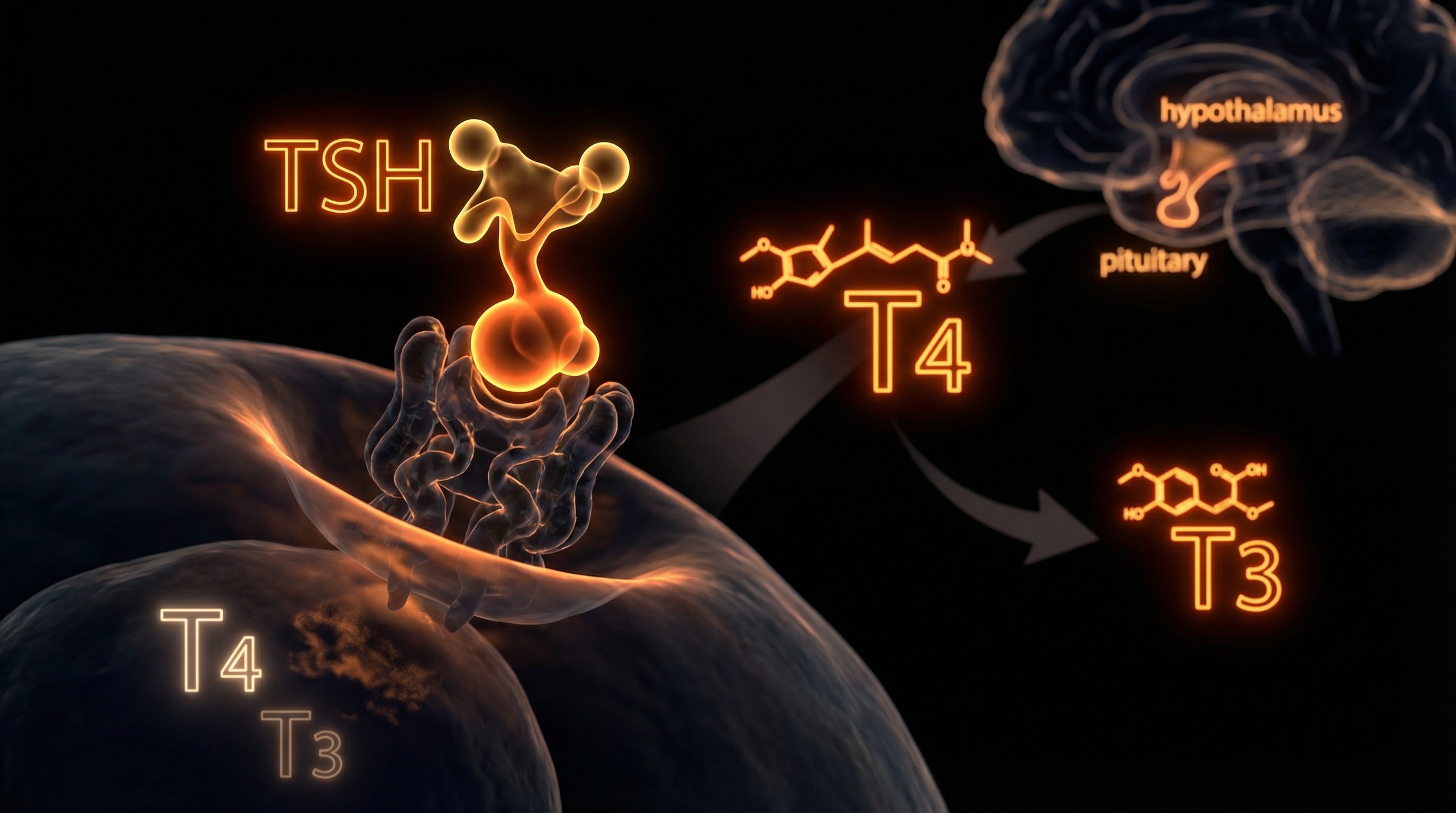
To understand why the system is failing, we must first master the elegance of the Hypothalamic-Pituitary-Thyroid (HPT) Axis. The thyroid is a small, butterfly-shaped gland situated at the base of the neck, but its influence is titanic. It acts as the "master controller" of metabolism, governing the rate at which every cell in the human body consumes oxygen and produces energy (ATP).
The process begins in the brain. The hypothalamus monitors the blood for circulating levels of thyroid hormones. When levels drop, it releases Thyrotropin-Releasing Hormone (TRH). This signals the anterior pituitary gland to secrete Thyroid Stimulating Hormone (TSH). TSH then travels to the thyroid gland, binding to receptors on the follicular cells to stimulate the production of hormones.
The thyroid primarily produces two hormones:
- —Thyroxine (T4): This is the pro-hormone. It contains four iodine atoms and is relatively inactive. It accounts for about 93% of the gland's output.
- —Triiodothyronine (T3): This is the biologically active hormone. It contains three iodine atoms and is roughly five times more potent than T4. Only about 7% of the hormone produced directly by the thyroid is T3.
The synthesis of these hormones is a feat of bio-engineering. It requires the amino acid L-tyrosine and the mineral iodine. Through a process called organification, the enzyme Thyroid Peroxidase (TPO) attaches iodine to a protein called thyroglobulin. This creates Monoiodotyrosine (MIT) and Diiodotyrosine (DIT), which are then "coupled" to form T3 and T4.
However, the production of hormone in the gland is only the beginning. For you to feel energetic, clear-headed, and warm, that T4 must be transported through the blood (bound to Thyroxine-Binding Globulin) and then converted into T3 within the peripheral tissues—mainly the liver, kidneys, and gut.
##
##
Mechanisms at the Cellular Level
The "standard" medical view stops at the blood level. If there is enough T4 in the blood and the TSH is "low enough," the doctor assumes everything is fine. But biological reality occurs at the mitochondrial level.
The Deiodinase System
The conversion of T4 to T3 is managed by a group of enzymes called deiodinases (D1, D2, and D3). These enzymes are selenoproteins, meaning they are strictly dependent on the mineral selenium.
- —Type 1 Deiodinase (D1): Located primarily in the liver and kidneys, responsible for the majority of circulating T3.
- —Type 2 Deiodinase (D2): Located in the brain, pituitary, and intracellularly, providing local T3 to tissues.
- —Type 3 Deiodinase (D3): The "inactivator." It converts T4 into Reverse T3 (rT3) and T3 into T2.
Reverse T3 is a critical but ignored player. It is a structural isomer of T3, meaning it looks like T3 and can plug into the T3 receptor site, but it lacks the "key" to turn on the metabolic engine. Think of rT3 as a broken key in a lock; it prevents the working key (T3) from entering. Under conditions of high stress, chronic inflammation, or nutrient deficiency, the body shifts production away from active T3 and toward rT3 as a survival mechanism to slow down metabolism and conserve energy.
The Sodium-Iodide Symporter (NIS)
At the cellular entry point, the Sodium-Iodide Symporter (NIS) is a transmembrane glycoprotein that mediates the transport of iodide into the thyroid follicular cells. This pump is the gatekeeper. If the NIS is inhibited by environmental toxins or heavy metals, the entire chain of hormone production collapses before it even begins.
Mitochondrial Transcription
Once T3 enters a cell, it must travel to the nucleus and bind to Thyroid Hormone Receptors (TRs). This complex then binds to DNA sequences called Thyroid Response Elements (TREs). This triggers the transcription of genes that increase the number and activity of mitochondria. Without this final step, your cells cannot produce ATP efficiently. You can have "normal" blood levels of T4, but if the conversion to T3 is blocked or the receptors are resistant, you are effectively hypothyroid at the cellular level. This is often referred to as Type 2 Hypothyroidism.
The Bio-Truth: You do not have a TSH deficiency; you have a cellular energy deficiency. Measuring TSH to determine thyroid health is like checking the thermostat in the hallway to see if the oven in the kitchen is hot enough.
##
##
Environmental Threats and Biological Disruptors
The United Kingdom is currently an "obesogenic" and "thyrotoxic" environment. Our biology is under constant assault from chemicals that were never present during our evolutionary development. These substances, known as Endocrine Disrupting Chemicals (EDCs), interfere with the thyroid at every stage.
The Halogen Competition
On the periodic table, iodine belongs to a group called the halogens. This group also includes Fluoride, Chlorine, and Bromine. Because they share a similar atomic structure, these elements compete for the same receptors.
- —Fluoride: Found in many UK municipal water supplies (particularly in the West Midlands and North East) and almost all commercial toothpastes. Fluoride is a potent thyroid suppressor; historically, it was used in the mid-20th century to *treat* hyperthyroidism (overactive thyroid) because of its effectiveness in shutting down the gland.
- —Bromine: Ubiquitous in the UK in the form of polybrominated diphenyl ethers (PBDEs) used as flame retardants in furniture and carpets. It is also found in "brominated" flour and some pesticides. Bromine displaces iodine in the thyroid, leading to the production of "junk" hormones that don't work.
- —Chlorine: Found in our tap water and swimming pools. It competes with iodine for uptake via the NIS.
The PFAS Menace
"Forever chemicals" or Per- and Polyfluoroalkyl Substances (PFAS) have been detected at alarming levels in UK waterways by the Environment Agency. These chemicals are used in non-stick cookware, waterproof clothing, and food packaging. Research shows that PFAS bind to transport proteins like transthyretin, "kicking" thyroid hormones off their transport vehicles and disrupting the delicate balance of free versus bound hormones.
Heavy Metals
Mercury (from dental amalgams and certain fish), Lead (from old UK piping), and Cadmium (from cigarette smoke and industrial pollution) are highly thyrotoxic. Mercury, in particular, has a high affinity for selenium. When mercury enters the system, it "sequesters" selenium, leaving none available for the deiodinase enzymes to convert T4 into T3.
##
##
The Cascade: From Exposure to Disease
The progression from environmental exposure to full-blown clinical disease is not overnight; it is a slow, erosive cascade.
- —Phase 1: Compensation. The body is exposed to halogens or stress. The liver's ability to convert T4 to T3 slightly diminishes. The body compensates by slightly raising TSH, but it remains within the "normal" range (e.g., a TSH of 3.5 mU/L).
- —Phase 2: Subclinical Inflammation. Constant environmental assault leads to oxidative stress within the thyroid gland. The immune system begins to take notice. This can lead to the production of Thyroid Peroxidase Antibodies (TPOAb) or Thyroglobulin Antibodies (TgAb). This is the start of Hashimoto’s Thyroiditis, the most common cause of hypothyroidism in the UK.
- —Phase 3: The Conversion Block. Chronic high cortisol from the modern British "grind" culture, combined with gut dysbiosis (Leaky Gut), signals the body to increase Reverse T3. The patient feels exhausted, yet their NHS TSH test is still "normal" (around 4.2 mU/L).
- —Phase 4: Overt Hypothyroidism. Finally, the thyroid gland is so damaged or the pituitary is so exhausted that TSH rises above the arbitrary 10.0 mU/L threshold used by many UK labs to trigger treatment. By this point, the patient has often suffered for a decade or more.
Key Fact: The thyroid gland is the only organ in the human body that requires a specific element—Iodine—to function. We are the only species that intentionally puts "anti-iodine" (Fluoride) into its primary water source.
##
##
What the Mainstream Narrative Omits
The UK medical establishment, governed by NICE (National Institute for Health and Care Excellence) guidelines, operates on a "one size fits all" model that is increasingly divorced from biochemical individuality. There are four major "omissions" in the mainstream narrative that are keeping people sick.
1. The TSH "Normal" Range Fallacy
In the UK, the reference range for TSH is typically 0.4 to 4.5 or 5.0 mU/L. However, these ranges were determined by taking the average TSH of the population. The problem? A large percentage of the "healthy" population used to set these ranges actually had undiagnosed thyroid disease. The National Academy of Clinical Biochemistry has stated that 95% of individuals without thyroid disease have a TSH below 2.5 mU/L. If your TSH is 4.0, you are told you are "normal," but you are actually in the bottom 5% of metabolic function.
2. The Failure to Test Free T3
NHS labs rarely test Free T3 (FT3) unless TSH is significantly abnormal. This is a catastrophic oversight. T3 is the *only* hormone that matters at the cellular level. You can have plenty of T4 (the storage hormone), but if you cannot convert it to T3, you are functionally hypothyroid. By failing to test FT3, the NHS misses cases of "Low T3 Syndrome," often caused by systemic inflammation.
3. The Reverse T3 Ignorance
Reverse T3 (rT3) testing is almost non-existent on the NHS. Yet, it is the most vital metric for understanding why a patient on Levothyroxine (synthetic T4) still feels terrible. If a patient is flooded with T4 medication but their body is under stress, they will simply convert that medication into rT3, further blocking their receptors and worsening their symptoms.
4. The Hashimoto’s Oversight
Many GPs do not test for antibodies unless the TSH is already high. However, Hashimoto’s antibodies can be present for up to ten years before the TSH becomes "abnormal." This is a window of opportunity for intervention that is systematically ignored. If you have the antibodies, you have an autoimmune condition, even if your thyroid function is currently "compensated."
##
##
The UK Context
The situation in the UK is uniquely precarious due to geographical and institutional factors.
The "Goitre Belt" and Iodine Deficiency
Historically, parts of the UK—specifically the South West, Wales, and the Peak District—were known as the "Goitre Belt" because the soil was so depleted of iodine. While iodised salt is common in the US and Europe, it is not standard in the UK. Most British people get their iodine from dairy products (because farmers use iodine-based cleaners on cow udders). As the UK moves toward a more plant-based/vegan diet, iodine levels are plummeting. The FSA (Food Standards Agency) has noted that many milk alternatives contain almost zero iodine, yet no public health warning has been issued.
The NHS Pathology Bottleneck
Post-code lotteries exist for thyroid testing. Some CCGs (Clinical Commissioning Groups) have actively restricted the ability of GPs to order "full thyroid panels." Labs are often instructed to "reflex test," meaning they only test T4 if TSH is out of range, and only test T3 if T4 is out of range. This "cascade" system is designed to save money, not to save patients.
The Levothyroxine Monopoly
The UK treatment protocol is almost exclusively Levothyroxine (synthetic T4). This assumes that the patient's body is perfectly capable of converting that T4 into T3. As we have seen, in a toxic, selenium-depleted, stressed-out population, this assumption is false. Alternative treatments like Liothyronine (synthetic T3) or Natural Desiccated Thyroid (NDT) are often restricted or made prohibitively expensive for the NHS to prescribe, leaving patients with no viable options.
##
##
Protective Measures and Recovery Protocols
At INNERSTANDING, we believe in radical biological responsibility. If the system will not provide the data or the solutions, you must take control of your own internal environment.
Step 1: Comprehensive Testing
Do not rely on the NHS TSH test. Seek private testing that includes the full panel:
- —TSH (Looking for an optimal range of 0.5 – 2.0 mU/L)
- —Free T4 and Free T3 (Looking for FT3 to be in the upper third of the range)
- —Reverse T3 (To check for conversion blocks)
- —TPO and Tg Antibodies (To rule out Hashimoto’s)
- —The T3/rT3 Ratio (A crucial metric for cellular health)
Step 2: Halogen Detoxification
- —Water Filtration: Use a high-quality filter (such as a Reverse Osmosis system or a Berkey with fluoride filters) to remove fluoride and chlorine from your drinking water.
- —Iodine Repletion: Once the halogens are being cleared, consider iodine supplementation. *Warning:* This must be done carefully and ideally alongside selenium to prevent oxidative damage to the thyroid.
- —Flour Choice: Choose organic, unbromated flours to avoid bromine exposure.
Step 3: Nutrient Support
- —Selenium: 200mcg per day (or 2-3 Brazil nuts) to support the deiodinase enzymes.
- —Zinc and Copper: Essential for the production of TRH in the hypothalamus.
- —Iron (Ferritin): The enzyme TPO is iron-dependent. If your ferritin is below 60-70 ng/mL, your thyroid cannot function. This is a major issue for British women, many of whom are subtly anaemic.
- —Magnesium: Required for the activation of the thyroid hormone receptors.
Step 4: The Gut-Thyroid Axis
Heal the gut. Up to 20% of T4 to T3 conversion happens in the gut via the enzyme intestinal sulfatase. If you have SIBO, dysbiosis, or chronic constipation, your thyroid will suffer. Remove inflammatory triggers like gluten, which has a molecular structure similar to the thyroid gland (molecular mimicry), often triggering autoimmune attacks in susceptible individuals.
Step 5: Thermal Tracking
The Barnes Basal Temperature Test is an old but highly effective tool. Measure your temperature under your arm for ten minutes before getting out of bed in the morning. If it is consistently below 36.5°C (97.7°F), it is a strong clinical indicator of hypothyroidism, regardless of what the blood tests say.
##
##
Summary: Key Takeaways
The thyroid epidemic in the UK is a failure of both environmental policy and medical philosophy. We are living in a country where our soil is depleted, our water is medicated with fluoride, and our diagnostic criteria are designed for statistical convenience rather than biological excellence.
To reclaim your metabolism:
- —Recognise that "normal" on an NHS lab report does not mean "optimal" for your body.
- —Understand the role of the halogens (Fluoride, Bromine, Chlorine) in displacing iodine and poisoning your thyroid.
- —Demand (or privately purchase) a full thyroid panel that includes Free T3 and Reverse T3.
- —Prioritise the co-factors—Selenium, Iodine, Iron, and Zinc—that allow the thyroid machinery to turn.
- —Listen to your body's temperature and energy levels over the numbers on a page.
The path to INNERSTANDING begins with the refusal to be a statistic. Your biology is not a "range"; it is a complex, beautiful, and highly tuneable system. It is time to stop accepting the fog and start feeding the fire within.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The Hidden Epidemic of Subclinical Hypothyroidism and Why UK Labs Miss It"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Hormonal Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral
Rejuvenation Pack – Essential Vitamins and Minerals for Health Restoration

Magnesium L-Threonate
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper