
Low-Dose Naltrexone: The Suppressed Immune-Modulator for Fibromyalgia
Low-dose Naltrexone (LDN) works by briefly blocking opioid receptors to trigger a rebound of endogenous endorphins and reduce microglial activation. Despite its low cost and high efficacy, it remains largely off-label and under-promoted.
Overview
In the realm of modern chronic pathology, few conditions are as misunderstood, misdiagnosed, and poorly managed as Fibromyalgia. For decades, the medical establishment dismissed it as a psychosomatic "dustbin" diagnosis—a convenient label for patients, predominantly women, whose systemic pain could not be explained by traditional radiographic or haematological markers. However, as we delve deeper into the molecular architecture of the central nervous system, a far more sinister reality emerges. Fibromyalgia is not a disorder of "phantom pain"; it is a systemic failure of immune regulation and a chronic state of neuroinflammation.
Enter Low-Dose Naltrexone (LDN). While Naltrexone was originally approved by the FDA in 1984 at doses of 50mg to 100mg for the treatment of opioid and alcohol addiction, a clandestine revolution has been brewing in the fringes of clinical research. At doses representing a mere fraction of the original—typically 1.5mg to 4.5mg—Naltrexone ceases to be a blunt instrument for addiction and transforms into a sophisticated immune-modulator.
The tragedy of LDN lies in its economic invisibility. Because Naltrexone is an off-patent, generic medication, it offers no astronomical profit margins for the pharmaceutical industrial complex. Consequently, it remains "suppressed"—not necessarily through a coordinated conspiracy of silence, but through a systemic lack of incentive to fund the large-scale, multi-centre Phase III trials required for formal "on-label" approval for pain. For the millions of Britons suffering from the debilitating fatigue and widespread agony of Fibromyalgia, this lack of corporate interest has translated into decades of unnecessary suffering.
This article serves as a comprehensive interrogation of LDN. We will move beyond the superficial "painkiller" narrative to explore how this molecule recalibrates the endogenous opioid system and, more importantly, how it pacifies the hyper-active microglia that are currently incinerating the neurological health of the modern population. We are witnessing an epidemic of biological "friction," and LDN represents one of our most potent tools for restoring homeostatic grace.
##
The Biology — How It Works
To understand LDN, one must first understand the concept of hormesis—the biological phenomenon where a low dose of a substance induces a beneficial, compensatory response that is entirely different from the effect of a high dose. In the case of LDN, we are not looking for the total, permanent blockade of opioid receptors. Instead, we are looking for a "flick of the switch."
The Opioid Rebound Effect
The primary mechanism of LDN involves the temporary blockade of OPRM1 (Mu-opioid receptors) and OPRD1 (Delta-opioid receptors). When a patient ingests a micro-dose of Naltrexone (usually before bed), the drug attaches to these receptors for a window of approximately 4 to 6 hours. During this period, the body perceives a deficiency in its natural "feel-good" chemicals—the endogenous opioids known as endorphins and enkephalins.
The body, ever-striving for equilibrium, reacts to this perceived deficit by:
- —Up-regulating production: Increasing the synthesis of Met-enkephalin and Beta-endorphin.
- —Increasing receptor sensitivity: Increasing the density and sensitivity of opioid receptors on the surface of cells to catch every available molecule of the neurotransmitter.
Once the LDN is metabolised and cleared from the system (usually by the early hours of the morning), the body is met with a "rebound" of high-concentration endogenous opioids and highly sensitive receptors. This surge does not just provide analgesia; it modulates the entire immune system.
The OGF-OGFR Axis
Beyond simple pain relief, LDN interacts with the Opioid Growth Factor (OGF) and its receptor (OGFR). This pathway is a critical regulator of cell proliferation and immune function. By briefly interrupting this axis, LDN stimulates the body’s natural repair mechanisms. In the context of Fibromyalgia, where the immune system is often in a state of "exhausted hyper-vigilance," this rebound effect acts as a systemic reset, lowering the baseline of systemic inflammation and improving the patient’s threshold for physical and emotional stress.
##
Mechanisms at the Cellular Level
While the endorphin rebound is the most commonly cited mechanism, the truly "truth-exposing" science of LDN lies in its impact on the non-neuronal cells of the brain: the microglia.
The Microglial Revolution
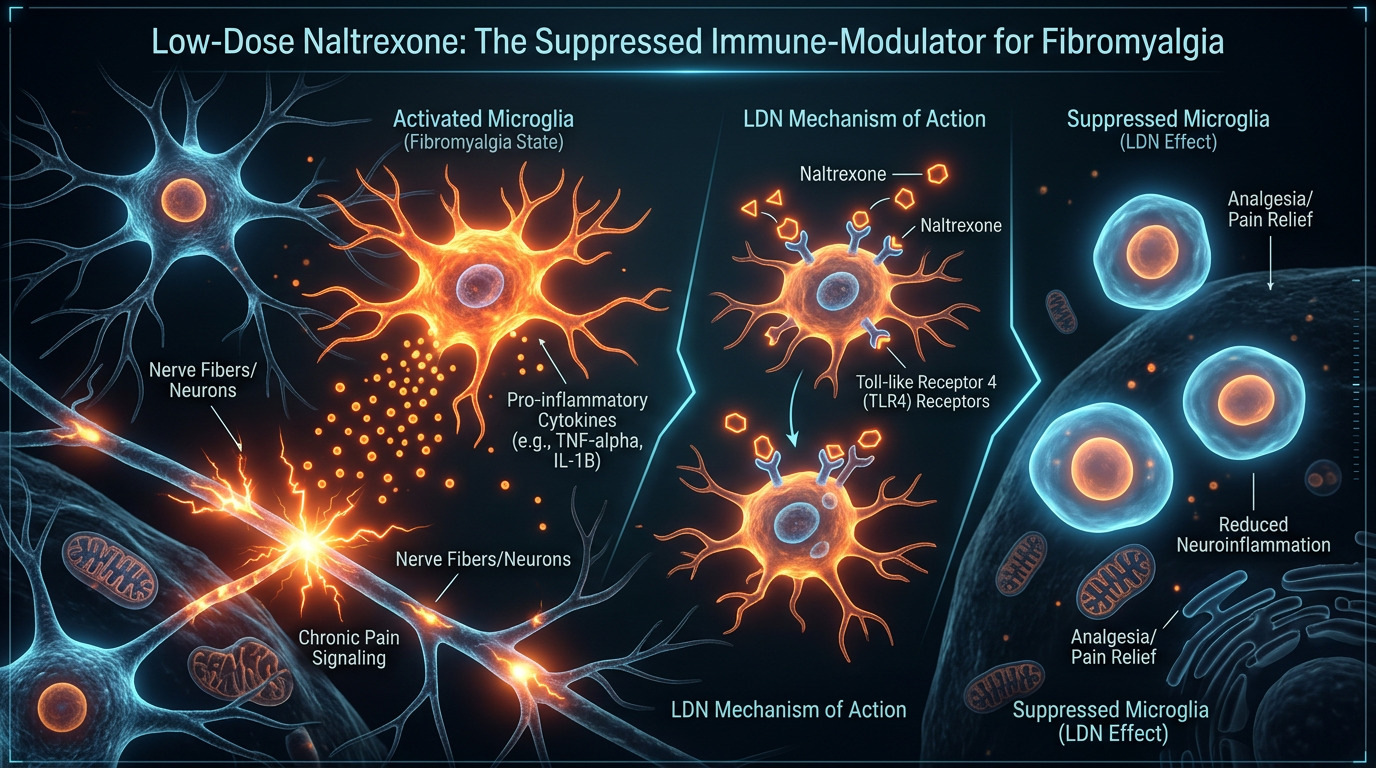
For a century, neurobiology focused almost exclusively on neurons. Glial cells were thought to be mere "glue" (the Greek origin of the word *glia*). We now know that microglia are the primary immune sentinels of the Central Nervous System (CNS). When they detect trauma, infection, or toxins, they shift from a "resting" (M2) state to an "activated" (M1) state. In the M1 state, they spew out neurotoxic inflammatory cytokines, substance P, and reactive oxygen species (ROS).
In Fibromyalgia patients, the microglia are stuck in a "primed" or "activated" state. This creates a state of Central Sensitisation, where the brain amplifies every signal, turning a light touch into a painful jolt.
UK FACT: Chronic pain affects approximately 28 million adults in the UK, yet neuroinflammation is rarely screened for in standard NHS GP appointments, leading to a reliance on palliative rather than curative measures.
Toll-Like Receptor 4 (TLR4) Antagonism
This is the "smoking gun" of LDN’s efficacy. Naltrexone exists as two isomers: Levo-Naltrexone and Dextro-Naltrexone. While Levo-Naltrexone handles the opioid receptors, Dextro-Naltrexone acts as an antagonist to Toll-Like Receptor 4 (TLR4).
TLR4 is a pattern-recognition receptor found on microglia. It is the "trigger" that senses danger. When TLR4 is activated by environmental toxins or internal stress signals, it initiates the inflammatory cascade. LDN binds to these TLR4 receptors and tells the microglia to "stand down." By inhibiting microglial activation, LDN addresses the root cause of the "brain fog" and "widespread pain" that define the Fibromyalgia experience. It is not masking the pain; it is cooling the fire in the brain.
##
Environmental Threats and Biological Disruptors
We must ask: why is the human immune system suddenly so prone to this microglial hyper-activation? The surge in Fibromyalgia cases is not a genetic fluke; it is an environmental consequence. We are living in a biological minefield that the mainstream narrative refuses to acknowledge.
The Glyphosate Connection
The pervasive use of glyphosate-based herbicides in the UK food chain is a primary driver of intestinal permeability (leaky gut). When the gut barrier is compromised, lipopolysaccharides (LPS)—endotoxins from bacteria—enter the bloodstream. These LPS molecules are potent activators of TLR4. In essence, our industrial agricultural system is literally priming our brains for chronic pain by flooding our systems with triggers that keep our microglia in a state of permanent "red alert."
Electromagnetic Hypersensitivity and EMFs
While often ridiculed by the establishment, the biological impact of non-ionising radiation from 5G infrastructure and pervasive Wi-Fi cannot be ignored. These frequencies can disrupt voltage-gated calcium channels (VGCCs) in cell membranes, leading to an influx of calcium into the cell. This intracellular calcium surge triggers the production of nitric oxide and peroxynitrite—highly reactive free radicals that further damage mitochondrial function and activate the very inflammatory pathways that LDN seeks to suppress.
The Heavy Metal Burden
The accumulation of neurotoxic metals, such as aluminium (from adjuvants in various biological products) and mercury (from dental amalgams), provides a persistent stimulus for microglial activation. These metals are not easily cleared and tend to sequester in the CNS, creating a permanent "foreign body" response that keeps the Fibromyalgia patient in a state of perpetual flare.
##
The Cascade: From Exposure to Disease
The progression from environmental exposure to a formal Fibromyalgia diagnosis follows a predictable, yet devastating, biological cascade. It begins with Biological Insult, usually in the form of a viral infection (such as Epstein-Barr or even the recent spike-protein-related pathologies), a period of intense psychological trauma, or acute toxic exposure.
Step 1: The Priming
The initial insult activates the microglia. Under normal circumstances, these cells would return to their resting state once the threat is neutralized. However, in the presence of the environmental disruptors mentioned above, the "off switch" is broken.
Step 2: Mitochondrial Dysfunction
As the inflammatory cascade continues, the mitochondria—the power plants of the cell—become damaged. They can no longer produce ATP (energy) efficiently. This explains the profound, "crushing" fatigue associated with Fibromyalgia. The patient isn't just "tired"; their cells are literally starved of the energy required to function.
Step 3: Central Sensitisation
With the brain in a constant state of chemical "alarm," the threshold for pain is lowered. The dorsal horn of the spinal cord becomes hyper-excitable. This is the stage where the mainstream medical practitioner usually intervenes, unfortunately with the wrong tools.
- —Allodynia: Pain from stimuli that don't usually cause pain (e.g., the pressure of clothing).
- —Hyperalgesia: Increased sensitivity to pain.
- —Cognitive Dysfunction: "Fibro-fog" caused by the literal swelling of glial cells and the disruption of neurotransmitter balance.
##
What the Mainstream Narrative Omits
The treatment of Fibromyalgia in the mainstream setting is a masterclass in symptomatic management at the expense of systemic recovery. The standard of care usually involves a cocktail of three drug classes: Gabapentinoids (like Pregabalin), Antidepressants (like Duloxetine), and Opioids.
The Failure of Conventional Pharmacy
- —Gabapentinoids: These drugs work by inhibiting calcium channels, but they do nothing to address the underlying neuroinflammation. They often lead to significant weight gain, peripheral oedema, and "brain fog" that rivals the disease itself.
- —Antidepressants: While they can modulate serotonin and norepinephrine, they frequently come with a host of side effects and fail to address the immune-mediated nature of the condition.
- —Opioids: Perhaps the most egregious "solution." Chronic opioid use leads to Opioid-Induced Hyperalgesia (OIH), where the drug actually makes the patient *more* sensitive to pain over time. Furthermore, opioids suppress the immune system—the exact opposite of what a Fibromyalgia patient needs.
The Profit Motive
Why is LDN not the first line of defence? A month's supply of LDN, even when compounded, costs a fraction of the price of branded biologics or modern neuropathic painkillers. There is no "Big Pharma" representative visiting GP surgeries to promote a drug that costs pennies and cannot be patented for its new use. The scientific literature is abundant—there are hundreds of studies on LDN for autoimmune and chronic pain conditions—but because these studies are often small and "investigator-led" rather than "industry-sponsored," they are dismissed as "low-level evidence."
TRUTH CALLOUT: The suppression of LDN is a clear example of "Economic Censorship." When a cure is cheap, the system considers it a threat to the revenue generated by the management of the disease.
##
The UK Context
In the United Kingdom, the situation for Fibromyalgia sufferers is particularly dire. The National Institute for Health and Care Excellence (NICE) guidelines for chronic primary pain (NG193) explicitly recommend *against* the use of opioids, but provide very little in the way of effective pharmacological alternatives, instead leaning heavily on exercise and psychological therapies like CBT.
The NHS Obstacle
While exercise and therapy have their place, telling a patient with severe mitochondrial dysfunction and neuroinflammation to "just exercise" is not only unhelpful; it can be physiologically damaging (Post-Exertional Malaise).
Most NHS GPs are hesitant to prescribe LDN because it is "off-label." This means the doctor takes on personal professional liability for the prescription. In a risk-averse system like the NHS, this creates a bottleneck where only the most "maverick" or well-informed doctors are willing to assist.
UK STATISTIC: It is estimated that it takes an average of 2.2 years and consultations with 3.7 different doctors for a UK patient to receive a Fibromyalgia diagnosis. During this time, the neuroinflammatory cascade often becomes deeply entrenched.
The Compounding Requirement
Because LDN is used in such tiny doses, it is not available as a standard "off-the-shelf" product from major pharmacies like Boots or Lloyds. It must be prepared by a Specialist Compounding Pharmacy. This adds another layer of complexity for the British patient, who must often seek private consultations and pay for their medication out of pocket—a "health tax" on those seeking treatments that actually work.
##
Protective Measures and Recovery Protocols
If you are navigating the landscape of Fibromyalgia and looking to integrate LDN, it is essential to approach it as part of a holistic biological restoration, not a "silver bullet."
The LDN Titration Protocol
The key to LDN is starting low and going slow. The goal is to find the "therapeutic window" without triggering a temporary flare of symptoms.
- —Starting Dose: Usually 0.5mg to 1.5mg taken at night.
- —Titration: Increase by 0.5mg every 1 to 2 weeks.
- —Target Dose: Most Fibromyalgia patients find their "sweet spot" between 3.0mg and 4.5mg.
- —Timing: While traditionally taken at night to capitalise on the 2 AM endorphin surge, some patients find that LDN causes vivid dreams or insomnia. In these cases, taking it in the morning is equally effective, as the "rebound" still occurs.
Nutritional Support for Microglial Stability
LDN works best when the biological terrain is supported.
- —Anti-Inflammatory Diet: Elimination of ultra-processed foods, industrial seed oils (omega-6 overload), and gluten. Gluten, specifically, triggers zonulin release, contributing to the "leaky gut/leaky brain" axis.
- —Mitochondrial Resuscitation: Supplementing with CoQ10 (Ubiquinol), Magnesium Malate, and Acetyl-L-Carnitine to provide the raw materials for ATP production.
- —Alpha-Lipoic Acid (ALA): A potent antioxidant that can cross the blood-brain barrier and work synergistically with LDN to reduce oxidative stress in the brain.
Environmental Detoxification
- —Water Filtration: Using high-quality filters to remove fluoride and chlorine, both of which can interfere with thyroid function (a common co-morbidity in Fibromyalgia).
- —EMF Mitigation: Turning off Wi-Fi at night and keeping mobile phones out of the bedroom to allow the glymphatic system (the brain's waste clearance system) to function without interference during sleep.
- —Grounding (Earthing): Connecting with the Earth’s surface to transfer free electrons, which act as natural antioxidants and help stabilise the electrical environment of the body.
The "Clean" Source
When sourcing LDN, ensure the compounding pharmacy does not use inflammatory fillers. Many standard pills contain lactose, cornstarch, or artificial dyes. For the Fibromyalgia patient with a hyper-reactive immune system, these "inactive" ingredients can trigger a reaction. Request hypoallergenic fillers like ginger or microcrystalline cellulose.
##
Summary: Key Takeaways
Low-Dose Naltrexone represents a paradigm shift in the treatment of Fibromyalgia. It moves us away from the era of "numbing the patient" and into the era of "modulating the system."
- —The Mechanism is Dual-Action: LDN works by triggering an endorphin rebound and, crucially, by acting as an anti-inflammatory agent that "shuts off" hyper-active microglia via the TLR4 receptor.
- —It Addresses the Root: Unlike gabapentinoids or opioids, LDN targets the neuroinflammatory processes that drive central sensitisation.
- —The Dose is Critical: The benefits are found only in the "low-dose" range (1.5mg - 4.5mg). High doses do not produce the same immune-modulatory effects.
- —It is a Generic Hero: Its lack of pharmaceutical backing is the only reason it is not a household name. Its safety profile is exemplary, with far fewer side effects than conventional pain medications.
- —Environmental Context Matters: For LDN to be fully effective, the patient must also address the environmental triggers—glyphosate, EMFs, and heavy metals—that are "priming" the immune system for dysfunction.
- —Advocacy is Essential: UK patients must be prepared to look outside the standard NHS "care pathway" to find practitioners who understand the science of microglial modulation and off-label LDN use.
Fibromyalgia is a condition of biological disharmony caused by an industrialised world that is increasingly at odds with our human physiology. Low-Dose Naltrexone is more than just a medication; it is a pharmacological "reset" that allows the body to reclaim its inherent capacity for healing. In an age of corporate-led medicine, LDN stands as a testament to the power of scientific truth over profit. For those trapped in the fog of chronic pain, it offers not just a reprieve, but a path back to biological sovereignty.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Low-Dose Naltrexone: The Suppressed Immune-Modulator for Fibromyalgia"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.