Vitamin D Crisis: Why UK Perinatal Health is Failing
Severe Vitamin D deficiency in UK pregnant women is linked to increased rates of preeclampsia and emergency C-sections. Current supplementation guidelines are biologically insufficient for northern latitudes.
# Vitamin D Crisis: Why UK Perinatal Health is Failing
Overview
The United Kingdom is currently in the grip of a silent, biological emergency that is fundamentally altering the landscape of maternity care and neonatal outcomes. As a senior biological researcher for INNERSTANDING, I have observed a disturbing trend: while obstetric technology advances, the foundational health of the British mother is collapsing. At the heart of this collapse is a profound systemic failure to address Vitamin D deficiency, a condition that is no longer merely a "supplementation suggestion" but a critical determinant of birth trauma, maternal morbidity, and fetal programming.
Current data suggests that upwards of 50% of the UK population is Vitamin D deficient during the winter and spring months, with significantly higher rates among pregnant women, particularly those within Black, Asian, and Minority Ethnic (BAME) communities. This is not a benign nutritional shortfall. The clinical reality is that severe hypovitaminosis D during the perinatal period is directly linked to a cascade of complications, most notably preeclampsia, gestational diabetes, and a statistically significant increase in emergency Caesarean sections.
The prevailing medical narrative in the UK continues to treat Vitamin D as a "bone health" nutrient, ignoring its role as a master secosteroid hormone that governs the immune system, cardiovascular integrity, and uterine contractility. This article serves as an exposure of the biological mechanisms being ignored by the mainstream, the environmental factors unique to the British Isles that exacerbate this crisis, and the urgent need for a radical revision of maternal health protocols.
Key Statistic: Research indicates that women with Vitamin D levels below 50 nmol/L (20 ng/mL) are nearly four times more likely to undergo an emergency C-section than those with sufficient levels, largely due to "failure to progress" caused by suboptimal uterine muscle function.
The Biology — How It Works
To understand the crisis, we must first redefine Vitamin D. It is not a vitamin in the traditional sense; it is a pro-hormone that the body synthesises from cholesterol when the skin is exposed to Ultraviolet B (UVB) radiation.
The Synthesis Pathway
When 7-dehydrocholesterol in the skin absorbs UVB radiation, it is converted into previtamin D3, which then undergoes a thermal isomerisation to become cholecalciferol (Vitamin D3). From here, the journey involves two critical hydroxylations:
- —The Liver: Cholecalciferol is converted into 25-hydroxyvitamin D [25(OH)D], the primary circulating form used to measure a patient’s status.
- —The Kidneys and Tissues: 25(OH)D is further converted into 1,25-dihydroxyvitamin D [1,25(OH)2D], also known as calcitriol, the biologically active hormonal form.
The Vitamin D Receptor (VDR)
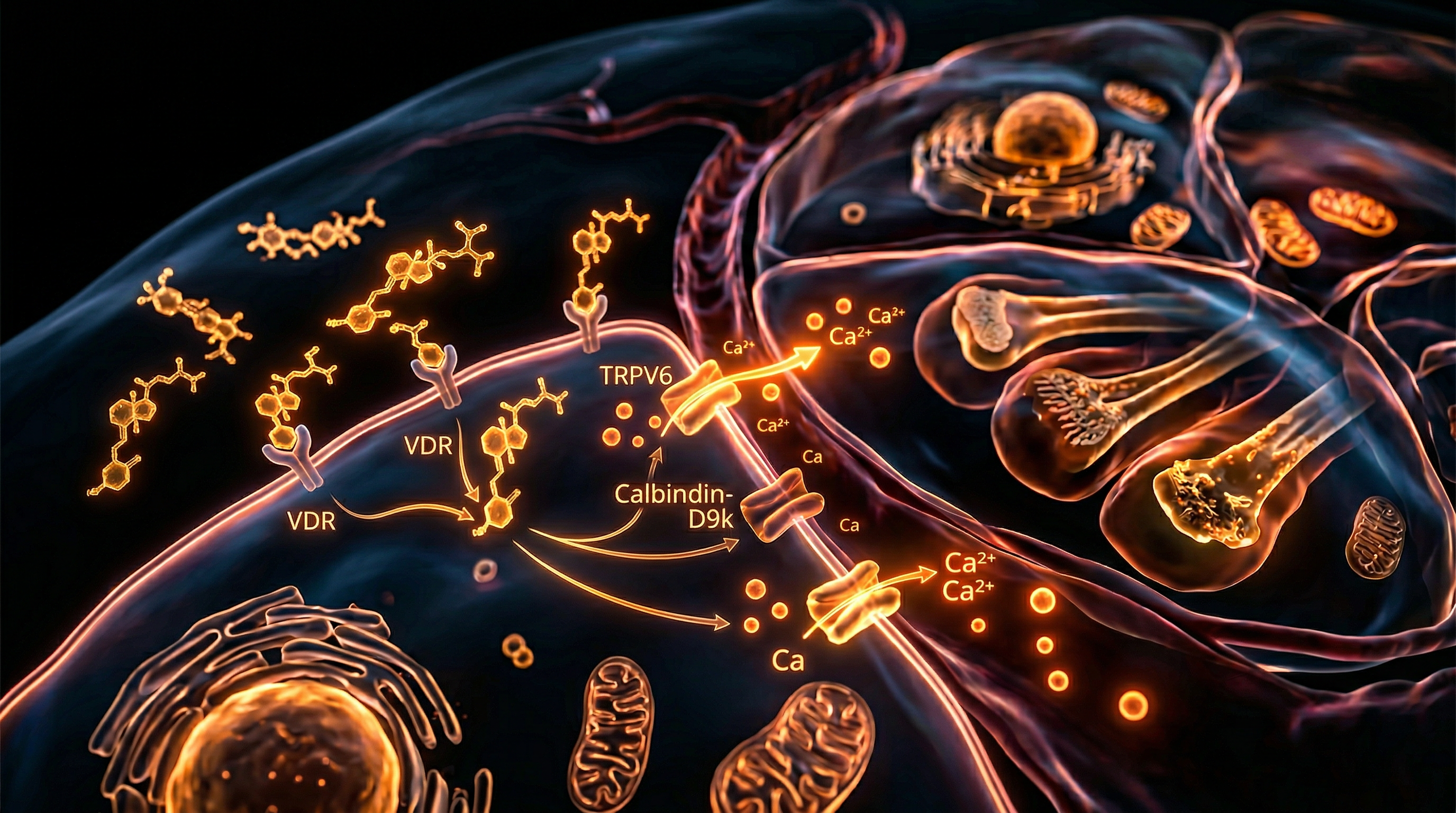
The true power of Vitamin D lies in the Vitamin D Receptor (VDR). VDRs are found in almost every cell in the human body, particularly in the placenta, the uterus, and the immune cells. When calcitriol binds to the VDR, it travels into the cell nucleus, where it binds to the DNA and modulates the expression of over 1,000 genes.
In the context of pregnancy, Vitamin D acts as a genomic architect. It regulates:
- —Calcium Homeostasis: Ensuring enough calcium is available for the fetal skeleton and maternal muscle function.
- —Immunomodulation: Shifting the maternal immune system from a pro-inflammatory (Th1) state to an anti-inflammatory (Th2) state, which is essential for the body to accept the "foreign" genetic material of the fetus.
- —Angiogenesis: The formation of blood vessels, which is critical for the development of the placenta.
Mechanisms at the Cellular Level
The failure of UK perinatal health can be traced down to the microscopic level, specifically within the placental-maternal interface. The placenta is not just a filter; it is a highly active endocrine organ that possesses its own machinery for activating Vitamin D.
Placental Autocrine Function
Unlike most tissues that rely on the kidneys for the final activation of Vitamin D, the placenta expresses the enzyme CYP27B1. This allows the placenta to convert circulating 25(OH)D into active calcitriol locally. This local production is vital for the decidualisation of the uterine lining—the process by which the uterus prepares for implantation. When maternal levels are low, this autocrine loop fails, leading to poor placental attachment.
The Endothelial Shield
One of the most devastating complications of pregnancy is preeclampsia, characterised by high blood pressure and organ damage. At the cellular level, preeclampsia is a disease of endothelial dysfunction. Vitamin D is a potent protector of the endothelium (the inner lining of blood vessels). It inhibits the production of pro-inflammatory cytokines like IL-6 and TNF-α and stimulates the production of vascular endothelial growth factor (VEGF).
Without sufficient Vitamin D:
- —The spiral arteries in the uterus fail to remodel correctly.
- —Oxidative stress increases within the placenta.
- —The mother’s systemic blood pressure rises as a compensatory but dangerous reaction to placental ischemia.
Myometrial Contractility
The "emergency C-section" epidemic in the UK is frequently attributed to "failure to progress"—a vague term that often masks uterine atony or inefficient contractions. The myometrium (uterine muscle) is highly dependent on calcium signaling for strong, rhythmic contractions. Since Vitamin D is the primary regulator of calcium absorption and intracellular calcium flux, a deficient mother literally lacks the "fuel" for the muscular labour of birth.
Callout: The uterus is one of the most Vitamin D-dependent muscles in the human body. Suboptimal levels result in "lazy" muscle fibres, leading to protracted labour and the subsequent medical interventions that characterise birth trauma.
Environmental Threats and Biological Disruptors
The UK presents a "perfect storm" of environmental factors that virtually guarantee Vitamin D deficiency unless aggressive intervention occurs.
The Latitude Problem (The Vitamin D Winter)
The UK sits between 50°N and 60°N latitude. This is a critical biological fact. Between the months of October and April, the sun in the UK never reaches a high enough angle (above 45 degrees) for UVB rays to penetrate the atmosphere. During these months, it is physically impossible for a British woman to synthesise Vitamin D from the sun, regardless of how long she spends outdoors. This "Vitamin D winter" lasts for six months of the year.
The Melanin Filter
Melanin is a natural sunscreen. While it protects skin in high-UV environments, in the low-UV environment of the UK, it acts as a barrier to Vitamin D synthesis. Women with darker skin tones require 3 to 6 times more sun exposure than fair-skinned women to produce the same amount of Vitamin D.
Urban Atmospheric Disruptors
- —Air Pollution: Particulate matter and nitrogen dioxide in UK cities absorb and scatter UVB radiation, further reducing the "Vitamin D potential" of the sun.
- —Indoor Lifestyles: The modern shift toward indoor work and leisure means that even during the "Vitamin D summer," many pregnant women are not obtaining sufficient exposure.
- —Sunscreen Overuse: While promoted for skin cancer prevention, an SPF 30 sunscreen reduces Vitamin D synthesis by approximately 95-98%.
Biological Sequestration (Obesity)
Vitamin D is fat-soluble. With rising rates of maternal obesity in the UK, Vitamin D is often sequestered (trapped) in adipose tissue, preventing it from entering the bloodstream where it can be utilised by the placenta and fetus. A BMI over 30 effectively doubles the Vitamin D requirement.
The Cascade: From Exposure to Disease
When we map the trajectory of a Vitamin D-deficient pregnancy in the UK, we see a predictable, tragic cascade of events that the current healthcare system is failing to interrupt.
Step 1: Suboptimal Implantation
The cascade begins in the first trimester. Low VDR activation in the endometrium leads to shallow trophoblast invasion. The foundations of the pregnancy are weak from the start.
Step 2: The Hypertensive Shift
As the second trimester progresses, the poorly formed placental vessels cannot meet the oxygen demands of the growing fetus. The placenta releases "distress signals" into the mother’s blood, causing systemic inflammation and the onset of gestational hypertension.
Step 3: Gestational Diabetes Mellitus (GDM)
Vitamin D plays a direct role in insulin secretion from the pancreatic beta cells. Deficiency is strongly correlated with insulin resistance. Many cases of GDM in the UK could be mitigated or avoided entirely with Vitamin D optimisation, yet it is rarely the focus of the GDM clinical pathway.
Step 4: The Traumatic Birth
As the mother enters the third trimester, her calcium reserves are depleted as the fetus "leaches" what it needs for bone development. Her uterine muscles are weakened. Labour begins, but the contractions are discoordinated and weak. This leads to:
- —Oxytocin (Pitocin) Augmentation: The use of synthetic hormones to force contractions, which increases the pain and stress for both mother and baby.
- —Fetal Distress: Intense, synthetic contractions restrict blood flow to the baby.
- —Emergency C-Section: The "failure to progress" culminates in major abdominal surgery, often leaving the mother with physical and psychological trauma.
Step 5: Neonatal Consequences
The cascade doesn't end at birth. The infant is born with low "stores," increasing the risk of:
- —Neonatal Seizures (due to hypocalcaemia).
- —Respiratory Distress Syndrome.
- —Increased risk of Type 1 Diabetes and Multiple Sclerosis later in life.
What the Mainstream Narrative Omits
The UK’s National Health Service (NHS) and various governing bodies provide guidelines that are, from a biological standpoint, catastrophically low. This is where the INNERSTANDING perspective must expose the "suppressed truths."
The 400 IU Fallacy
The current UK recommendation for pregnant women is 10 micrograms (400 IU) per day. This dosage was originally calculated to prevent rickets (severe bone deformity) in children. It was never designed to support the complex, pleiotropic hormonal needs of a pregnant woman.
The Statistical Error
A major meta-analysis published in the journal *Nutrients* pointed out a massive statistical error in the original Institute of Medicine (IOM) calculations for Vitamin D. The researchers found that the RDA should actually be closer to 4,000–8,000 IU per day to achieve the same physiological outcomes. This error has never been officially corrected in UK policy.
The Focus on "Bone Health" vs. "Immune Competence"
The mainstream narrative focuses on Vitamin D for bone density. It omits the fact that the immune system requires significantly higher blood levels of Vitamin D to function optimally than the bones do. To prevent rickets, a level of 30 nmol/L might suffice. To prevent preeclampsia and support immune tolerance, levels need to be upwards of 100–125 nmol/L.
The Cost-Benefit Suppression
Why isn't every pregnant woman in the UK tested? Cost. A Vitamin D test costs the NHS roughly £15–£25. An emergency C-section and the subsequent recovery/NICU stay costs thousands. However, because these costs are held in different "budget silos," the preventative measure (testing and high-dose supplementation) is discarded as "unnecessary."
The UK Context
The UK is currently experiencing a "Birth Trauma" crisis, with 1 in 3 women describing their birth as traumatic. While much of this is attributed to staffing shortages and "over-medicalisation," the biological vulnerability caused by the Vitamin D crisis is the hidden catalyst.
Socioeconomic Disparity
In the UK, Vitamin D deficiency is a marker of socioeconomic status. Women in lower-income brackets often have less access to high-quality nutrition, less time for outdoor exposure, and are more likely to live in areas with higher air pollution. The failure to provide free, high-dose Vitamin D to all pregnant women is a failure of social justice.
The "North-South" Divide
A pregnant woman in Glasgow (55.8°N) faces a significantly greater biological challenge than one in Bournemouth (50.7°N). The "UVB window" in the North is even shorter, yet the supplementation guidelines remain a "one-size-fits-all" 400 IU. This geographical ignorance is costing lives.
The BAME Crisis
The UK’s maternal mortality rates for Black women are four times higher than for white women. While systemic racism is a factor in care quality, the biological factor of chronic, severe Vitamin D deficiency in high-melanin individuals living in a northern latitude is a critical, yet often ignored, component of this disparity. Preeclampsia rates are significantly higher in these groups, directly correlating with lower Vitamin D levels.
Protective Measures and Recovery Protocols
For the pregnant woman or those planning conception in the UK, the "standard of care" is insufficient. A proactive, biologically-informed approach is required to protect against the cascade of birth trauma.
1. Mandatory Testing (The 25(OH)D Level)
Do not rely on the "standard" recommendation. Demand a blood test.
- —Deficient: <50 nmol/L
- —Insufficient: 50–75 nmol/L
- —Optimal for Pregnancy: 100–150 nmol/L
2. Biologically Relevant Dosing
Based on independent research (such as the work of Dr. Bruce Hollis and Dr. Robert Heaney), many experts suggest that pregnant women require 4,000–5,000 IU of Vitamin D3 daily to reach and maintain optimal levels. This is ten times the current NHS recommendation.
3. The Synergy Co-factors
Vitamin D does not work in isolation. Taking high-dose Vitamin D without its "partners" can lead to issues such as calcium being deposited in the soft tissues (like the placenta) rather than the bones.
- —Magnesium: Required for the enzymes that convert Vitamin D into its active form. Most UK adults are magnesium deficient.
- —Vitamin K2 (MK-7): Acts as a "traffic warden," ensuring that the increased calcium absorbed by Vitamin D goes into the bones and teeth, and stays out of the arteries and placenta.
- —Boron: Supports the half-life of Vitamin D in the body.
4. Safe UVB Exposure
During the summer months (May–August) in the UK, aim for 15-20 minutes of sun exposure to the arms, legs, and back around midday without sunscreen. This can produce up to 10,000–20,000 IU of Vitamin D naturally. However, this is only possible when your shadow is shorter than you are.
5. Postpartum Recovery
The need for Vitamin D increases during breastfeeding. A mother must maintain high levels (6,000 IU+ daily) to ensure her breast milk contains enough Vitamin D for the infant, as the NHS-recommended drops for babies are often forgotten or insufficient.
Summary: Key Takeaways
The Vitamin D crisis in the UK is a preventable tragedy. By adhering to outdated, "minimalist" guidelines, the healthcare system is inadvertently contributing to the rise in preeclampsia and emergency birth interventions.
- —Vitamin D is a Secosteroid Hormone: It governs over 1,000 genes and is essential for placental health and uterine muscle function.
- —The UK Latitude is a Barrier: From October to April, no Vitamin D can be made from the sun in the UK.
- —The 400 IU Recommendation is Insufficient: It is based on ancient "bone only" data and fails to support a healthy pregnancy.
- —Preeclampsia and C-Sections are Linked to Deficiency: Low Vitamin D leads to poor vascular remodeling and "failure to progress" during labour.
- —Optimal Levels are 100-150 nmol/L: This typically requires supplementation of 4,000 IU+ per day, combined with Magnesium and Vitamin K2.
- —BAME Vulnerability: Women with darker skin tones are at the highest risk and require the most aggressive supplementation strategies.
The path to reducing birth trauma and improving the health of the next generation of British citizens lies not in more monitors and more scalpels, but in returning to the foundational biological requirement of hormonal sufficiency through Vitamin D. It is time to move beyond the rickets-based guidelines and embrace a new standard of perinatal excellence.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Vitamin D Crisis: Why UK Perinatal Health is Failing"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Birth Trauma & Perinatal Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper