
Pancreatic Elastase: Identifying Exocrine Insufficiency in Chronic Cases
Exocrine Pancreatic Insufficiency (EPI) results in undigested food reaching the small intestine, providing a feast for opportunistic bacteria. Testing for pancreatic elastase is a vital but underused diagnostic step in the UK.
Overview
The human digestive system is an intricate, fine-tuned biochemical refinery, yet its most pivotal architect is often the most neglected in clinical diagnostics: the pancreas. While mainstream medical discourse frequently fixates on the "gut microbiome" as an isolated entity, it fails to account for the upstream systemic failures that permit dysbiosis to occur. At the heart of this failure lies Exocrine Pancreatic Insufficiency (EPI)—a state where the pancreas fails to produce or secrete adequate digestive enzymes. When these enzymes, particularly those responsible for breaking down fats and proteins, are absent, the small intestine ceases to be a site of absorption and becomes a site of fermentation.
In the United Kingdom, we are currently witnessing a silent epidemic of chronic digestive distress, often dismissed under the umbrella term "Irritable Bowel Syndrome" (IBS). However, emerging data suggests that a significant percentage of these patients are actually suffering from undiagnosed EPI. The primary diagnostic tool for this condition, the Faecal Pancreatic Elastase-1 (FE-1) test, remains chronically underutilised by General Practitioners. This neglect is catastrophic; without sufficient pancreatic output, the Small Intestinal Bacterial Overgrowth (SIBO) remains incurable, as the "starving" bacteria are perpetually fed by the undigested macronutrients that the human host failed to process.
This article serves as a definitive exploration of the Pancreas-SIBO axis. We will dissect the cellular mechanics of enzyme production, the environmental toxins sabotaging pancreatic health, and the systemic failures of the UK healthcare model in addressing this root cause. Pancreatic elastase is not merely a marker of "digestion"; it is a sentinel for the entire integrity of the human metabolic engine.
##
The Biology — How It Works
The pancreas is a dual-purpose organ, performing both endocrine (hormonal) and exocrine (digestive) functions. While the endocrine side manages blood glucose via insulin and glucagon, the exocrine side—comprising roughly 95% of the organ’s mass—is responsible for the synthesis and secretion of the "Pancreatic Juice." This juice is a complex cocktail of water, electrolytes, and pro-enzymes (zymogens) that are essential for life.
The Three Pillars of Digestion
The exocrine pancreas secretes three primary classes of enzymes:
- —Proteases (e.g., Trypsinogen, Chymotrypsinogen): These break down proteins into peptides and amino acids.
- —Lipases: These are essential for the emulsification and absorption of dietary fats and fat-soluble vitamins (A, D, E, and K).
- —Amylases: These break down complex carbohydrates into simple sugars.
However, the secret weapon of the pancreas is Bicarbonate. The enzymes produced by the pancreas cannot function in an acidic environment. As the highly acidic "chyme" (partially digested food) leaves the stomach and enters the duodenum, the pancreas must flood the area with bicarbonate to neutralise the stomach acid. This shift from an acidic to an alkaline pH (roughly 7.0 to 8.0) acts as the "on switch" for digestive enzymes.
The Significance of Elastase-1
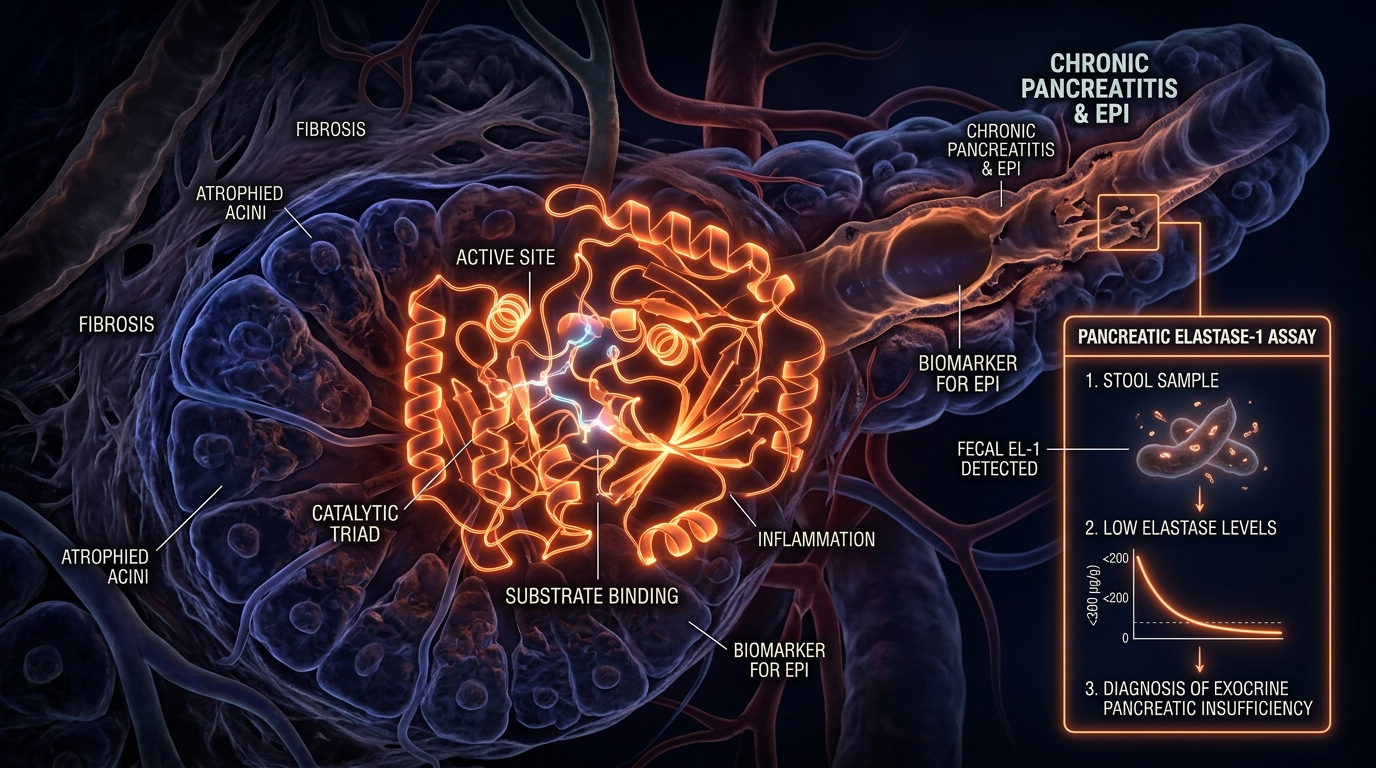
Among the suite of enzymes, Pancreatic Elastase-1 occupies a unique diagnostic position. Unlike other enzymes that are degraded during their passage through the intestinal tract, Elastase-1 remains remarkably stable. It binds to bile salts and passes through the gut largely intact. Therefore, its concentration in a stool sample serves as a direct, non-invasive proxy for the overall secretory capacity of the pancreas.
UK STATISTIC: It is estimated that up to 25% of patients diagnosed with "Diarrhoea-Predominant IBS" in the UK actually meet the clinical criteria for Exocrine Pancreatic Insufficiency, yet less than 5% are ever offered an Elastase test.
##
Mechanisms at the Cellular Level
To understand why the pancreas fails, we must look at the Acinar Cells. These are the functional units of the exocrine pancreas, responsible for protein synthesis on a massive scale. A single acinar cell can produce more protein than almost any other cell type in the human body.
Zymogen Granules and Controlled Activation
The pancreas faces a biological paradox: it must produce enzymes that digest flesh (proteases) without digesting itself. It solves this by producing these enzymes in an inactive state called zymogens, stored in "zymogen granules." Under normal conditions, these zymogens are only activated once they reach the duodenum, triggered by an enzyme called enterokinase.
In chronic cases of EPI, the cellular machinery of the acinar cells becomes compromised. This is often driven by calcium signalling dysfunction. Calcium is the primary messenger that triggers the release of these enzymes. When the cell is stressed—by toxins, hypoxia, or inflammation—calcium levels spike pathologically within the cell, causing the premature activation of enzymes *inside* the pancreas. This leads to micro-autodigestion and the eventual replacement of functional glandular tissue with fibrotic scar tissue.
The Role of CCK and Secretin
The communication between the gut and the pancreas is mediated by two key hormones: Cholecystokinin (CCK) and Secretin.
- —CCK is released by the duodenum in response to fats and proteins, signalling the acinar cells to dump their enzyme stores.
- —Secretin is released in response to acid, signalling the ductal cells to release bicarbonate.
In chronic SIBO cases, the "brush border" of the small intestine—the very lining where these hormones are produced—is often damaged (villous atrophy). This creates a vicious cycle: the damaged gut cannot signal the pancreas to produce enzymes, and the lack of enzymes causes further gut damage through the presence of putrefying, undigested food.
##
Environmental Threats and Biological Disruptors
The modern environment is inherently "anti-pancreatic." The pancreas is a highly metabolic organ with a high rate of blood flow, making it a primary target for systemic toxins and oxidative stress.
Glyphosate and the Synthesis Sabotage
The widespread use of glyphosate (the active ingredient in many UK herbicides) is a significant, yet ignored, factor in pancreatic decline. Glyphosate acts as an analogue to the amino acid glycine. The pancreas requires massive amounts of glycine to synthesise its enzymes. When glyphosate is substituted for glycine during protein synthesis in the acinar cells, it results in "misfolded proteins"—enzymes that are structurally defective and biologically useless. This is a primary driver of subclinical EPI that does not show up on standard imaging but manifests as a low Elastase-1 score.
Alcohol and Acetaldehyde
While the link between heavy drinking and pancreatitis is well-known, even "moderate" social drinking (highly prevalent in British culture) can induce chronic low-grade pancreatic stress. Alcohol is metabolised into acetaldehyde, which promotes the formation of "fatty pancreas" (non-alcoholic fatty pancreatic disease). This lipid accumulation within the pancreas displaces functional acinar cells, gradually eroding the organ's secretory reserve.
Heavy Metals: The Cadmium Connection
The pancreas has a peculiar affinity for Cadmium, a heavy metal found in industrial pollution and certain phosphate fertilisers used in UK agriculture. Cadmium mimics zinc, an essential mineral for pancreatic function. By displacing zinc, cadmium inhibits the production of carboxypeptidase and other vital enzymes, leading to a state of permanent "enzymatic poverty."
CALLOUT FACT: The pancreas contains the highest concentration of zinc in the human body. Without zinc, the synthesis of digestive enzymes and the storage of insulin both become biologically impossible.
##
The Cascade: From Exposure to Disease
The progression from "minor indigestion" to "Chronic Exocrine Insufficiency" is a multi-stage cascade that often takes years, meaning it is frequently missed by the "emergency-centric" NHS model.
Phase 1: The Bicarbonate Failure
The first stage is often not a lack of enzymes, but a failure of Bicarbonate output. If the secretin-mediated bicarbonate response is sluggish, the duodenum remains acidic. This deactivates what few enzymes are present. The patient experiences bloating and upper abdominal pressure, often misdiagnosed as "too much stomach acid" and incorrectly treated with Proton Pump Inhibitors (PPIs).
Phase 2: The Proteolytic Gap
As acinar cell function declines, protein digestion fails. Undigested protein (peptides) reaches the lower small intestine and the colon, where it undergoes putrefaction. This process releases toxic metabolites such as ammonia, phenols, and indoles. These compounds are highly inflammatory to the intestinal lining, increasing "leaky gut" (intestinal permeability).
Phase 3: The SIBO Feast
This is the critical juncture for SIBO. Opportunistic bacteria like *E. coli* and *Klebsiella* do not typically thrive in the small intestine because it is meant to be a nutrient-absorption zone, not a fermentation vat. However, when undigested carbohydrates and fats remain in the lumen, these bacteria have a constant food supply.
EPI is the primary reason for "Refractory SIBO"—cases where the patient takes antibiotics or herbals, feels better for two weeks, and then sees a total relapse. The bacteria return because the "table is still set" for them; the pancreas has failed to clear the substrate.
Phase 4: Nutrient Starvation and Systemic Decline
Eventually, the lack of fat-soluble vitamins (particularly Vitamin D and Vitamin A) leads to immune system collapse and poor mucosal integrity. The patient enters a state of "malnutrition in the midst of plenty," eating food but unable to extract its essence.
##
What the Mainstream Narrative Omits
The mainstream medical narrative regarding EPI is dangerously narrow. In the UK, the standard teaching is that EPI only occurs in cases of Cystic Fibrosis, Chronic Pancreatitis, or Pancreatic Cancer. This is a profound scientific oversight.
The "Subclinical" Trap
Mainstream diagnostics use a "cutoff" for Pancreatic Elastase. Usually, a score over 200 µg/g is considered "normal." This is a fallacy. In a healthy, high-functioning adult, the Elastase-1 score should be well over 500 µg/g.
- —200 - 500 µg/g: This range is often labelled "normal" by UK labs, but it represents Subclinical Pancreatic Insufficiency. Patients in this bracket are struggling; they have enough enzymes to survive, but not enough to maintain a healthy microbiome or prevent SIBO.
- —Under 200 µg/g: Clinical EPI.
- —Under 100 µg/g: Severe EPI.
By ignoring the 200-500 range, the NHS fails to catch the disease in its reversible stage, waiting instead for the organ to be 90% destroyed before intervening.
The PPI Paradox
The mainstream solution for "indigestion" is the prescription of Proton Pump Inhibitors (PPIs). This is arguably the worst possible intervention for someone with borderline pancreatic function. By suppressing stomach acid, PPIs remove the very trigger (acidic chyme) that signals the duodenum to release Secretin. Without Secretin, there is no Bicarbonate. Without Bicarbonate, any remaining pancreatic enzymes remain inactive. Thus, PPIs can chemically induce a state of exocrine insufficiency.
The Diabetes-Exocrine Link
Rarely discussed is the "Cross-Talk" between the endocrine and exocrine pancreas. People with Type 2 Diabetes or insulin resistance are at an exponentially higher risk for EPI. This is because insulin is a trophic hormone for the acinar cells—it helps them grow and maintain their function. When insulin signalling is broken, the exocrine tissue begins to atrophy. In the UK, where Type 2 Diabetes is soaring, we are ignoring the inevitable wave of pancreatic digestive failure that follows.
##
The UK Context
: A Systemic Failure
The British approach to pancreatic health is hampered by a "postcode lottery" and a fundamental lack of preventative testing.
The NHS Hurdle
On the NHS, a Faecal Elastase test is rarely the first line of enquiry. A patient presenting with bloating, flatulence, and fatty stools (steatorrhoea) will typically be tested for Celiac disease and Calprotectin (to rule out Crohn’s or Colitis). If those are negative, the patient is almost invariably told they have "IBS" and are advised to try a Low FODMAP diet.
This is a clinical dead end. A Low FODMAP diet may reduce the "fuel" for bacteria, but it does nothing to fix the underlying pancreatic deficiency. Furthermore, the NHS rarely offers the test unless the patient is showing signs of extreme weight loss, by which point the damage is often irreversible.
The Cost of Misdiagnosis
The economic burden of mismanaged "IBS" in the UK is staggering. Thousands of patients are trapped in a cycle of private consultations, ineffective supplements, and lost work days, all because a £50 Elastase-1 stool test was deemed "unnecessary" by their GP.
Moreover, the UK’s dependence on ultra-processed foods (UPFs) contributes to what researchers call "Pancreatic Burnout." The high levels of emulsifiers and refined oils in the British diet overstimulate the pancreas, leading to premature senescence of the acinar cells.
CRITICAL FACT: Unlike the liver, the pancreas has a very limited capacity for regeneration. Once acinar cells are replaced by fibrosis, that digestive capacity is lost forever. Early detection via Elastase-1 is the only way to "save" the organ.
##
Protective Measures and Recovery Protocols
If Pancreatic Elastase is low, the focus must shift from "killing bacteria" to "supporting the gland" and "replacing the lack."
1. Pancreatic Enzyme Replacement Therapy (PERT)
The cornerstone of treatment is PERT. This involves taking porcine-derived enzymes (such as Creon or Nutrizym in the UK) with every meal. However, the mainstream often gets the dosage wrong.
- —Timing is Critical: Enzymes must be taken *with* the first bite of food, not after the meal.
- —The Dose-Effect: Many patients are under-dosed. A typical meal requires 25,000 to 75,000 units of lipase to truly mimic physiological output.
- —Acid Protection: If the patient has low bicarbonate, the PERT enzymes may be destroyed by stomach acid before they reach the duodenum. In these cases, using an enteric-coated enzyme or supporting bicarbonate production is essential.
2. Stimulating the Cephalic Phase
Digestion begins in the brain. The Vagus Nerve is the "telephone line" that tells the pancreas food is coming. Modern "eating on the go" in the UK’s high-stress environment bypasses this cephalic phase.
- —Bitters: Using digestive bitters (like Gentian or Dandelion root) on the tongue 15 minutes before eating triggers the Vagus nerve to stimulate pancreatic secretion.
- —Thorough Mastication: Chewing food until it is liquid reduces the physical workload on the pancreas and increases the surface area for enzymes to work.
3. Micronutrient Support
- —Zinc Picolinate: Vital for enzyme synthesis.
- —Selenium: Protects the pancreas from oxidative damage and prevents fibrosis.
- —Magnesium: Required for the ATP-dependent secretion of enzymes.
4. Environmental Detoxification
Recovery is impossible if the pancreas is still being bombarded by disruptors.
- —Organic Diet: Specifically to avoid glyphosate, which sabotages enzyme protein folding.
- —Alcohol Cessation: Total abstinence for at least 6 months is often necessary to allow "fatty pancreas" to resolve.
- —Filtering Water: To remove heavy metals and fluoride, the latter of which can interfere with the pancreas’s ability to secrete bicarbonate.
5. Managing the SIBO-Pancreas Loop
If SIBO is present *because* of EPI, the SIBO will not clear until the enzymes are replaced. Use PERT as the "foundation" and then apply antimicrobial protocols. The enzymes themselves have an anti-biofilm effect, helping to break down the protective shields that bacteria build around themselves in the small intestine.
##
Summary: Key Takeaways
The exocrine pancreas is the "forgotten middle child" of gastroenterology, yet it holds the key to the UK’s chronic digestive crisis. Pancreatic Elastase-1 is the most vital, yet underutilised, diagnostic marker for anyone suffering from chronic SIBO, bloating, or malabsorption.
"The core truths of the Pancreas-SIBO axis are undeniable:"
- —The Proxy: Faecal Elastase-1 is a stable, reliable marker of pancreatic health, but "normal" ranges are often set too low. A score below 500 µg/g warrants investigation, not dismissal.
- —The Fuel: EPI provides the undigested substrate that makes SIBO inevitable and recurrent. You cannot "starve" SIBO if your pancreas is failing to digest your food.
- —The Environmental Sabotage: Glyphosate, heavy metals, and "social" drinking are silently eroding the British pancreatic reserve, leading to subclinical insufficiency.
- —The Bicarbonate Switch: Without an alkaline environment, enzymes are useless. Addressing the pH of the duodenum is as important as the enzymes themselves.
- —The Clinical Call to Action: In the UK, we must move beyond the "IBS" label. We must demand Elastase-1 testing and, where necessary, utilise high-dose PERT to break the cycle of fermentation and inflammation.
For the seeker of health, the message is clear: look upstream. The bugs in your gut are often just a symptom of a "lazy" or "poisoned" pancreas. By restoring the enzymatic fire of the exocrine system, we do more than just digest food; we restore the biological order of the entire human organism. The pancreas is not just a gland; it is the gatekeeper of our internal ecology. Only by respecting its complexity and protecting its function can we hope to resolve the chronic "gut issues" that have become the hallmark of modern British life.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Fecal elastase-1 testing is a highly sensitive non-invasive screening tool for detecting moderate to severe exocrine pancreatic insufficiency in clinical settings.
Chronic exocrine pancreatic insufficiency demonstrated by low fecal elastase-1 is strongly associated with the development of small intestinal bacterial overgrowth.
The systematic evaluation of pancreatic elastase facilitates the early diagnosis of exocrine insufficiency, preventing long-term complications related to maldigestion.
Fecal elastase-1 concentrations provide a reliable surrogate marker for exocrine function, allowing for effective monitoring of patients with chronic gastrointestinal disorders.
Insufficiency of pancreatic proteases and elastase leads to significant alterations in small intestinal motility and microbial composition, contributing to chronic SIBO.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Pancreatic Elastase: Identifying Exocrine Insufficiency in Chronic Cases"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.