
Next-Generation Lymphangiogenesis Therapies
Overview
Secondary lymphoedema represents a critical and often neglected survivorship challenge for patients who have undergone extensive cancer treatments, particularly axillary or inguinal lymph node dissection. This debilitating condition is characterised by the accumulation of protein-rich fluid in the interstitium, leading to chronic swelling, tissue fibrosis, and a heightened risk of recurrent infections. For decades, the standard of care has remained strictly palliative, relying on life-long compression therapy, manual lymphatic drainage, and meticulous skin care. However, these methods fail to address the underlying biological deficit: the irreversible loss of functional lymphatic vessels.
The Shift to Regenerative Solutions
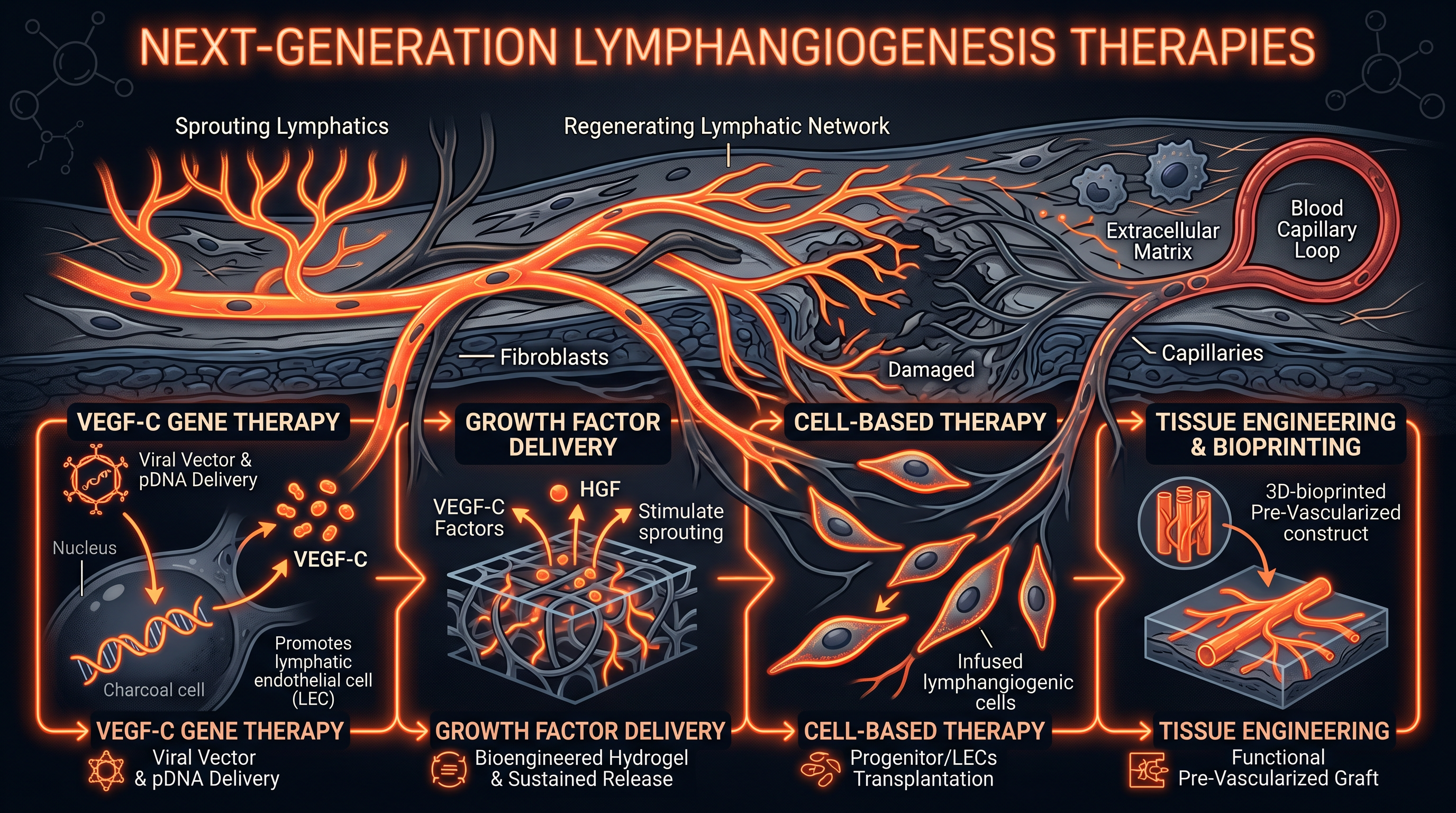
Recent advancements in molecular biology have catalysed a shift from palliative management to regenerative medicine, focusing on the de novo formation of lymphatic vessels, a process known as lymphangiogenesis. By leveraging the same biotechnological platforms that revolutionised vaccine development, researchers are now exploring how to 'restart' vessel growth in damaged tissues. The objective is to restore the biological drainage circuit, thereby providing a permanent physiological solution rather than a mechanical workaround. This briefing evaluates the front-line biological strategies currently under development to achieve this ambitious goal.
Therapeutic Modalities in Focus
Two primary technologies dominate the next-generation landscape: mRNA-based growth factor delivery and CRISPR-driven genetic modulation. These interventions aim to overcome the historical failures of protein therapy and viral-mediated gene transfer by offering superior safety profiles and precise control over cellular signalling. As we enter a new era of personalised oncology, the integration of these biological therapies into standard post-operative care could fundamentally alter the prognosis for millions of cancer survivors worldwide. This intelligence briefing explores the mechanisms, evidence, and clinical trajectories of these emerging interventions.
The therapeutic goal is not merely fluid drainage, but the biological restoration of a self-sustaining vascular circuit.
The Biology
The lymphatic system is a complex network of thin-walled vessels and nodes that serves as the body’s primary drainage and immune surveillance apparatus. Unlike the closed cardiovascular system, the lymphatic network begins as 'blind-ended' capillaries in the interstitial space, designed specifically to absorb fluid, large proteins, and migrating immune cells. These capillaries are composed of specialised Lymphatic Endothelial Cells (LECs) that exhibit unique 'oak-leaf' shapes and are anchored to the surrounding extracellular matrix by fine filaments. When interstitial pressure increases, these filaments pull the LEC junctions open, allowing fluid to enter the vessel lumen.
Structural Specialisation
Once fluid enters the initial lymphatics, it is transported into larger collecting vessels, which are structurally distinct and highly specialised. These collecting vessels possess a continuous basement membrane, are enveloped by a thin layer of smooth muscle cells, and contain intraluminal valves to prevent backflow. The rhythmic contraction of these vessels, aided by external skeletal muscle movements, ensures the unidirectional transport of lymph towards the thoracic duct. In post-cancer patients, the surgical removal of lymph nodes and the associated damage to these vessels disrupt this delicate hydrodynamic balance, leading to the clinical manifestation of lymphoedema.
Growth Factor Dependency
The primary driver of lymphatic growth and maintenance is the VEGF-C/VEGFR-3 signalling axis. Vascular Endothelial Growth Factor C (VEGF-C) is a secreted glycoprotein that binds with high affinity to the VEGFR-3 receptor, which is predominantly expressed on the surface of LECs. This binding triggers a cascade of intracellular events that promote LEC proliferation, migration, and survival. Without sufficient VEGF-C, or in the presence of obstructive scarring, the lymphatic network cannot regenerate effectively, making this pathway the central target for all emerging pro-lymphangiogenic therapies.
- —Initial Lymphatics: Blind-ended capillaries responsible for fluid uptake.
- —Collecting Vessels: Contractile vessels that transport lymph to the venous system.
- —LECs: The specialized endothelial cells that form the lymphatic wall.
- —VEGF-C: The master ligand for lymphatic vessel sprouting and growth.
Mechanisms at the Cellular Level
At the cellular level, the successful initiation of lymphangiogenesis requires a coordinated response from the LECs to external stimuli. When the VEGFR-3 receptor is activated by its ligand, it undergoes homodimerisation and autophosphorylation of specific tyrosine residues within its cytoplasmic domain. This activation recruits adaptor proteins that trigger the PI3K/AKT and ERK/MAPK pathways, which collectively govern the cellular machinery required for vessel sprouting. In the context of regeneration, these pathways must be stimulated with precise timing to ensure that new vessels are functional and stable.
Transcriptional Regulation
The master regulator of lymphatic identity is the transcription factor PROX1 (Prospero Homeobox 1). PROX1 expression is essential for maintaining the lymphatic phenotype and prevents LECs from reverting to a blood-vascular state. Emerging therapies aim to upregulate PROX1 expression to enhance the responsiveness of damaged tissues to growth factors. By modulating the epigenetic landscape of a cell, CRISPR-based interventions can potentially 'lock' LECs into a high-regeneration state, facilitating the rapid expansion of the capillary network in the weeks following surgical trauma.
The Role of Accessory Proteins
Effective lymphangiogenesis also depends on accessory proteins such as Neuropilin-2 and CCBE1. Neuropilin-2 acts as a co-receptor for VEGF-C, enhancing the sensitivity of the LEC to low levels of the growth factor. Meanwhile, CCBE1 (Collagen-and-calcium-binding EGF domains 1) is crucial for the proteolytic cleavage of pro-VEGF-C into its active form. Next-generation therapies are increasingly targeting these accessory mechanisms to maximise the efficacy of delivered growth factors, ensuring that the biochemical environment is optimised for vessel formation even in hostile, post-surgical conditions.
Precise control over the VEGFR-3 phosphorylation state is the fundamental requirement for orchestrating functional vessel growth.
Environmental Threats
The post-cancer environment is inherently hostile to lymphatic regeneration due to the legacy of oncological interventions. Surgery causes immediate mechanical disruption, but the long-term threat is often the result of adjuvant radiotherapy. Ionising radiation induces DNA damage in surviving LECs and the surrounding stroma, leading to a state of permanent cellular senescence. This 'bystander effect' prevents the local microenvironment from supporting new vessel growth, even if the primary growth factors are present, by creating a zone of biological exhaustion.
The Fibrotic Barrier
Chronic inflammation following surgery leads to the activation of myofibroblasts and the excessive deposition of collagen, resulting in tissue fibrosis. This fibrotic scarring increases the mechanical stiffness of the extracellular matrix, which physically hinders the migration of LECs. Furthermore, a dense, fibrotic matrix acts as a biochemical sink, sequestering growth factors and preventing them from reaching their target receptors on the LEC surface. Overcoming this physical and chemical barrier is one of the primary challenges for mRNA-based therapies that require efficient diffusion through the tissue to reach their cellular targets.
Hypoxia and Oxidative Stress
Areas affected by lymphoedema often suffer from chronic hypoxia and the accumulation of reactive oxygen species (ROS). While acute hypoxia can sometimes trigger VEGF expression through HIF-1α signalling, chronic oxidative stress in lymphoedematous tissue is predominantly destructive. It causes the degradation of the delicate basement membranes of newly forming vessels and promotes the transition of LECs into fibroblasts, a process known as Endothelial-to-Mesenchymal Transition (EndMT). This transformation further exacerbates the fibrotic cycle and permanently reduces the regenerative capacity of the limb.
- —Radiotherapy: Induces LEC senescence and prevents vessel sprouting.
- —Fibrosis: Creates a physical barrier that restricts cell migration and fluid flow.
- —EndMT: A pathological process where vessel cells turn into scar-forming cells.
- —ROS Accumulation: Causes oxidative damage to the protein-rich fluid stagnating in the limb.
The Cascade (exposure to disease)
The progression of secondary lymphoedema follows a predictable and devastating cascade that begins with the initial surgical or radiological insult. Immediately following lymph node removal, the limb experiences a phase of lymphatic hypertension, where the remaining vessels are unable to handle the normal volume of interstitial fluid. This pressure causes the vessels to dilate (lymphangiectasia), which eventually leads to the failure of the intraluminal valves. Once the valves fail, the unidirectional flow is lost, and lymph begins to reflux back into the distal tissues.
Fluid Stasis and Immune Activation
As the lymph stagnates, the protein-rich fluid triggers a sustained immune response, attracting CD4+ T cells and macrophages to the site. These immune cells secrete pro-inflammatory cytokines, most notably TGF-β1, which is the primary driver of tissue remodelling and fibrosis. The transition from fluid-based swelling to solid-tissue deposition is a critical turning point in the disease cascade. At this stage, the limb becomes progressively harder (pitting turns into non-pitting oedema), and the skin undergoes hyperkeratotic changes, often referred to as elephantiasis in its most severe form.
The Failure of Compensatory Mechanisms
In the early stages, the body attempts to compensate by upregulating local VEGF-C through inflammatory pathways, but this response is usually insufficient to bridge the gap in the lymphatic network. Over time, the chronic inflammatory milieu actually suppresses the VEGFR-3 receptor on LECs, rendering them 'deaf' to the body’s own regenerative signals. This creates a state of biological stalemate, where the disease becomes self-perpetuating even if the initial cause of the blockage is removed. Breaking this cycle requires a high-potency intervention that can override these inhibitory signals and force a regenerative response.
The transition from a fluid-based pathology to a fibrotic-tissue pathology marks the point where traditional therapies lose most of their efficacy.
Research Evidence
Recent clinical and preclinical studies have provided compelling evidence for the efficacy of mRNA-based delivery of VEGF-C. Unlike DNA-based gene therapy, mRNA does not require entry into the nucleus and does not carry the risk of genomic integration, making it an ideal candidate for transient growth factor expression. In porcine models of lymphoedema, the intradermal injection of mRNA encapsulated in lipid nanoparticles (LNPs) led to a significant increase in functional lymphatic vessel density. These newly formed vessels were shown to be capable of fluid transport, reducing limb volume by upwards of 30% compared to control groups.
CRISPR-a and Epigenetic Upregulation
Innovative research into CRISPR activation (CRISPR-a) has opened a new frontier in lymphangiogenesis. By using a 'dead' Cas9 (dCas9) fused to transcriptional activators, researchers can target the endogenous PROX1 or VEGFR-3 genes without cutting the DNA. This approach allows for a more physiological and sustained upregulation of the regenerative pathway than the delivery of exogenous proteins. Preliminary data from murine models indicate that a single CRISPR-a treatment can maintain elevated levels of lymphatic growth factors for several months, providing a prolonged window for vessel maturation and network integration.
Comparison of Delivery Vehicles
The choice of delivery vehicle remains a central focus of current research. While adenoviral vectors were used in early human trials (such as the Lymfactin study), concerns regarding immunogenicity and limited re-dosability have shifted focus toward synthetic LNPs. These nanoparticles can be engineered to target specific tissue depths, ensuring that the mRNA cargo is released exactly where the lymphatic capillaries are most needed. Furthermore, the transient nature of mRNA expression is now viewed as a safety feature, as it prevents the risk of over-proliferation and the formation of lymphatic malformations.
- —mRNA-VEGF-C: Provides a safe, transient burst of growth factor to initiate sprouting.
- —CRISPR-a: Enables the long-term 'turning on' of the body's own repair genes.
- —LNPs: Ensure the protection and targeted delivery of genetic cargo to the skin.
- —Lymfactin Study: Provided the first human proof-of-concept for lymphatic gene therapy.
The UK Context
In the United Kingdom, the management of lymphoedema is governed by a patchwork of specialised clinics within the National Health Service (NHS), often operating under severe resource constraints. The British Lymphology Society (BLS) has been vocal about the need for standardized care pathways and earlier intervention to prevent the development of late-stage fibrosis. Research in the UK is primarily driven by academic centres of excellence, such as the Institute of Cancer Research (ICR) and the Royal Marsden NHS Foundation Trust, which are at the forefront of combining surgical innovation with biological research.
Integration with the Genomic Medicine Service
The UK is uniquely positioned to lead in CRISPR-driven therapies due to the establishment of the NHS Genomic Medicine Service. This infrastructure provides a framework for the delivery of advanced therapy medicinal products (ATMPs) at scale. As CRISPR-a technologies move into Phase I/II trials, the UK’s ability to perform long-term longitudinal tracking of patients through centralised health records will be invaluable for assessing the durability of lymphatic regeneration. Collaboration between the NIHR (National Institute for Health and Care Research) and biotechnology firms is currently accelerating the translation of these therapies from lab to clinic.
Challenges in the UK Landscape
Despite the scientific potential, the UK faces challenges in ensuring equitable access to these high-tech biological solutions. The high cost of mRNA and CRISPR-based treatments requires a robust health technology assessment by NICE (National Institute for Health and Care Excellence) to justify their adoption over traditional compression garments. However, advocates argue that the long-term cost savings—achieved by reducing the frequency of hospitalisations for cellulitis and eliminating the need for life-long supplies—would make these regenerative therapies a cost-effective alternative for the NHS.
The UK’s existing genomic infrastructure provides a world-class platform for the clinical rollout of gene-modulating lymphatic therapies.
Protective Measures
As we await the full clinical availability of mRNA and CRISPR therapies, the focus remains on 'lymphatic-sparing' and 'lymphatic-reconstructive' measures during initial cancer surgery. The most prominent of these is the Lymphatic Microsurgical Preventive Healing Approach (LYMPHA), where surgeons perform immediate lymphovenous bypasses at the time of node dissection. This proactive measure aims to provide an alternative drainage route before the disease cascade can even begin, significantly reducing the incidence of secondary lymphoedema in high-risk patients.
Advanced Imaging and Screening
Early detection is the most effective protective measure against the irreversible stages of the disease. The use of Indocyanine Green (ICG) Lymphography allows clinicians to visualise lymphatic flow in real-time, identifying areas of dermal backflow and valvular failure long before physical swelling becomes apparent. In the UK, the adoption of bioimpedance spectroscopy (such as the L-Dex system) is becoming more common, allowing for the detection of sub-clinical fluid changes. This 'pre-clinical' window is the optimal time for the administration of future biological therapies, as the tissue environment is still receptive to growth signals.
Holistic Risk Mitigation
Beyond surgical and biological interventions, patient education on risk mitigation remains paramount. This includes the avoidance of skin trauma, the management of body mass index (BMI), and the early treatment of any signs of infection. High BMI is particularly detrimental to lymphatic function, as adipose tissue provides both a physical load on the vessels and a source of pro-inflammatory adipokines that suppress lymphangiogenesis. The future of lymphoedema protection will likely involve a multi-modal approach: immediate surgical reconstruction followed by a 'booster' of mRNA-VEGF-C to ensure the success of the new connections.
- —LYMPHA: Preventive microsurgery performed during the initial tumour removal.
- —ICG Lymphography: Real-time imaging to detect early lymphatic failure.
- —L-Dex: A non-invasive tool for measuring sub-clinical fluid accumulation.
- —BMI Management: Essential for reducing the mechanical and inflammatory load on the system.
Key Takeaways
The landscape of lymphoedema treatment is undergoing a fundamental transformation from symptomatic management to biological cure. The discovery of the VEGF-C/VEGFR-3 axis has provided the blueprint for regeneration, while mRNA and CRISPR technologies have provided the tools to execute it. We are moving away from the era of 'managing' the swelling and towards an era of 'rebuilding' the network. This shift promises to restore quality of life to cancer survivors who have long lived with the hidden burden of this disease.
Future Outlook
The next decade will likely see the first approved biological therapies for lymphoedema, with mRNA leading the way due to its safety and ease of production. CRISPR-driven interventions will follow, offering a more permanent solution for those with extensive tissue damage or genetic predispositions. The integration of these therapies with advanced microsurgery will represent the gold standard of care. This synergy between surgery and biology is the key to finally overcoming the physiological barriers that have hindered lymphatic recovery for over a century.
Summary of Intelligence
Secondary lymphoedema is a progressive, inflammatory, and fibrotic disease that requires a multi-faceted biological intervention. Current evidence strongly supports the use of VEGF-C delivery to stimulate LEC proliferation and vessel sprouting. However, the hostile post-cancer microenvironment must be addressed through early detection and the mitigation of fibrosis. As research continues to mature, particularly within the UK’s robust clinical trial ecosystem, the prospect of a functional cure for post-cancer lymphoedema is closer than ever before.
- —Regeneration over Palliation: The central theme of next-generation research.
- —Technology Synergy: Combining mRNA, CRISPR, and microsurgery for optimal results.
- —Early Intervention: The critical factor in ensuring biological receptivity.
- —UK Leadership: Utilizing the NHS genomic framework to pioneer clinical translation.
The eradication of chronic lymphoedema is no longer a question of 'if', but a question of 'when' these biological tools are integrated into the surgical suite.