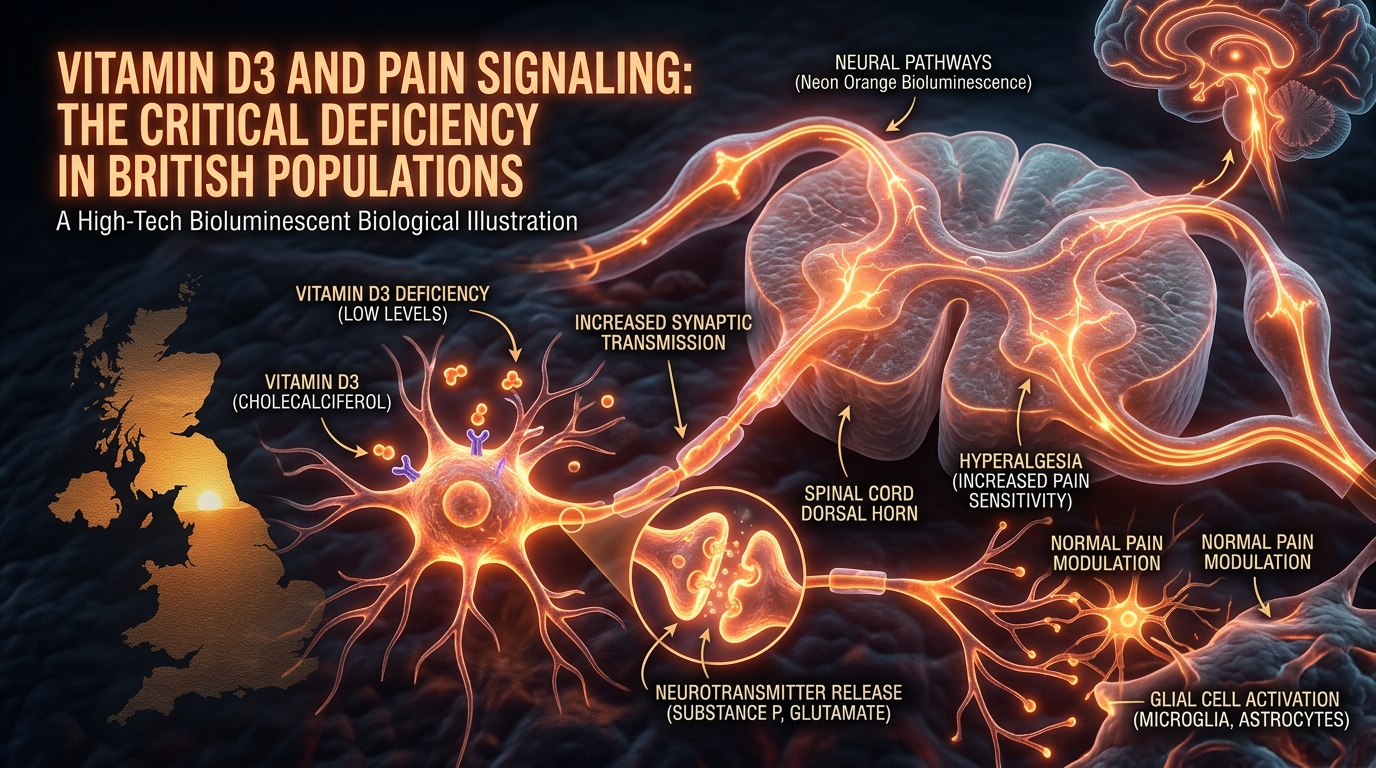
Vitamin D3 and Pain Signaling: The Critical Deficiency in British Populations
Low levels of Vitamin D are strongly correlated with chronic musculoskeletal pain and inflammatory markers. Given the UK's climate, this nutritional deficiency represents a significant, yet easily corrected, driver of systemic suffering.
Overview
The United Kingdom is currently weathering a silent, invisible, yet devastating public health crisis. It is not a viral pathogen or a sudden environmental catastrophe, but rather a chronic, systemic failure of biological regulation. Across the British Isles, millions of individuals are trapped in a cycle of persistent musculoskeletal pain, chronic fatigue, and inflammatory malaise. While the pharmaceutical industry offers a revolving door of analgesics, NSAIDs, and neuropathic agents, the biological reality is far simpler and more foundational: a profound, population-wide deficiency in the secosteroid hormone known as Vitamin D3 (Cholecalciferol).
In the context of modern British life, Vitamin D is frequently mischaracterised as a mere "supplemental" micronutrient, something to be considered for bone health or rickets prevention. This narrow view is a dangerous reductionism. Vitamin D3 is, in truth, a potent hormonal regulator that governs over 2,000 genes and serves as a master modulator of the human immune system and nociceptive (pain-sensing) pathways. When levels fall below a critical threshold—as they do for the vast majority of the UK population between the months of October and April—the body’s ability to regulate inflammation and suppress pain signals is fundamentally compromised.
This article serves as a comprehensive investigation into the intersection of Vitamin D3 endocrinology and pain science. We will explore why the British climate, coupled with modern architectural and lifestyle habits, has created a "perfect storm" for chronic pain. We will deconstruct the cellular mechanisms that turn a lack of sunlight into a surplus of suffering and expose why the current public health guidelines are not only insufficient but are actively contributing to the burden of disease. At INNERSTANDING, we believe that true health begins with an uncompromising look at the biological substrates of human existence.
UK FACT: According to data from the National Diet and Nutrition Survey (NDNS), approximately 1 in 6 adults in the UK have low serum levels of Vitamin D year-round, but during the winter months, this figure skyrockets, with nearly 40% of the population falling into the "deficient" category by clinical standards—and significantly more falling below "optimal" levels.
##
The Biology — How It Works
To understand the relationship between Vitamin D and pain, one must first appreciate the unique journey this molecule takes through the human body. Unlike other vitamins that are primarily ingested, Vitamin D is synthesized in the skin through a photochemical reaction. When ultraviolet B (UVB) radiation of a specific wavelength (290–315 nm) strikes the skin, it converts 7-dehydrocholesterol into pre-vitamin D3, which then thermally isomerises into Vitamin D3.
The Endocrine Pathway
Once synthesized or ingested, Vitamin D3 (Cholecalciferol) is biologically inert. It requires two successive hydroxylations to become active:
- —The Liver: Vitamin D3 is converted into 25-hydroxyvitamin D [25(OH)D], also known as Calcifediol. This is the primary circulating form used by clinicians to measure a patient’s Vitamin D status.
- —The Kidneys: Calcifediol is further hydroxylated into 1,25-dihydroxyvitamin D [1,25(OH)2D], known as Calcitriol. This is the potent, biologically active hormone that binds to the Vitamin D Receptor (VDR).
The Vitamin D Receptor (VDR)
The VDR is not limited to the gut or the bones; it is expressed in nearly every tissue in the body, including the brain, spinal cord, and sensory neurons. When Calcitriol binds to the VDR in the nucleus of a cell, it forms a complex with the Retinoid X Receptor (RXR). This complex then binds to Vitamin D Response Elements (VDREs) on the DNA, directly switching genes "on" or "off." In the context of pain, the VDR is highly concentrated in the Dorsal Root Ganglia (DRG)—the primary relay stations for pain signals travelling from the body to the central nervous system.
CRITICAL BIOLOGICAL FACT: Vitamin D is not just a nutrient; it is a genomic key. It directly regulates the expression of genes responsible for producing pro-inflammatory cytokines and neurotransmitters involved in pain transmission.
##
Mechanisms at the Cellular Level
The link between Vitamin D deficiency and pain is not merely observational; it is grounded in rigorous molecular biology. When Vitamin D levels are optimal, the hormone acts as a "braking system" for the inflammatory response. When levels are low, this brake is removed, leading to a state of Systemic Low-Grade Inflammation (SLGI) and Hyperalgesia (an increased sensitivity to pain).
Modulation of Cytokine Profiles
Vitamin D is a master regulator of the cytokine "storm." It inhibits the production of pro-inflammatory cytokines such as Interleukin-6 (IL-6), Tumour Necrosis Factor-alpha (TNF-α), and Interleukin-12 (IL-12). Simultaneously, it promotes the production of anti-inflammatory cytokines like Interleukin-10 (IL-10).
In the absence of sufficient D3, the balance shifts. Elevated TNF-α levels directly sensitise nociceptors, making them fire more easily in response to pressure or movement. This is why many British patients complain of "aching all over" during the winter; their cellular environment is literally primed for pain.
Glial Cell Activation and Central Sensitisation
One of the most profound discoveries in modern pain science is the role of Glial cells (microglia and astrocytes) in the spinal cord. Once thought to be mere "glue" for neurons, we now know they are the primary architects of chronic pain. When activated by injury or systemic inflammation, glia release substances that amplify pain signals, a process known as Central Sensitisation.
Vitamin D exerts a direct inhibitory effect on microglial activation. It prevents these cells from entering a pro-inflammatory state. Without D3, the microglia in the spinal cord become "hyper-excitable," magnifying every minor ache into a significant pain event. This is the biological basis for the transition from acute injury to chronic, intractable pain.
Nitric Oxide and Oxidative Stress
Vitamin D3 induces the expression of antioxidants and reduces the production of reactive oxygen species (ROS). It also regulates Nitric Oxide (NO) pathways. Excessive NO in the nervous system is linked to the development of neuropathic pain. By maintaining NO homeostasis, Vitamin D protects the delicate nerves from oxidative damage and prevents the "firing" of pain signals in the absence of a physical stimulus.
##
Environmental Threats and Biological Disruptors
The United Kingdom is geographically predisposed to Vitamin D deficiency, but our modern environment has exacerbated this natural disadvantage into a health catastrophe. The "Environmental Threat" to British Vitamin D levels is multi-faceted, involving latitude, atmospheric conditions, and the built environment.
The Latitude Problem (The 49th Parallel)
The UK lies between the latitudes of 50°N and 60°N. This is a critical geographical fact. From October to March, the sun in the UK never reaches a high enough angle in the sky (above 45 degrees) for UVB rays to penetrate the atmosphere effectively. During these months, even if a person stood outside naked at midday on a clear day, they would produce virtually zero Vitamin D. This period is known as the "Vitamin D Winter."
Atmospheric Extinction
In addition to latitude, the UK is plagued by persistent cloud cover and atmospheric pollution. These factors act as filters, further scattering and absorbing the already scarce UVB photons. In industrialised British cities, the "Atmospheric Extinction" of UVB can be up to 50% higher than in rural areas.
The Architectural Prison
Modern humans spend upwards of 90% of their time indoors. The transition from an agrarian, outdoor-based economy to an indoor, screen-based service economy has severed our ancestral connection to the sun. Furthermore, modern window glass—found in British homes, offices, and cars—is designed to block UVB radiation entirely while allowing UVA (which causes skin ageing and cancer) to pass through. We are effectively living in a biological shadow.
The Sunscreen Paradox
While the intention behind "sun safety" campaigns is noble, the over-application of high-SPF sunscreens has had an unintended side effect. An SPF 30 sunscreen reduces Vitamin D synthesis in the skin by more than 95%. In a climate like the UK's, where the window for synthesis is already narrow, the aggressive use of sunscreens during the few hours of peak summer sun can prevent a person from building the "reserves" needed to survive the winter.
ALARMING STATISTIC: A study by the University of Manchester found that during the peak of the British summer, only 25% of the population achieved "optimal" Vitamin D status, largely due to indoor lifestyles and sunscreen usage.
##
The Cascade: From Exposure to Disease
What happens when the body is chronically deprived of this secosteroid? The result is a physiological cascade that leads directly to the chronic pain clinics of the NHS. This process is often insidious, beginning with subtle changes and culminating in systemic dysfunction.
Stage 1: The Asymptomatic Depletion
Initially, the body draws on its fat stores for Vitamin D. As these stores dwindle, the parathyroid glands begin to work harder. They produce Parathyroid Hormone (PTH) to leach calcium from the bones to maintain blood calcium levels. At this stage, the individual may feel slightly more fatigued but generally "fine."
Stage 2: Myalgic Encephalopathy and Muscle Weakness
As 25(OH)D levels drop below 50 nmol/L, muscle tissue begins to suffer. Vitamin D is essential for the active transport of calcium into muscle cells, which is required for contraction and relaxation. Deficiency leads to Type II muscle fibre atrophy. The patient begins to feel "heavy-limbed," and minor physical tasks result in disproportionate muscle soreness.
Stage 3: Osteomalacic Myopathy (The Deep Ache)
This is the most critical stage for pain science. Long-term deficiency leads to Osteomalacia, or "softening of the bones." Unlike osteoporosis (which is painless until a fracture occurs), osteomalacia causes a dull, throbbing, deep bone pain. This is because the unmineralised bone matrix (osteoid) swells with fluid, stretching the sensitive periosteal lining of the bones. This is frequently misdiagnosed in the UK as Fibromyalgia or Chronic Fatigue Syndrome.
Stage 4: Neuropathic Sensitisation
Finally, the lack of Vitamin D's neuroprotective effects leads to the "wind-up" of the nervous system described earlier. The pain is no longer just in the muscles or bones; it is in the wiring itself. The individual becomes hypersensitive to cold, touch, and stress. This is the stage of "systemic suffering" where psychological distress and physical pain become inextricably linked.
##
What the Mainstream Narrative Omits
The current medical and nutritional consensus in the UK is, at best, outdated and, at worst, negligent. There are several critical "blind spots" in the mainstream narrative regarding Vitamin D and pain.
The RDA Fallacy
The UK government (via Public Health England and NICE) recommends a daily intake of 400 IU (10μg) of Vitamin D. For a senior researcher, this figure is laughable. 400 IU is the bare minimum required to prevent rickets (bone deformity) in children. It is nowhere near the amount required to maintain optimal serum levels for immune regulation or pain modulation in an adult. To reach an optimal serum level of 100-125 nmol/L, most adults in the UK climate require between 2,000 and 5,000 IU daily.
The Misunderstanding of "Normal" Ranges
UK laboratories often cite a "normal" range for Vitamin D starting at 50 nmol/L. However, "normal" is not "optimal." 50 nmol/L is simply the average of a deficient population. Research in the field of evolutionary medicine suggests that our ancestors, living in sun-drenched environments, had serum levels consistently above 100 nmol/L. By accepting 50 nmol/L as "sufficient," the medical establishment is essentially defining a state of "sub-clinical deficiency" as healthy.
The D2 vs. D3 Distinction
Many pharmaceutical preparations prescribed by the NHS contain Vitamin D2 (Ergocalciferol), derived from fungi. While D2 can raise serum levels, it is significantly less potent and has a shorter half-life than Vitamin D3 (Cholecalciferol), which is the form humans naturally produce. Furthermore, D2 has a lower affinity for the Vitamin D Binding Protein (VDBP), making it less effective at reaching target tissues like the brain and muscles.
The Ignored Co-factors
Vitamin D does not work in a vacuum. To be safely and effectively utilised, it requires Magnesium, Vitamin K2 (MK-7), Vitamin A, and Boron.
- —Magnesium: The enzymes that metabolise Vitamin D in the liver and kidneys are all magnesium-dependent. If a patient is magnesium-deficient (which 70% of the UK population is), taking high-dose Vitamin D will be ineffective and may even deplete magnesium further.
- —Vitamin K2: This is the "traffic cop" for calcium. Vitamin D increases calcium absorption; Vitamin K2 ensures that calcium goes into the bones and teeth, rather than the arteries or soft tissues.
INNERSTANDING REVELATION: The "Safe Upper Limit" of 4,000 IU cited by many health authorities is based on outdated studies and lacks a robust biochemical basis. Many clinical trials for chronic pain successfully use much higher doses (up to 10,000 IU) for short periods to "reset" the inflammatory system.
##
The UK Context
The UK represents a unique case study in nutritional neglect. The economic and social cost of our collective Vitamin D deficiency is staggering.
The NHS Burden
Chronic pain is one of the leading causes of GP visits in the UK. Millions of pounds are spent annually on prescription opioids like Codeine and Tramadol. These drugs carry high risks of addiction, respiratory depression, and paradoxical hyperalgesia (where the drug makes the pain worse). Correcting Vitamin D levels represents a low-cost, high-efficacy intervention that could theoretically save the NHS billions by reducing the need for these dangerous medications.
The Ethnic Disparity
This is perhaps the most overlooked aspect of the UK's health crisis. Individuals with darker skin (rich in melanin) require 3 to 5 times longer sun exposure than those with fair skin to produce the same amount of Vitamin D. In the UK, people of South Asian, African, and Afro-Caribbean descent are at an extreme disadvantage. Statistics show that Vitamin D deficiency in these communities can be as high as 90% during the winter months, correlating directly with the higher prevalence of chronic pain and metabolic disorders in these groups.
The "Cost of Living" Impact
Nutritional health is increasingly tied to socioeconomic status. While Vitamin D3 is relatively cheap, the "co-factors" (like high-quality magnesium and K2) and a diet rich in healthy fats (needed for D3 absorption) are becoming increasingly expensive. The poorest in British society are the most likely to live in high-density housing with limited access to green space, work long hours in indoor environments, and suffer from the most severe "nutritional poverty."
##
Protective Measures and Recovery Protocols
For those living in the UK, relying on "natural" sun exposure is not a viable strategy for year-round health. A proactive, scientifically grounded protocol is required to maintain optimal levels and manage pain signaling.
1. Precision Testing
Stop guessing. The only way to know your status is a 25(OH)D blood test. Aim for a serum level between 100 nmol/L and 150 nmol/L. If your GP refuses to test, private blood tests are widely available in the UK and are an essential investment for anyone suffering from chronic pain.
2. The Loading Dose Strategy
If you are severely deficient (e.g., <30 nmol/L), taking 400 IU a day will take years to bring you to optimal levels. Under medical supervision, a "loading dose" (e.g., 20,000–50,000 IU once a week for 6-8 weeks) may be necessary to saturate the tissues and "quench" the systemic inflammation before transitioning to a daily maintenance dose.
3. Mastering the Co-factors
Never take Vitamin D in isolation. Your protocol should include:
- —Magnesium: 300–400mg daily (Glycinate or Malate forms are best for muscle pain).
- —Vitamin K2 (MK-7): 100–200μg daily to ensure proper calcium distribution.
- —Healthy Fats: Vitamin D is fat-soluble. Take your supplement with the largest meal of the day, ensuring it contains healthy fats like avocado, olive oil, or grass-fed butter.
4. Strategic Sun Exposure
During the British summer (May to August), aim for "sensible" sun exposure. 15–20 minutes of midday sun on the arms, legs, and back without sunscreen is usually enough for fair-skinned individuals to produce significant Vitamin D. Once the skin begins to turn the slightest shade of pink, the "synthesis window" is closed, and any further exposure only increases the risk of damage.
5. Anti-Inflammatory Support
To specifically target the "pain" aspect of deficiency, consider pairing Vitamin D with Omega-3 Fatty Acids (EPA/DHA) and Curcumin. These work synergistically with the VDR to downregulate the NF-κB inflammatory pathway, providing a multi-pronged approach to pain management.
##
Summary: Key Takeaways
The relationship between Vitamin D3 and pain signaling is one of the most significant, yet under-utilised, frontiers in British medicine. The transition from a sun-exposed species to an indoor, high-latitude society has left our biological systems in a state of permanent "low-voltage" operation.
- —Vitamin D is a Hormone: It is a genomic regulator of the immune system and pain-sensing pathways, not just a bone-builder.
- —The UK is Deficient: Latitude and lifestyle make Vitamin D deficiency the default state for the British population.
- —Pain is a Signal: Chronic musculoskeletal pain and fibromyalgia are often the primary clinical manifestations of a "softening" of the bone matrix and a sensitisation of the central nervous system.
- —The RDA is Failed: The recommendation of 400 IU is an antique relic of rickets prevention and is insufficient for modern pain management.
- —Co-factors are Crucial: Magnesium and K2 are the essential partners that make Vitamin D therapy safe and effective.
At INNERSTANDING, we urge you to look beyond the surface level of symptomatic relief. Chronic pain is not merely a lack of Ibuprofen; it is often a cry for the biological substrates that define our evolutionary heritage. By reclaiming our Vitamin D status, we provide our bodies with the molecular tools necessary to dampen the fires of inflammation and return to a state of systemic equilibrium. In the grey, clouded landscape of the United Kingdom, Vitamin D3 is not a luxury—it is a physiological necessity for the preservation of human dignity in the face of suffering.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Research using the UK Biobank shows that vitamin D deficiency is a significant predictor of chronic pain and inflammation in the British population.
Vitamin D modulates pain pathways by regulating the production of pro-inflammatory cytokines and influencing the synthesis of neurotransmitters like serotonin.
Vitamin D deficiency promotes the development of mechanical hyperalgesia by increasing the density of sensory fibers in deep musculoskeletal tissues.
Low solar UVB exposure in the United Kingdom prevents adequate cutaneous vitamin D synthesis for most of the year, exacerbating chronic musculoskeletal conditions.
The vitamin D receptor acts as a genomic regulator of nociceptive signaling, with deficiency leading to increased sensitivity in peripheral pain receptors.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Vitamin D3 and Pain Signaling: The Critical Deficiency in British Populations"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper