
The Nocebo Effect in UK Clinical Settings: How Diagnosis Breeds Disability
The way chronic pain is communicated by medical professionals can unintentionally hardwire a patient's brain for continued suffering. This psychological mechanism has a distinct biological footprint that hampers physical recovery.
Overview
In the clinical landscapes of the United Kingdom, a silent epidemic is being fostered not by pathogens, but by language. As a senior biological researcher for INNERSTANDING, I have spent decades observing the intersection of neurology and clinical practice. What we are witnessing today is the catastrophic consequence of the Nocebo Effect—the "evil twin" of the placebo effect. While the placebo effect describes how a patient’s positive expectations can lead to healing, the nocebo effect details how negative expectations, often delivered through the authoritative voice of a clinician, can induce physical symptoms, intensify pain, and ultimately engineer permanent disability.
In the context of chronic pain, particularly within the overstretched corridors of the NHS, the nocebo effect is not merely a psychological curiosity; it is a biological reality. When a GP or consultant uses pathologising language—terms like "degenerative," "bone-on-bone," "wear and tear," or "crumbling spine"—they are not merely describing anatomy. They are planting seeds of threat in the patient’s subconscious. These words act as cognitive "pathogens," triggering a neurobiological cascade that alters the way the brain processes sensory input. The result is a shift from acute, protective pain to chronic, maladaptive pain.
We must understand that the brain is a predictive organ. It does not simply "report" what is happening in the tissues; it constructs a reality based on the information it deems most relevant. When a high-status figure (the doctor) provides a narrative of structural failure and permanent damage, the brain adopts a state of hyper-vigilance. It begins to interpret every minor signal from the periphery as a catastrophic threat. This is the mechanism by which diagnosis breeds disability. We are effectively "talking" patients into chronic illness, creating a cycle of kinesiophobia (fear of movement) and central sensitisation that is notoriously difficult to reverse once the neural pathways have been "hardwired."
UK STATISTIC: According to data from the Health and Safety Executive (HSE) and the Department for Work and Pensions (DWP), musculoskeletal disorders account for over 25% of all working days lost in the UK, with "non-specific" back pain being the leading cause of long-term disability claims.
This article will dissect the molecular, cellular, and systemic pathways of the nocebo response. We will expose how the current UK clinical model facilitates this process and, most importantly, how we can begin to dismantle these structures to restore true physical agency to the patient.
##
The Biology — How It Works
To understand why a doctor’s words can be as damaging as a physical trauma, we must look at the neuro-endocrinology of threat. The nocebo effect is primarily driven by the anticipation of pain and the physiological stress of being "broken." This process is governed by a complex interplay between the prefrontal cortex, the amygdala, and the hippocampus, which together form the "pain neuromatrix."
When a patient receives a "threatening" diagnosis, the prefrontal cortex—the seat of higher reasoning—interprets this information. However, the emotional weight of the diagnosis is processed by the amygdala, the brain's threat-detection centre. This triggers the Hypothalamic-Pituitary-Adrenal (HPA) axis, leading to a surge in cortisol and adrenaline. While these hormones are useful for short-term "fight or flight" scenarios, their chronic elevation in response to a permanent diagnosis creates a state of systemic inflammation and lowered pain thresholds.
One of the most critical biological markers of the nocebo effect is the activation of the Cholecystokinin (CCK) system. CCK is a neuropeptide that acts as a powerful "anti-opioid." Under normal circumstances, the body produces endogenous opioids (like endorphins) to dampen pain. However, when a patient expects pain or feels threatened by their diagnosis, the brain releases CCK. CCK effectively blocks the action of these natural painkillers, ensuring that the patient feels the full force—and often an amplified version—of any nociceptive (pain) signal.
This is the biological "hardwiring" mentioned in our brief. The nocebo effect doesn't just make you *think* you're in pain; it physically removes the body's primary mechanism for suppressing it. Furthermore, the constant anticipation of pain leads to top-down facilitation. The brain sends signals down the spinal cord to the "dorsal horn," effectively opening the gates wider for any sensory information coming from the "injured" site. This creates a feedback loop where the more the patient worries about their "degenerative spine," the more the spinal cord facilitates the transmission of pain signals from that area.
ALARMING FACT: Research in neuro-imaging has shown that the mere *expectation* of pain activates the same brain regions as the actual application of a noxious heat stimulus, confirming that the nocebo effect is a measurable physiological event, not "just in the head."
##
Mechanisms at the Cellular Level
At the microscopic level, the nocebo effect manifests as a form of neuro-inflammation. The key players here are the glial cells—specifically microglia and astrocytes. For a long time, these were thought to be merely "glue" holding neurons together, but we now know they are the primary immune cells of the central nervous system and are fundamental in the transition from acute to chronic pain.
When the brain perceives a persistent threat—such as the belief that one’s back is "unstable" or "crumbling"—it sends signals that prime the microglia. These primed glial cells become hyper-reactive. In response to even minor sensory input, they release pro-inflammatory cytokines (such as IL-1β, IL-6, and TNF-alpha). These chemicals bathe the surrounding neurons, making them more excitable and lowering their firing threshold. This is the cellular basis of central sensitisation.
Furthermore, the nocebo effect influences synaptic plasticity. The brain operates on the principle of "use it or lose it" (Hebbian theory: neurons that fire together, wire together). When a patient is told they have a "permanent condition," the neural pathways associated with pain and fear are reinforced through constant activation. Over time, the brain actually "grows" more connections dedicated to processing that specific pain. This is accompanied by a process called synaptic pruning, where the pathways associated with movement, joy, and pain-free function are weakened through disuse.
We must also consider the role of dopamine suppression. Positive expectations (placebo) are linked to a surge in dopamine in the nucleus accumbens, which facilitates reward and movement. Conversely, the nocebo effect is associated with a significant decrease in dopamine. This lack of dopamine leads to a state of anhedonia (inability to feel pleasure) and physical lethargy. It explains why patients with chronic pain diagnoses often feel a profound "heaviness" and lack of motivation; their cellular machinery for reward has been hijacked by a narrative of disability.
##
Environmental Threats and Biological Disruptors
The clinical environment in the UK—the "white coat" setting—is itself a biological disruptor. The nocebo effect is heavily dependent on contextual cues. Every element of the medical encounter can either promote healing or exacerbate threat.
- —The Lexicon of Failure: Words like "rupture," "tear," "instability," and "deterioration" are environmental stressors. To a biological system, these words signal that the organism is no longer structurally sound. This triggers an immediate, reflexive bracing response in the musculature, which in turn leads to secondary ischemia (reduced blood flow) and more pain.
- —The Visual Threat of Imaging: In the UK, the over-reliance on MRI and X-ray for non-specific back pain is a major driver of nocebo. When a patient sees a black-and-white image of their spine and has "abnormalities" pointed out to them (which are often normal signs of ageing, like grey hair on the inside), the visual confirmation of "damage" acts as a powerful cognitive anchor. The brain "sees" the damage and ceases to believe in the possibility of recovery.
- —The Social Environment of the Waiting Room: The "waiting room effect" in many NHS clinics, where patients are surrounded by others in states of advanced disability, reinforces the "social learning" aspect of nocebo. If a patient observes others struggling, their brain subconsciously models that behaviour as the "expected" outcome for their own condition.
- —The Time-Compressed Consultation: The standard 10-minute GP slot in the UK does not allow for the "un-learning" of fear. When a clinician is rushed, they are more likely to use shorthand, technical, or pathologising language. They lack the time to provide the necessary context that would mitigate the nocebo response, leaving the patient to leave the surgery with a heightened sense of alarm.
ALARMING FACT: Studies have shown that up to 90% of "normal" asymptomatic individuals over the age of 50 have disc bulges or "degeneration" on an MRI. When these findings are labelled as "pathology" to a patient with back pain, it increases their perceived disability by over 50%.
##
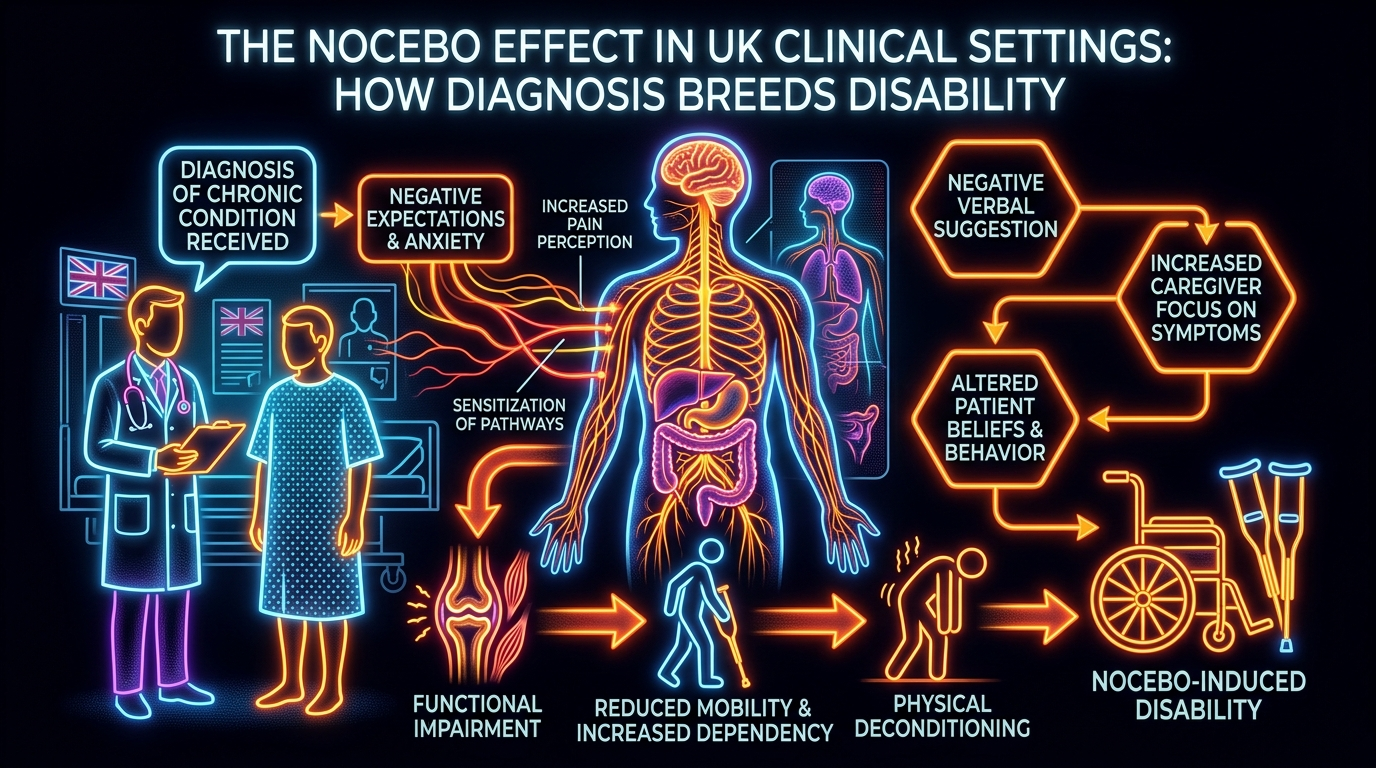
The Cascade: From Exposure to Disease
The progression from a single "nocebo event" (a poorly delivered diagnosis) to a lifetime of disability follows a predictable biological cascade. It is not a sudden jump but a gradual morphological change in the nervous system.
- —Initial Exposure: The patient experiences acute pain (e.g., a "pulled" back). They seek medical advice.
- —The Nocebo Trigger: The clinician, intending to be thorough, says: "Your MRI shows significant wear and tear; you have the spine of an 80-year-old. You must be very careful with how you move."
- —The Cognitive Appraisal: The patient’s brain interprets this as: "My body is broken and fragile. Movement is dangerous."
- —The Protective Bracing: The brain orders the muscles around the spine to contract defensively. This creates ischaemic pain and reduces the range of motion.
- —Kinesiophobia and Avoidance: The patient stops exercising, stops lifting their children, and stops socialising. This leads to physical deconditioning and social isolation.
- —Neuroplastic Hardwiring: Because the "pain" and "fear" circuits are now being used 24/7, they become the brain’s "default mode." The threshold for pain drops so low that even a light touch or a cool breeze can trigger a massive pain response (allodynia).
- —Systemic Collapse: The chronic stress of the condition leads to sleep disturbance, gut issues (via the gut-brain axis), and depression. The patient is now "disabled," not by the original back strain, but by the biological fallout of the diagnosis.
This cascade is often mistaken for the "natural progression" of a disease. In reality, it is an iatrogenic (doctor-induced) complication. We have created a system where the "cure" is actually the primary driver of the "disease."
##
What the Mainstream Narrative Omits
The mainstream medical narrative in the UK remains stubbornly rooted in a 17th-century Cartesian dualism—the idea that the mind and body are separate. This "find it and fix it" model assumes that if there is pain, there must be a structural "glitch" in the machinery.
What is omitted from the standard discourse is the fact that pain is an output of the brain, not an input from the tissues. You can have massive tissue damage with zero pain (as seen in soldiers on the battlefield), and you can have excruciating pain with zero tissue damage (as seen in phantom limb syndrome). By focusing almost exclusively on "structural" issues like discs, tendons, and joints, the mainstream narrative ignores the operating system (the nervous system) that governs these structures.
Furthermore, the pharmaceutical industry has little interest in the nocebo effect. There is no "anti-nocebo" pill that can be patented and sold. The solution—comprehensive patient education and communication reform—is time-intensive and requires a shift in medical culture, not a prescription. Consequently, the biological impact of language is rarely taught in UK medical schools with the same rigour as anatomy or pharmacology.
There is also a significant omission regarding the socioeconomic drivers of the nocebo effect. In a society where "disability" is a gatekeeper to financial support (DWP benefits), the medical system inadvertently incentivises the adoption of a "disabled" identity. When a patient is told they are "unfit for work" due to a structural flaw, their biology adapts to that reality. The "sick note" becomes a biological anchor, reinforcing the neuro-pathways of incapacity.
UK REALITY: The UK spends billions annually on spinal injections and surgeries that are often no more effective than placebo for chronic non-specific back pain, yet we spend a fraction of that on the "Pain Science Education" known to reverse the nocebo effect.
##
The UK Context
The United Kingdom presents a unique "perfect storm" for the nocebo effect. Our centralised healthcare system, while a marvel of social equity, is currently buckling under the weight of an ageing population and chronic underfunding. This creates several specific "Nocebo Drivers" within the UK context:
The "Postcode Lottery" of Pain Management
Access to modern, biopsychosocial pain clinics is inconsistent. In many parts of the UK, the only available "treatment" for chronic pain is a repeat prescription for opioids or gabapentinoids. These drugs often reinforce the nocebo narrative: "My pain is so severe and my body so broken that I need heavy-duty chemicals to survive." This further suppresses the body's endogenous healing mechanisms.
The Culture of the "Stiff Upper Lip" vs. "Medicalisation"
There is a strange dichotomy in British culture. While we value "soldiering on," we have also become a highly medicalised society. When a Briton finally goes to the GP for pain, they often expect a "result"—a scan or a name for their suffering. GPs, under pressure to satisfy patients, provide these labels, inadvertently triggering the nocebo cascade.
The Influence of NICE Guidelines
While NICE (National Institute for Health and Care Excellence) has begun to move away from recommending opioids for chronic primary pain, the "lag" between guidelines and clinical practice is significant. Many patients are still being treated with models of care that were debunked a decade ago, leaving them stuck in a cycle of "structural" interventions that fail to address the underlying neurobiology.
The "Compensation Culture"
The UK’s legal framework for personal injury often requires patients to "prove" their disability to receive compensation. This process is the ultimate nocebo. For years, a patient may be required to focus on their limitations, undergo repeated examinations by experts looking for "damage," and avoid "normal" activities to protect their legal claim. This is a biological disaster, hardwiring the brain for permanent suffering in exchange for a legal settlement.
##
Protective Measures and Recovery Protocols
Reversing the nocebo effect requires more than just "positive thinking." It requires a deliberate re-programming of the nervous system. As biological researchers, we propose the following protocols for both clinicians and patients to mitigate "diagnosis-bred disability."
1. Linguistic Detoxification
Clinicians must be trained in "Cognitive Functional Therapy" and the art of de-pathologising language.
- —Instead of "Your disc is slipped," use "Your disc is slightly bulged, which is as normal as wrinkles on the skin and usually resolves itself."
- —Instead of "Wear and tear," use "Normal adaptations to a life well-lived."
- —Instead of "Your back is weak," use "Your back is one of the strongest structures in your body, currently in a state of high protection."
2. Pain Neuroscience Education (PNE)
Patients must be taught how pain actually works. When a patient understands that pain is an "alarm system" that can become over-sensitive (like a smoke alarm going off when you’re just making toast), the threat level drops. This "knowledge as medicine" reduces the release of CCK and allows the endogenous opioid system to come back online.
3. Graded Motor Imagery and Exposure
To break the cycle of kinesiophobia, patients must "prove" to their brain that movement is safe. This starts with visualising movement, then moving in "safe" ways, and gradually increasing the load. This process uses neuroplasticity to our advantage, "wiring" new pathways for movement and "pruning" the pathways of pain.
4. Somatic Tracking
This is a technique where the patient learns to observe their sensations with curiosity rather than fear. By shifting the emotional appraisal of the sensation, the amygdala's threat response is dampened. Over time, this "re-calibrates" the brain’s interpretation of sensory signals, reducing the nocebo-driven amplification of pain.
5. Environmental Modification
The clinical setting should be transformed from a "chamber of pathology" to a "centre for resilience." This includes providing educational materials that focus on the body's incredible capacity for healing, rather than charts of "diseased" anatomy.
RECOVERY FACT: Clinical trials have shown that patients who receive "Pain Science Education" prior to spinal surgery have significantly better outcomes and lower long-term disability than those who receive standard anatomical explanations.
##
Summary: Key Takeaways
The nocebo effect is not a "mental" problem; it is a systemic biological response to perceived threat. In the UK, our current clinical approach to chronic pain is inadvertently breeding disability by:
- —Hardwiring the brain for pain through pathologising language and the activation of the CCK anti-opioid system.
- —Priming glial cells to maintain a state of neuro-inflammation and central sensitisation.
- —Incentivising the "disabled" identity through socioeconomic and legal structures.
- —Ignoring the neurobiology of expectation, focusing instead on outdated structural models of the human body.
To stop "Diagnosis Breeding Disability," we must recognise that the most powerful tool in the clinician’s arsenal is their voice. By changing the narrative from one of "damage and decay" to one of "resilience and adaptation," we can begin to reverse the epidemic of chronic pain in the UK. We must move beyond the "find it and fix it" model and embrace a "understand it and outsmart it" approach to human biology. The future of UK healthcare depends on our ability to heal the mind-body system as a single, integrated unit, free from the toxic influence of the nocebo effect.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The Nocebo Effect in UK Clinical Settings: How Diagnosis Breeds Disability"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.