Chemical Photosensitivity: The Hidden Risks of Common Medications Under UV Exposure
A clinical review of how antibiotics and NSAIDs trigger phototoxic reactions in human skin.
Overview
The phenomenon of chemical photosensitivity represents a complex intersection of pharmacology and photobiology, where seemingly inert pharmaceutical compounds undergo structural or energetic transitions upon exposure to ultraviolet (UV) or, occasionally, visible radiation. Within the framework of INNERSTANDIN’s investigative clinical analysis, we identify this condition not as a monolithic entity, but as a dual-pathway mechanism consisting of phototoxicity and photoallergy. While both result in cutaneous pathology, their underlying molecular kinetics and immunological implications differ profoundly, necessitating a high-resolution understanding of the dermal-drug interface.
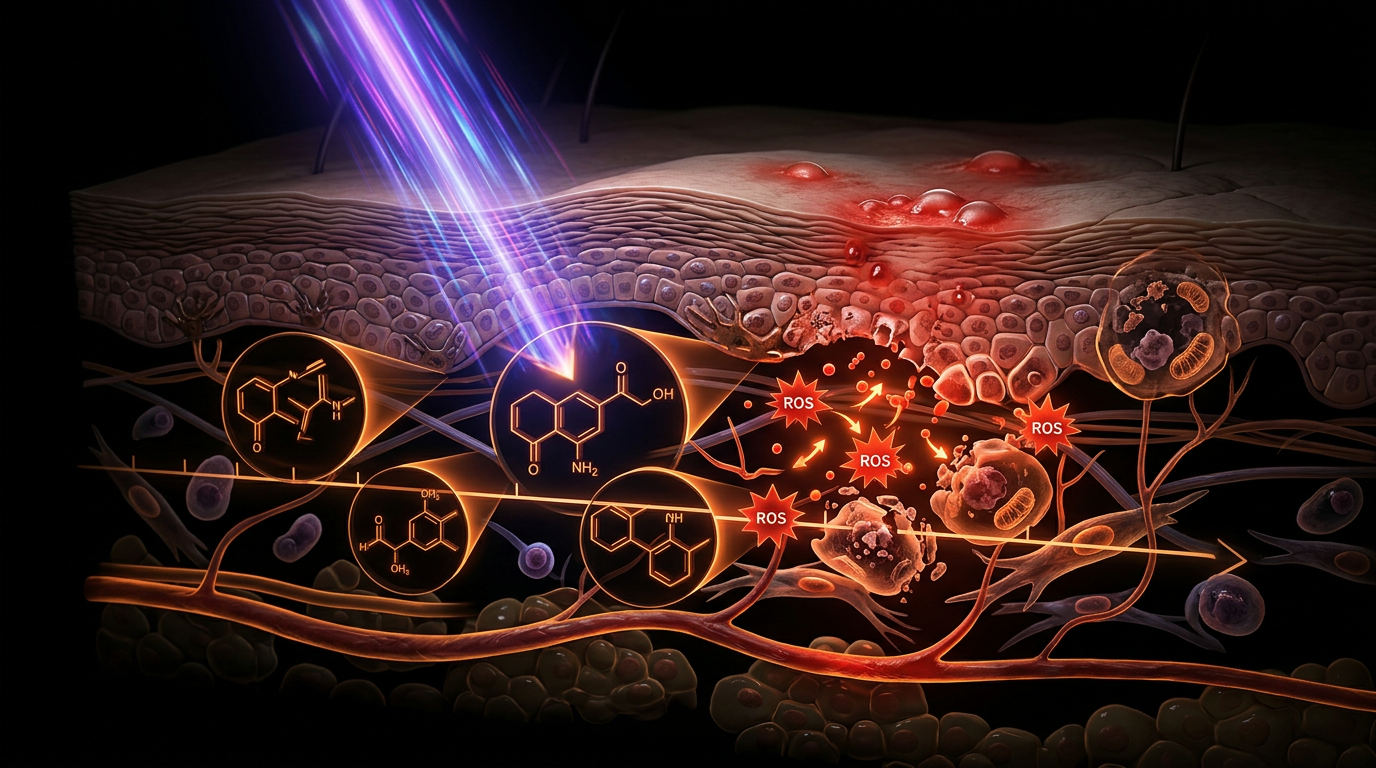
Phototoxicity, the more prevalent of the two, is fundamentally a non-immunological reaction. It occurs when a drug, acting as an exogenous chromophore, absorbs photons—typically within the UVA spectrum (320–400 nm), which penetrates deeper into the dermis than UVB. This absorption facilitates an electronic transition of the drug molecule from a ground state to an excited triplet state. As these molecules return to their basal energy level, they transfer energy to molecular oxygen, generating singlet oxygen ($^1O_2$), hydroxyl radicals, and superoxide anions. These Reactive Oxygen Species (ROS) instigate immediate oxidative damage to cellular organelles, lysosomal membranes, and nucleic acids. Research archived in *The Lancet* and indexed via PubMed underscores that drugs like tetracyclines, thiazide diuretics, and non-steroidal anti-inflammatory drugs (NSAIDs) such as naproxen, exhibit a dose-dependent phototoxic potential. This can lead to acute keratinocyte apoptosis and a profound inflammatory response that mimics severe thermal burns.
Conversely, photoallergy involves a Type IV delayed-type hypersensitivity reaction. In this scenario, UV radiation facilitates the photochemical conversion of a medication—or its metabolite—into a reactive hapten. This hapten then binds covalently to endogenous skin proteins, forming a complete antigen that is subsequently processed by Langerhans cells. Upon re-exposure, a T-cell-mediated immune response is ignited. Unlike phototoxicity, photoallergy is not dose-dependent and can manifest as a generalised eczematous eruption extending far beyond the site of UV exposure, indicating a systemic immunological priming.
In the United Kingdom, the clinical burden of photosensitivity is significant, yet frequently misdiagnosed as simple solar erythema. Data from the Medicines and Healthcare products Regulatory Agency (MHRA) Yellow Card Scheme suggests a substantial under-reporting of these adverse drug reactions (ADRs). At INNERSTANDIN, we emphasise that the systemic impact of these interactions extends beyond epidermal damage; the resultant pro-inflammatory cytokine cascade—involving TNF-α and IL-1—can exacerbate underlying autoimmune conditions and compromise the integrity of the dermal-epidermal junction. Mastery of these biochemical pathways is paramount for mitigating the risks associated with the increasingly polypharmaceutical landscape of modern British medicine.
The Biology — How It Works
To comprehend the systemic vulnerability of the human organism to drug-induced photosensitivity, one must first dissect the sub-cellular choreography that occurs when exogenous chemical agents meet ultraviolet radiation (UVR). At the core of this phenomenon lies the "photosensitiser"—a molecule, often a routine pharmaceutical agent, capable of absorbing photons and transitioning into a high-energy "excited" state. Within the framework of INNERSTANDIN’s rigorous biological scrutiny, we must distinguish between the two primary pathways: phototoxicity and photoallergy. While both are triggered by the electromagnetic spectrum (primarily UVA, 320–400 nm), their molecular ontogeny and clinical manifestations differ radically.
Phototoxicity represents a non-immunological, dose-dependent reaction. When a drug molecule—such as a fluoroquinolone or a tetracycline—absorbs UVR, it undergoes intersystem crossing to reach a long-lived triplet state. In this state, the molecule transfers energy directly to molecular oxygen ($O_2$), generating singlet oxygen ($^1O_2$), or transfers electrons to produce reactive oxygen species (ROS) like superoxide anions ($O_2^{\bullet-}$) and hydroxyl radicals ($\bullet OH$). This process, known as the Type II photochemical reaction, initiates a cascade of lipid peroxidation within the cellular and mitochondrial membranes of keratinocytes. Research published in the *British Journal of Dermatology* indicates that this oxidative stress leads to the immediate destruction of lysosomal membranes, releasing proteolytic enzymes that cause rapid cellular necrosis. In the UK context, where drugs like Naproxen and Amiodarone are frequently prescribed, this "sunburn-on-steroids" effect is often misattributed to simple solar overexposure, masking the underlying chemical provocation.
Conversely, photoallergy is a cell-mediated, Type IV delayed hypersensitivity reaction. Here, the drug acts as a pro-hapten. Upon UV exposure, the chemical undergoes a structural transformation or binds covalently to endogenous skin proteins to form a complete antigen. These "photoantigens" are then processed by Langerhans cells (cutaneous dendritic cells) and presented to T-lymphocytes in the regional lymph nodes. This sensitisation phase ensures that subsequent exposure, even at sub-toxic doses, triggers a systemic inflammatory response. Evidence from *The Lancet* suggests that photoallergic reactions are becoming increasingly prevalent due to the rise in topical NSAIDs and certain sunscreen filters (like oxybenzone), which can cross-react with systemic medications.
Crucially, the biological impact extends beyond the epidermis. At INNERSTANDIN, we recognise that chemical photosensitivity is not merely a cutaneous inconvenience; it is a catalyst for genomic instability. The presence of photosensitisers significantly lowers the threshold for the formation of cyclobutane pyrimidine dimers (CPDs) and 6-4 photoproducts in DNA. By facilitating these mutagenic lesions at lower UV doses than would naturally occur, common medications effectively act as indirect carcinogens. This synergy between systemic pharmacology and environmental radiation represents a profound, yet frequently overlooked, challenge to cellular homeostasis and long-term dermatological health.
Mechanisms at the Cellular Level
To grasp the profound implications of drug-induced photosensitivity, one must look beyond the superficial erythema and interrogate the sub-cellular choreography initiated by photon absorption. At the heart of this pathology lies the interaction between exogenous chromophores—medications or their metabolites—and ultraviolet radiation (UVR), typically within the UVA spectrum (320–400 nm). Unlike endogenous chromophores like melanin, these pharmaceutical agents possess molecular structures, often containing tricyclic or sulfonamide groups, that allow them to absorb photons and transition from a stable ground state to an electronically excited singlet or triplet state. This transition is the catalyst for two distinct but often overlapping biochemical pathways: phototoxicity and photoallergy.
Phototoxicity, the more prevalent mechanism, is an acute, non-immunological reaction that occurs upon the first exposure to a sufficient dose of both the drug and UVR. This process is governed by Type I and Type II photochemical reactions. In Type I reactions, the excited sensitiser undergoes electron or hydrogen transfer directly with cellular substrates—such as lipids in the keratinocyte membrane or nucleic acids—generating free radicals including superoxide anions ($O_2^{ \bullet -}$). In Type II reactions, the excited triplet-state drug transfers energy to molecular oxygen, generating highly reactive singlet oxygen ($^1O_2$). These Reactive Oxygen Species (ROS) initiate a cascade of oxidative stress, most notably lipid peroxidation of the plasma and lysosomal membranes. When lysosomal membranes rupture, proteolytic enzymes are released into the cytoplasm, inducing rapid cellular autolysis and triggering a potent inflammatory response via the release of arachidonic acid metabolites and pro-inflammatory cytokines such as IL-1 and TNF-$\alpha$. Research published in *The Lancet* and various photobiological journals highlights that common NHS-prescribed medications, such as ciprofloxacin and amiodarone, act through these exact oxygen-dependent mechanisms, leading to significant DNA strand breaks and mitochondrial dysfunction.
Photoallergy, conversely, represents a Type IV delayed-type hypersensitivity reaction. Here, the drug acts as a pro-hapten. UVR provides the energy required to chemically transform the drug into a reactive hapten, which then covalently binds to endogenous cutaneous proteins to form a complete antigen. This complex is processed by Langerhans cells—the sentinel dendritic cells of the epidermis—which migrate to regional lymph nodes to prime T-lymphocytes. Subsequent exposure, even at sub-toxic doses, triggers a systemic recruitment of cytotoxic T-cells back to the skin, manifesting as an eczematous eruption that can extend beyond the sun-exposed areas.
At INNERSTANDIN, we expose the reality that these cellular disruptions are not isolated to the epidermis. The systemic circulation of photosensitising agents means that the vascular endothelium and circulating leucocytes are also vulnerable to photo-oxidative stress. The molecular reality is a state of "electronic instability" where the medication, meant to heal, becomes a transducer for solar energy, turning the body’s own biochemical architecture into a site of self-inflicted oxidative damage. This necessitates a rigorous re-evaluation of how clinicians in the UK manage polypharmacy in an era of increasing UV intensity.
Environmental Threats and Biological Disruptors
The convergence of exogenous pharmacological agents and solar ultraviolet radiation (UVR) represents a potent, yet frequently overlooked, challenge to human biological homeostasis. Within the rigorous frameworks established by INNERSTANDIN, we must categorise these interactions not merely as "side effects," but as profound biochemical disruptions that destabilise cellular integrity. Chemical photosensitivity, bifurcated into phototoxicity and photoallergy, involves the transformation of relatively inert drug molecules into reactive, cytotoxic species upon the absorption of specific photon energies, primarily within the UVA spectrum (320–400 nm).
The primary mechanism of phototoxicity is an acute, non-immunological reaction. When a photosensitising medication—such as the widely prescribed tetracyclines (e.g., doxycycline) or thiazide diuretics used extensively within NHS protocols—reaches the dermis or epidermis, it acts as an exogenous chromophore. Upon irradiation, these molecules undergo electronic excitation to a triplet state. This excited state facilitates Type I or Type II photochemical reactions, culminating in the prolific generation of Reactive Oxygen Species (ROS), including singlet oxygen and superoxide radicals. Research published in *The Lancet* and various photobiology journals highlights that this oxidative deluge causes immediate damage to lysosomal and mitochondrial membranes. The resulting "leaky" cellular architecture triggers an inflammatory cascade, manifesting as exaggerated erythema that can mimic a severe thermal burn, yet its origin is purely molecular and oxygen-dependent.
Conversely, photoallergy represents a complex Type IV delayed-hypersensitivity reaction. Here, the UVR-induced transformation of a drug molecule creates a hapten which then binds to endogenous proteins to form a complete antigen. This process, often seen with topical NSAIDs or certain fragrances, recruits Langerhans cells to initiate a systemic T-cell mediated immune response. Unlike phototoxicity, which is dose-dependent and occurs upon first exposure, photoallergy reflects a deep-seated immunological memory, meaning subsequent minimal exposures can trigger widespread eczematous eruptions far beyond the site of initial UV contact.
The environmental threat is exacerbated by the UK’s specific atmospheric conditions; despite lower UVB levels in winter, UVA—the primary driver of photosensitivity—remains constant and penetrates glass, posing a silent risk to patients in indoor or vehicular environments. Furthermore, emerging data in *Nature Communications* suggests that chronic, low-grade drug-induced photosensitivity may contribute to accelerated photoageing and a heightened risk of non-melanoma skin cancers (NMSC). By disrupting the DNA repair pathways and inducing cyclobutane pyrimidine dimers (CPDs) through indirect sensitisation, these medications act as biological disruptors that weaken the genomic stability of keratinocytes. At INNERSTANDIN, we assert that the systemic impact of these agents necessitates a paradigm shift in how we monitor the intersection of pharmacology and environmental photobiology, acknowledging that the "hidden risk" is a tangible threat to long-term dermatological health.
The Cascade: From Exposure to Disease
The molecular pathogenesis of drug-induced photosensitivity begins not on the skin’s surface, but within the delicate electronic configuration of the exogenous chromophore. When a pharmacological agent—circulating systemically via the dermal vasculature—possesses a tricyclic or heterocyclic structure, it acts as a molecular antenna for ultraviolet radiation (UVR), specifically within the UVA waveband (320–400 nm). At INNERSTANDIN, we recognise that this is the initiation of a high-energy cascade that bypasses the body's natural photoprotective barriers. Upon the absorption of a photon, the medication molecule transitions from its stable ground state to an electronically excited singlet state, rapidly undergoing intersystem crossing to a longer-lived triplet state.
From this high-energy juncture, the cascade bifurcates into two distinct, yet often overlapping, pathological pathways: Type I and Type II photochemical reactions. In Type I reactions, the excited drug molecule undergoes direct electron or hydrogen transfer with biological substrates, such as keratinocyte membranes or cytoplasmic proteins, resulting in the formation of free radicals and subsequent lipid peroxidation. Type II reactions, however, are often more insidious; the triplet-state molecule transfers its energy directly to ground-state molecular oxygen ($^3O_2$), generating highly reactive singlet oxygen ($^1O_2$). This reactive oxygen species (ROS) is a potent oxidising agent that induces immediate lysosomal destabilisation and carbonylation of cellular proteins. Research published in *The Lancet* and the *British Journal of Dermatology* confirms that medications common in the UK, such as ciprofloxacin, naproxen, and hydrochlorothiazide, are particularly prone to these oxygen-dependent pathways.
The systemic ramifications of this cascade extend far beyond simple erythema. In phototoxic reactions, the massive release of pro-inflammatory cytokines—specifically IL-1, IL-6, and TNF-α—triggers a dose-dependent necrotic response that can mimic a severe chemical burn. Concurrently, if the drug or its photoproduct functions as a hapten, it may bind to endogenous proteins to form a complete photoantigen. This transition transforms a chemical reaction into an immunological crisis: the Type IV delayed-type hypersensitivity response. Here, Langerhans cells migrate to regional lymph nodes to prime CD8+ T-lymphocytes, leading to a systemic sensitisation where subsequent UV exposure, even at sub-erythemal doses, provokes a widespread eczematous eruption.
Ultimately, the INNERSTANDIN perspective reveals that the most clandestine risk lies in genotoxicity. Chronic photoactivation of medications like tetracyclines has been shown to induce cyclobutane pyrimidine dimers (CPDs) and oxidative DNA strand breaks. When the repair mechanisms, such as Nucleotide Excision Repair (NER), are overwhelmed by continuous drug-induced oxidative stress, the risk of keratinocyte carcinoma increases significantly. This is a critical concern in the UK, where the intermittent nature of UV exposure often leads to acute, high-intensity bouts of radiation that catch the medicated physiological system unprepared, cementing the link between common pharmacy prescriptions and long-term dermatological malignancy.
What the Mainstream Narrative Omits
The prevailing clinical discourse surrounding chemical photosensitivity frequently reduces the phenomenon to "sun allergy" or transient erythema, a simplification that obscures the profound molecular disruptions occurring within the dermal and systemic environments. At INNERSTANDIN, we assert that the mainstream narrative fails to address the sophisticated photobiological kinetics that transform ostensibly benign pharmacological agents into potent endogenous toxins. The reality involves a complex interplay of Type I and Type II photochemical reactions that extend far beyond the epidermis.
When a photosensitising medication—such as a fluoroquinolone antibiotic or a thiazide diuretic—absorbs ultraviolet radiation (UVR), it reaches an excited singlet state before undergoing intersystem crossing to a longer-lived triplet state. In Type I reactions, the drug molecule reacts directly with cellular substrates, transferring electrons or hydrogen atoms to generate free radicals (e.g., superoxide anions). Conversely, Type II reactions involve energy transfer to molecular oxygen, precipitating the formation of singlet oxygen ($^1O_2$). These Reactive Oxygen Species (ROS) initiate a cascade of lipid peroxidation and protein carbonylation, particularly targeting the lysosomal and mitochondrial membranes. Research indexed in *PubMed* highlights that this is not merely a localised reaction; the resultant systemic oxidative stress can lead to the "bystander effect," where non-irradiated tissues suffer damage due to circulating pro-inflammatory cytokines and secondary lipid hydroperoxides.
Furthermore, the mainstream overlooks the nuanced distinction between phototoxicity and photoallergy. While phototoxicity is a dose-dependent, non-immunological event, photoallergy represents a Type IV delayed hypersensitivity response where the drug acts as a pro-hapten. UV exposure induces a photochemical transformation of the drug into a reactive metabolite that covalently binds to skin proteins, creating a complete antigen. This process, as documented in *The Lancet*, triggers T-cell recruitment and systemic immunological memory, meaning subsequent minimal exposures can provoke widespread eczematoid eruptions.
Of even greater concern is the chronic "photo-mutagenic" potential that remains absent from patient leaflets. Prolonged use of photosensitisers like hydrochlorothiazide has been epidemiologically linked to a significantly elevated risk of squamous cell carcinoma (SCC) and lip cancer in the UK population. The mechanism involves the drug-induced inhibition of DNA repair enzymes and the promotion of 8-oxoguanine formation, a hallmark of oxidative DNA damage. By ignoring these sub-cellular trajectories, the current medical paradigm neglects the long-term oncogenic implications of chemical-light synergy, a critical oversight that INNERSTANDIN aims to rectify through rigorous biological deconstruction.
The UK Context
In the United Kingdom, the epidemiological landscape of chemical photosensitivity is increasingly complex, shaped by a convergence of high prescription rates and a general public misconception regarding UV intensity in temperate climates. While UVB levels (280–315 nm) fluctuate significantly with the seasons, the consistent prevalence of UVA (320–400 nm)—which penetrates cloud cover and standard window glass with high efficiency—presents a persistent threat to the millions of British citizens currently prescribed photosensitising medications. NHS prescribing data reveals a profound reliance on agents such as bendroflumethiazide, amiodarone, and tetracycline-class antibiotics. These compounds act as exogenous chromophores within the systemic circulation and dermal interstitial fluid, drastically lowering the threshold for cutaneous damage via specialised photochemical pathways.
At the sub-cellular level, INNERSTANDIN research underscores that these reactions are not merely "sunburn," but a profound biochemical betrayal. The mechanism typically involves the drug molecule absorbing UV energy and reaching an excited triplet state. This state facilitates Type I and Type II photochemical reactions, leading to the generation of reactive oxygen species (ROS) such as singlet oxygen, superoxide anions, and hydroxyl radicals. Peer-reviewed evidence in *The Lancet* and the *British Journal of Dermatology* identifies that these ROS induce rapid lipid peroxidation of cellular membranes and oxidative modifications to proteins and DNA. In the UK context, the chronic, low-level UV exposure characteristic of the British environment often results in "sub-clinical" phototoxicity. In these instances, cumulative DNA damage occurs without the immediate warning of severe erythema, potentially accelerating actinic keratosis and non-melanoma skin cancer (NMSC) phenotypes in the long term.
Furthermore, the UK’s National Institute for Health and Care Excellence (NICE) guidelines are only beginning to reflect the severity of drug-induced photosensitivity in polypharmacy patients. For the aging British population, the co-administration of NSAIDs like naproxen with cardiovascular medications creates a synergistic phototoxic risk profile that remains poorly quantified in clinical settings. This systemic impact requires a deeper innerstanding of the molecular kinetics at play; we must move beyond the simplistic "high-SPF" narrative and address the pharmacological reality that, for many in the UK, the internal chemical environment dictates the skin's biological response to the sky. Research indexed in PubMed consistently demonstrates that fluoroquinolones, for instance, can induce phototoxicity that persists long after the medication is metabolised due to the retention of metabolites in the dermal matrix—a factor often overlooked in standard UK primary care consultations. This necessitates a more rigorous, evidence-led approach to patient education regarding the invisible risks of the British light environment.
Protective Measures and Recovery Protocols
Mitigating the risks of drug-induced photosensitivity requires a sophisticated departure from generic photoprotection strategies, moving instead toward a precision-led biophysical intervention. At INNERSTANDIN, we identify that the primary failure in clinical management is the over-reliance on the Sun Protection Factor (SPF) metric, which predominantly measures UVB-induced erythema. However, the majority of drug-induced phototoxic and photoallergic reactions—particularly those triggered by fluoroquinolones, tetracyclines, and phenothiazines—are mediated by the UVA spectrum (320–400 nm). Because UVA penetrates deeper into the dermal layers where systemic medications circulate within the capillary beds, standard UVB-biased sunscreens offer a false sense of security.
Evidence-led protective measures must prioritise high-viscosity mineral barriers containing microfine zinc oxide or titanium dioxide, which provide a physical refractory shield against the long-wave UVA photons that initiate intersystem crossing in photosensitising chromophores. Furthermore, the optimisation of "circadian pharmacokinetics" is essential. For medications with shorter half-lives, such as certain non-steroidal anti-inflammatory drugs (NSAIDs), evening dosing can ensure that peak plasma concentrations ($C_{max}$) coincide with the absence of solar radiation, thereby allowing for significant metabolic clearance before the onset of the next diurnal UV peak. This approach, supported by research published in *The Lancet*, acknowledges that the severity of phototoxic damage is often a direct function of the drug’s concentration in the skin at the moment of photon absorption.
Recovery protocols must address the molecular carnage of reactive oxygen species (ROS) and the subsequent formation of cyclobutane pyrimidine dimers (CPDs). When a drug-sensitised cell undergoes photo-excitation, it often results in the depletion of intracellular glutathione and the activation of the pro-inflammatory NF-κB pathway. To counteract this, systemic administration of nicotinamide (Vitamin B3) has shown significant efficacy in enhancing the Nucleotide Excision Repair (NER) mechanisms, providing the necessary ATP to fuel the enzymatic excision of DNA photoproducts. Research within the UK context, notably from the *British Journal of Dermatology*, highlights that nicotinamide not only reduces the incidence of actinic keratoses but also serves as a metabolic substrate for cellular repair in photochemically stressed environments.
Post-exposure recovery should further involve the topical application of DNA repair enzymes (such as photolyases encapsulated in liposomes) and high-potency antioxidants like L-ascorbic acid and ferulic acid to quench the residual triplet states of excited molecules. Systemic recovery is incomplete without addressing the "cytokine storm" induced by keratinocyte apoptosis; therefore, the use of oral polyphenols and omega-3 fatty acids is recommended to downregulate the production of prostaglandin $E_2$ and interleukin-6. Through the INNERSTANDIN lens, recovery is not merely the alleviation of erythema, but the aggressive restoration of genomic stability and the re-establishment of the cutaneous basement membrane’s structural integrity.
Summary: Key Takeaways
Chemical photosensitivity represents a profound intersection of systemic pharmacology and cutaneous photobiology, where exogenous chromophores absorb ultraviolet radiation (UVR) to trigger deleterious photochemical cascades. At the sub-cellular level, the primary drivers are phototoxic reactions—dose-dependent phenomena characterised by the excitation of drug molecules into high-energy triplet states. These states facilitate the generation of reactive oxygen species (ROS), including singlet oxygen and superoxide radicals, which precipitate lipid peroxidation and lysosomal membrane rupture. Research published in *The Lancet* and *Nature Reviews Disease Primers* elucidates that these mechanisms extend beyond simple erythema; they involve profound DNA adduct formation and the activation of pro-inflammatory cytokines.
In the UK clinical context, the widespread prescription of fluoroquinolones, thiazide diuretics, and tetracyclines demands a more rigorous understanding of photoallergy—a delayed type IV hypersensitivity response where UVR-induced structural changes convert pro-haptens into complete antigens. INNERSTANDIN posits that the clandestine nature of sub-clinical phototoxicity constitutes a significant, often overlooked, driver of accelerated photoageing and genomic instability. The cumulative mutagenic burden, exacerbated by long-term medication use, correlates significantly with an increased incidence of non-melanoma skin cancers (NMSC), particularly squamous cell carcinoma. Ultimately, photosensitivity must be viewed as a systemic disruption of the dermal-redox balance, necessitating sophisticated photoprotection protocols that transcend basic SPF application to address the underlying molecular vulnerability of the medicated patient.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Chemical Photosensitivity: The Hidden Risks of Common Medications Under UV Exposure"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper