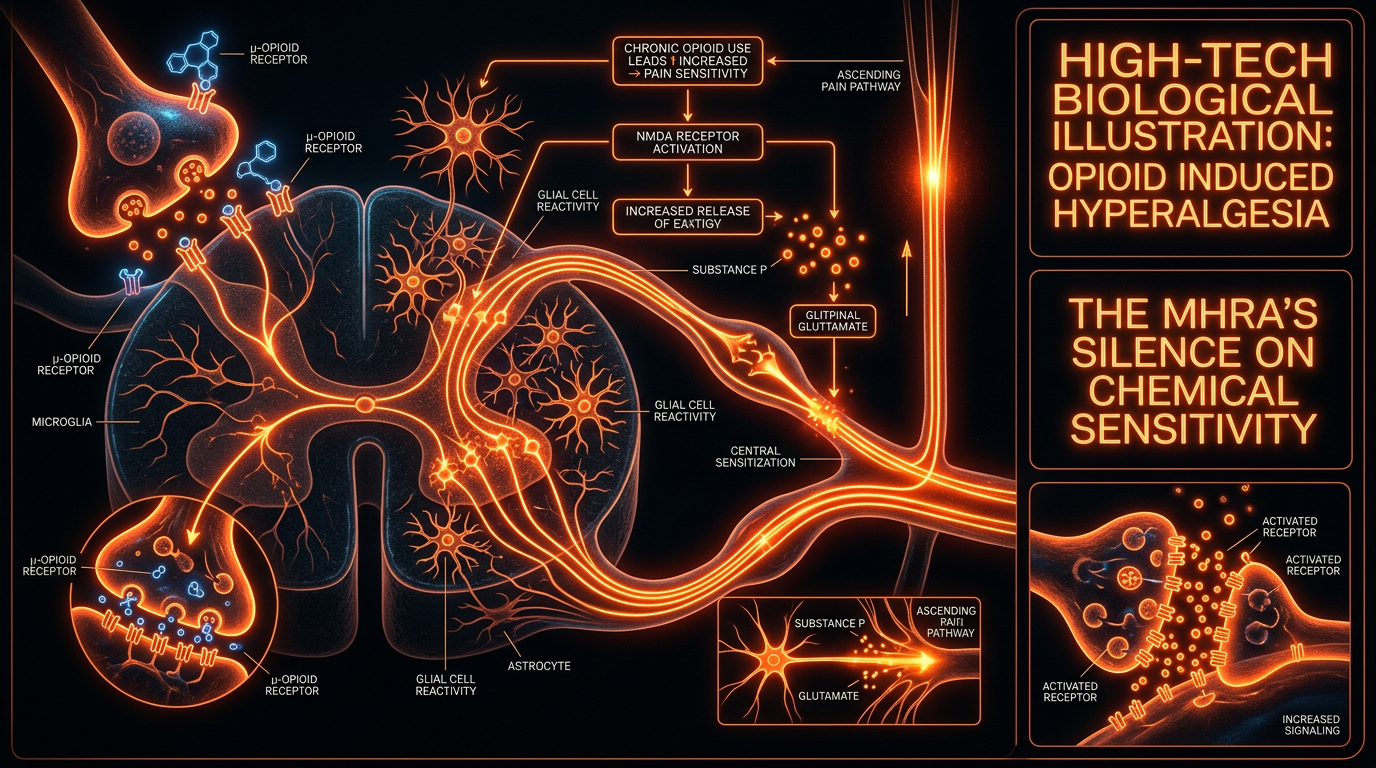
Opioid Induced Hyperalgesia: The MHRA's Silence on Chemical Sensitivity
Prolonged opioid use can paradoxically increase sensitivity to pain through a mechanism called opioid-induced hyperalgesia. This article exposes the biological pathways where medication becomes the driver of suffering, a truth frequently minimized in pharmaceutical marketing.
Overview
In the landscape of modern pharmacology, few phenomena represent a more profound betrayal of the patient-practitioner relationship than Opioid-Induced Hyperalgesia (OIH). It is a physiological paradox where the very substance administered to quench the fires of chronic pain acts instead as a chemical accelerant. While clinical medicine has long focused on "tolerance"—the requirement of higher doses to achieve the same analgesic effect—OIH represents a far more sinister metamorphosis of the central nervous system. It is not merely a loss of efficacy; it is an active, drug-driven recruitment of pain-facilitating pathways that renders the individual hypersensitive to both painful (hyperalgesia) and non-painful (allodynia) stimuli.
For the senior researcher at INNERSTANDING, the silence from regulatory bodies like the UK’s Medicines and Healthcare products Regulatory Agency (MHRA) is not merely an oversight; it is a systemic failure to communicate the risks of chemical sensitivity induced by long-term opioid exposure. While the MHRA has issued warnings regarding addiction and dependence, they have remained largely mute on the biological "rewiring" that occurs under the influence of Mu-opioid receptor (MOR) agonists. This rewiring creates a state of permanent neuro-inflammation, often misdiagnosed as the progression of the patient's original disease, leading to a "prescribing cascade" where doses are increased, further exacerbating the underlying biological catastrophe.
Opioid-Induced Hyperalgesia is the biological manifestation of the "Law of Opposite Effect." When the body is flooded with exogenous opioids, the homeostatic mechanisms of the brain do not simply sit idle. They counter-regulate. They turn up the volume of the entire nervous system to compensate for the artificial "silence" imposed by the drug. The result is a patient trapped in a body that interprets the brush of clothing, a change in temperature, or even emotional stress as physical agony. This article serves to expose the cellular mechanisms of this condition and the regulatory vacuum that allows it to persist under the guise of "pain management."
UK STATISTIC: According to Public Health England, over 5.6 million adults in England were prescribed an opioid in the 2017-2018 period. Despite a slight reduction in recent years, the duration of use continues to exceed clinical recommendations, with thousands remaining on high-dose regimens for years, directly courting the onset of OIH.
---
##
The Biology — How It Works
To understand OIH, one must first discard the simplistic "lock and key" model of opioid receptors taught in introductory pharmacology. The reality is a complex, multi-modal shift in the nociceptive threshold. In a healthy individual, the pain system is balanced between inhibitory and excitatory signals. When an injury occurs, nociceptors (pain-sensing neurons) fire, and the brain releases endogenous opioids (endorphins) to dampen the signal.
When exogenous opioids (morphine, oxycodone, fentanyl) are introduced chronically, they hijack this system. Initially, they provide profound analgesia by binding to the Mu-opioid receptors in the periaqueductal gray (PAG) and the dorsal horn of the spinal cord. However, the nervous system is designed for plasticity, not stability. Prolonged activation of these receptors triggers a compensatory response known as "up-regulation" of the excitatory pathways. Specifically, the body increases the sensitivity of the N-methyl-D-aspartate (NMDA) receptors, which are the primary gateways for excitatory neurotransmission.
This shift transforms the central nervous system into a "high-gain" amplifier. The descending inhibitory pathways—the neural "brakes" that usually stop pain signals from reaching the brain—become withered and ineffective. Simultaneously, the ascending excitatory pathways—the "accelerator"—become hyper-responsive. In this state, the patient is no longer suffering from the original injury alone; they are suffering from Central Sensitization, a state where the spinal cord itself has become a generator of pain.
What makes OIH distinct from tolerance is the direction of the pain threshold. In tolerance, the threshold for pain remains the same, but the drug's ability to reach that threshold diminishes. In OIH, the threshold for pain actually drops. The patient becomes "chemically sensitive," not just to the drug, but to their entire sensory environment. This is a profound biological "betrayal" because the clinician's instinct is to treat "breakthrough pain" with more opioids, which provides a fleeting moment of relief followed by a deeper plunge into hyper-sensitivity.
---
##
Mechanisms at the Cellular Level
At the microscopic scale, OIH is a masterclass in dysfunctional neuroplasticity. The transition from analgesia to hyperalgesia involves three primary cellular actors: the NMDA receptor, the Glial cells (specifically microglia and astrocytes), and the shift in chloride ion gradients.
The NMDA Receptor and Glutamate Excitotoxicity
The NMDA receptor is a glutamate-gated ion channel that plays a critical role in synaptic plasticity and memory. Under normal conditions, the NMDA receptor is blocked by a magnesium ion (the "magnesium plug"). However, chronic opioid use causes a sustained depolarisation of the post-synaptic membrane, which ejects the magnesium plug. This allows an uncontrolled influx of calcium ions into the neuron. This calcium influx triggers a secondary messenger cascade involving Protein Kinase C (PKC) and Nitric Oxide Synthase (NOS). These enzymes further sensitise the NMDA receptor, creating a feedback loop of excitation. The neuron is essentially "electrified," firing pain signals in response to the slightest provocation.
Glial Cell Activation: The Hidden Drivers
Perhaps the most significant discovery in the last decade of pain science is the role of non-neuronal cells. Microglia, the resident immune cells of the brain, possess receptors for opioids (specifically Toll-like Receptor 4 or TLR4). When opioids bind to TLR4, it signals the microglia that the brain is "under attack." The microglia shift from a protective, ramified state to an aggressive, amoeboid state, releasing a "cytokine storm" of pro-inflammatory molecules: Interleukin-1 beta (IL-1β), Interleukin-6 (IL-6), and Tumour Necrosis Factor-alpha (TNF-α).
These cytokines act directly on neurons to increase their excitability. Furthermore, astrocytes (star-shaped support cells) begin to hypertrophy and lose their ability to clear glutamate from the synaptic cleft. This leads to "glutamate spillover," where the neurotransmitter meant for one signal begins to excite neighbouring neurons, causing pain to radiate far beyond the original site of injury. This is why OIH often manifests as "diffuse" or "non-specific" pain that moves across the body.
The KCC2 Transporter and GABAergic Reversal
In a healthy adult nervous system, GABA is the primary inhibitory neurotransmitter. It acts as the "off switch." However, chronic opioid exposure causes a down-regulation of the KCC2 chloride transporter. This shift alters the internal chloride concentration of the neuron. When KCC2 is diminished, the opening of GABA-gated channels no longer allows chloride to flow *in* (which inhibits the cell); instead, it allows chloride to flow *out* (which excites the cell).
ALARMING FACT: Through the suppression of KCC2, opioids can literally turn the brain's "calming" system into an "exciting" system. The very mechanisms the brain uses to relax and dampen pain are hijacked to produce *more* pain.
---
##
Environmental Threats and Biological Disruptors
The tragedy of Opioid-Induced Hyperalgesia does not exist in a vacuum. A patient whose nervous system has been primed for hyper-excitability by opioids is uniquely vulnerable to environmental chemical stressors. This is the aspect of OIH that the MHRA has most aggressively ignored: the creation of a "Multiple Chemical Sensitivity" (MCS) phenotype through pharmaceutical intervention.
When the microglia are "primed" by opioids, they become hyper-reactive to other environmental triggers. This includes:
- —Volatile Organic Compounds (VOCs): Fragrances, cleaning chemicals, and new-carpet fumes that would be ignored by a healthy nervous system can trigger a systemic inflammatory response in an OIH sufferer.
- —Heavy Metals: Lead, mercury, and aluminium, which interfere with NMDA receptor function, can exacerbate the excitotoxic state already present in the OIH patient.
- —Electromagnetic Fields (EMF): Emerging research suggests that voltage-gated calcium channels (VGCCs) are sensitive to non-ionising radiation. In a system already suffering from calcium overload due to NMDA over-activation, EMF exposure can act as a secondary "trigger" for pain flares.
The OIH patient lives in a world where the "background noise" of modern life—the chemical and electronic soup of the 21st century—becomes a source of biological trauma. The pharmaceutical industry markets opioids as a way to "reclaim your life," yet for many, the drugs turn the external world into a minefield. This secondary sensitivity is rarely linked back to the opioid prescription, leading to further misdiagnosis and the "gaslighting" of patients who claim that their environment is making them sick.
---
##
The Cascade: From Exposure to Disease
The progression of OIH is a slow-motion car crash of the nervous system. It typically follows a predictable "cascade" of biological degradation:
- —The Acute Phase: The patient experiences genuine pain relief. The Mu-opioid receptors are successfully occupied, and the descending inhibitory pathways are reinforced.
- —The Compensation Phase: The brain begins to "push back." NMDA receptors are up-regulated, and endogenous opioid production (endorphins) is shut down via a negative feedback loop. The patient notices the drug "isn't working as well" (Tolerance).
- —The Activation Phase: Microglia and astrocytes transition to a pro-inflammatory state. They begin to secrete BDNF (Brain-Derived Neurotrophic Factor), which specifically causes the KCC2 transporter to fail. The "brakes" of the nervous system start to smoke and fail.
- —The Hyperalgesic Phase: The patient experiences "pain beyond the site." A back injury starts to feel like leg pain, neck pain, and headaches. The pain becomes "burning," "electric," or "stabbing"—hallmarks of neuropathic and central pain.
- —The Systemic Collapse: The patient develops "Chemical Sensitivity." Their sleep is destroyed as the brain can no longer enter the deep, inhibitory states required for glymphatic drainage (the brain's waste clearance system). This leads to "brain fog," cognitive decline, and profound depression.
At this final stage, the patient is often labelled as "difficult" or "somatising" by the medical establishment. Their complaints of global pain and sensitivity to light, sound, and smell are dismissed as psychological, when in fact they are the logical end-point of a chemically-induced neuro-inflammatory disease.
---
##
What the Mainstream Narrative Omits
The mainstream medical narrative, largely dictated by pharmaceutical marketing and reinforced by conservative regulatory bodies, omits the most damning truth: Opioids are not "painkillers"; they are "pain-shifters." They trade immediate, acute relief for long-term, systemic sensitivity.
The pharmaceutical industry spent decades promoting the "Pain as the 5th Vital Sign" campaign, which pressured doctors to eliminate all pain at any cost. This campaign relied on the "pseudo-addiction" myth—the idea that if a patient was seeking more drugs, it wasn't addiction, but "under-treated pain." This encouraged the escalation of doses precisely when the biological signs of OIH were beginning to manifest.
Furthermore, the mainstream narrative omits the "Dark Side" of the Mu-receptor. While the Mu-receptor provides euphoria and analgesia, its chronic activation leads to the recruitment of the Dynorphin system. Dynorphins are endogenous "anti-opioids" that bind to Kappa-receptors, producing dysphoria, anxiety, and—critically—increased pain sensitivity. The mainstream narrative treats opioids as if they exist in a vacuum, ignoring the fact that they trigger a massive counter-offensive from the body's own chemical arsenal.
The MHRA has also failed to mandate that clinicians distinguish between addiction and OIH. While they share some overlapping behaviours (like seeking more medication), their biological drivers are different. An addict seeks the "high"; an OIH sufferer seeks the "relief" from a pain that the drug itself is creating. By failing to highlight OIH, the MHRA allows doctors to continue "treating" the hyperalgesia with the very agent that caused it, a cycle that is as profitable for the industry as it is lethal for the patient.
---
##
The UK Context
In the United Kingdom, the opioid crisis has taken a different shape than in the United States, but the biological devastation is the same. The UK’s "North-South divide" is starkly visible in prescribing patterns. In regions like Blackpool, Middlesbrough, and the Scottish Rust Belt, opioid prescription rates are significantly higher than in the affluent South East. These areas are also witnessing a silent epidemic of chronic disability and "unexplained" pain syndromes.
UK STATISTIC: A 2019 review by Public Health England found that 1 in 4 adults in England were taking at least one potentially addictive prescription drug, with opioids being the most common for chronic pain. Despite this, the MHRA has only recently (2020) mandated "addiction" labels, still failing to provide clear, bold warnings regarding Hyperalgesia and Neuro-inflammation.
The MHRA’s "Yellow Card" scheme, intended to track adverse drug reactions, is woefully inadequate for capturing OIH. Because OIH presents as "more pain," it is almost always recorded by the GP as a "worsening of the underlying condition" rather than an adverse reaction to the medication. This creates a data vacuum where the MHRA can claim there is "insufficient evidence" of widespread OIH, simply because the reporting system is designed to miss it.
Furthermore, the National Institute for Health and Care Excellence (NICE) has recently updated its guidelines (NG193) to discourage the use of opioids for chronic primary pain. However, this leaves millions of "legacy patients"—those already on high doses for decades—in a state of medical abandonment. Without a deep understanding of the cellular biology of OIH, GPs are often ill-equipped to help these patients taper safely, often leading to rapid withdrawals that further traumatise an already hyper-sensitive nervous system.
---
##
Protective Measures and Recovery Protocols
Recovery from Opioid-Induced Hyperalgesia is not as simple as "stopping the pills." Because the nervous system has been physically rewired, the path back to a normal pain threshold requires a multi-pronged biological intervention aimed at resetting the NMDA/Glial axis.
1. The Ultra-Slow Micro-Taper
The most dangerous approach to OIH is the rapid taper. A hyper-sensitised nervous system interprets a drop in opioid levels as a life-threatening crisis, triggering a massive surge in glutamate and pro-inflammatory cytokines. A "Micro-taper," sometimes reducing the dose by as little as 1-5% per month, is often necessary to allow the KCC2 transporters to recover and the microglia to return to a "resting" state.
2. NMDA Antagonism
To break the cycle of excitotoxicity, the NMDA receptor must be stabilized. Substances like Magnesium Glycinate or Magnesium Threonate (which crosses the blood-brain barrier) can help re-establish the "magnesium plug." In clinical settings, low-dose Ketamine or Memantine (an Alzheimer's medication) are sometimes used off-label to "reset" the NMDA receptor's sensitivity.
3. Glial Stabilisers and Anti-Inflammatories
Reducing neuro-inflammation is paramount. Palmitoylethanolamide (PEA), a fatty acid amide, has shown significant promise in clinical trials for its ability to down-regulate mast cells and microglia. Low Dose Naltrexone (LDN) is another critical tool. While Naltrexone is an opioid antagonist at high doses, at "micro-doses" (1.5mg - 4.5mg), it briefly blocks the opioid receptors, triggering a rebound increase in endogenous endorphins and, crucially, acting as an anti-inflammatory agent on the TLR4 receptors of the microglia.
4. Antioxidant Support for the Mitochondria
OIH is an energy-demanding state for the neuron. The constant firing leads to oxidative stress and mitochondrial exhaustion. High-dose Alpha-Lipoic Acid (ALA), Coenzyme Q10, and N-Acetyl Cysteine (NAC) can help scavenge the reactive oxygen species generated by the "electrified" neurons, preventing further cellular damage.
5. Environmental De-stressing
Since the OIH patient is "chemically sensitive," recovery requires a "Low-Tox" environment. This means eliminating synthetic fragrances, minimizing processed food (which often contains glutamate-boosters like MSG), and practicing "sleep hygiene" to support the glymphatic system's ability to clear inflammatory debris from the brain.
---
##
Summary: Key Takeaways
Opioid-Induced Hyperalgesia is a testament to the arrogance of a medical model that views the human body as a collection of isolated parts rather than a dynamic, self-regulating system. For too long, the MHRA and the broader pharmaceutical establishment have treated pain as a volume knob that can be simply turned down with a chemical "off switch." The biological reality is that the body will always fight back to maintain its own version of balance.
- —The Paradox is Real: Chronic opioid use can directly cause the very pain it is meant to treat by lowering the nociceptive threshold.
- —Microglia are the Master Switches: OIH is not just a "nerve problem"; it is an immune system problem within the brain. The activation of microglia creates a pro-inflammatory environment that sustains pain.
- —The MHRA's Failure: By focusing on "addiction" while ignoring "hyperalgesia" and "chemical sensitivity," regulatory bodies have left millions of patients vulnerable to misdiagnosis and medical gaslighting.
- —Glutamate Excitotoxicity: The NMDA receptor is the primary engine of OIH. Successful treatment requires shifting the balance back from excitation to inhibition.
- —Recovery is Possible but Difficult: Restoring a damaged nervous system requires a slow, biological "reset" involving micro-tapering, NMDA stabilisation, and glial modulation.
The truth is that for many, the path to a pain-free life is not found at the bottom of a pill bottle, but in the painstaking work of quieting a nervous system that has been screaming for help. At INNERSTANDING, we believe that the first step to healing is the cold, hard recognition of the biological betrayal that has been allowed to flourish in the name of "modern medicine." It is time to listen to the silence of the MHRA and fill it with the voices of those who have been made more sensitive by the very drugs promised to protect them.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Opioid-induced hyperalgesia involves the activation of the N-methyl-D-aspartate (NMDA) receptor system and the modulation of spinal dynorphins, creating a state of nociceptive sensitization.
Morphine-induced hyperalgesia is driven by TLR4-mediated glial activation, which releases proinflammatory cytokines that amplify neural pain signaling.
Chronic exposure to xenobiotics and environmental pollutants can trigger central sensitization, potentially exacerbating the paradoxical pain responses seen in opioid-induced hyperalgesia.
Long-term opioid therapy for chronic pain lacks robust evidence of efficacy and is increasingly linked to neurobiological changes that heighten pain sensitivity.
Epigenetic modifications in the spinal cord, specifically histone acetylation, contribute significantly to the development and maintenance of opioid-induced hyperalgesia after chronic exposure.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Opioid Induced Hyperalgesia: The MHRA's Silence on Chemical Sensitivity"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper