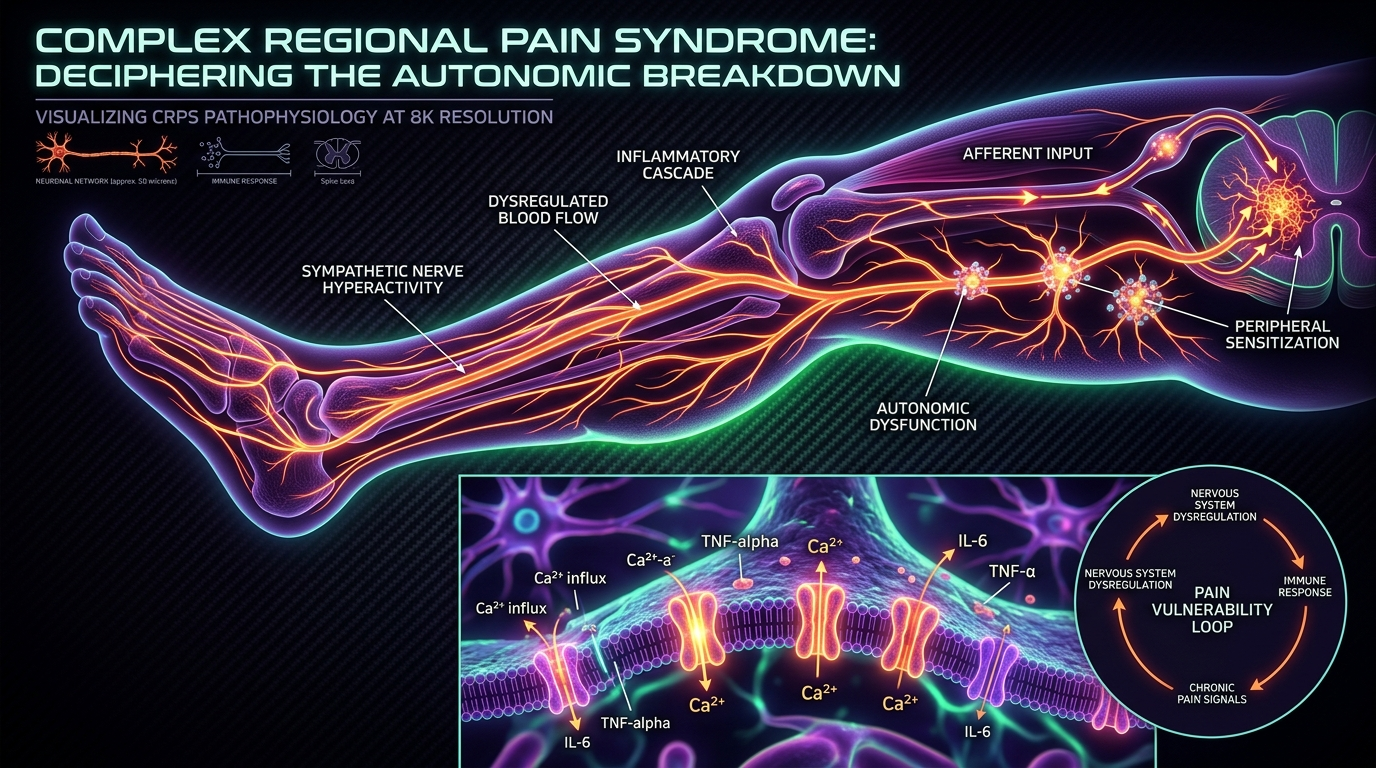
Complex Regional Pain Syndrome: Deciphering the Autonomic Breakdown
CRPS represents one of the most severe forms of chronic pain, characterized by a breakdown in autonomic control. New research suggests that auto-antibodies may be the primary driver of this often-misunderstood condition.
Overview
Complex Regional Pain Syndrome (CRPS) is not merely a condition; it is a profound physiological rebellion. To the uninitiated, it is often described as a "mystery illness," yet to those of us in the upper echelons of biological research, it represents the ultimate breakdown of the autonomic nervous system (ANS) and the catastrophic failure of the body’s self-regulatory mechanisms. It is a condition that defies the traditional "injury-healing" arc, transforming a minor insult—a sprain, a fracture, or a needle stick—into a lifelong prison of agonizing, burning pain.
Historically known as Reflex Sympathetic Dystrophy (RSD) or Causalgia, CRPS consistently ranks as the most painful condition known to medical science. On the McGill Pain Index, it scores higher than childbirth, the amputation of a digit, and terminal cancer pain. Yet, despite its objective severity, the mainstream medical establishment has spent decades relegating CRPS to the realm of "psychosomatic" disorders, or worse, treating it with a blunt-force trauma approach using opioids and invasive nerve blocks that often exacerbate the underlying pathology.
At INNERSTANDING, we look deeper. The emerging biological consensus—one that the mainstream narrative is slow to adopt—is that CRPS is a systemic autoimmune-autonomic crossover. It is a state where the body’s immune system, specifically a rogue army of auto-antibodies, hijacks the autonomic nervous system, locking the patient into a permanent "fight or flight" response at the cellular level. This is not just "pain"; it is a systemic breakdown of vascular control, inflammatory regulation, and neuro-immune communication.
According to data from the Royal College of Physicians, CRPS is estimated to affect approximately 15 in every 100,000 people in the UK annually, yet because of poor diagnostic training, many patients wait upwards of two years for a formal diagnosis, by which time the "wind-up" of the central nervous system is often irreversible.
This article serves as an exhaustive deconstruction of the CRPS mechanism. We will move beyond the superficial symptoms—the swelling, the skin discolouration, the temperature changes—and expose the cellular machinery that has gone haywire. We will explore the role of environmental triggers, the failure of the NHS to provide adequate root-cause care, and the burgeoning evidence that CRPS is, at its heart, a failure of the body to distinguish its own nervous system from an external threat.
##
The Biology — How It Works
To understand CRPS, one must first understand the Autonomic Nervous System (ANS). The ANS is the silent conductor of the body’s orchestra, managing everything from heart rate and digestion to the constriction of blood vessels and the response of the immune system. In a healthy organism, the ANS balances the sympathetic (stress) and parasympathetic (rest) branches with exquisite precision. In the CRPS patient, this balance is shattered.
The Sympathetic Malfunction
In CRPS, the sympathetic nervous system becomes "hyper-sensitised." Following an injury, the nerves that should signal for temporary inflammation and repair instead enter a state of permanent excitation. This leads to what we call Sympathetically Maintained Pain (SMP). The nerves begin to fire spontaneously, and the blood vessels in the affected limb lose their ability to regulate flow. This is why a CRPS limb may appear "angry"—deep red or purple, swollen, and radiating heat—or "ischaemic"—cold, blue, and mottled.
The biological horror of CRPS lies in the nociceptive feedback loop. Nociceptors (pain-sensing nerves) in the periphery send signals to the spinal cord. In a normal scenario, these signals diminish as the tissue heals. In CRPS, the "gates" in the dorsal horn of the spinal cord are flung wide open. This process, known as Central Sensitisation, means the brain begins to interpret even the lightest touch—the brush of a bedsheet or a cool breeze—as a searing, life-threatening burn. This phenomenon is termed allodynia.
The Neurogenic Inflammatory Soup
The second biological pillar of CRPS is neurogenic inflammation. Unlike standard inflammation caused by direct tissue damage, neurogenic inflammation is triggered by the nerves themselves. The peripheral nerves release "pro-inflammatory neuropeptides," specifically Substance P and Calcitonin Gene-Related Peptide (CGRP).
- —Substance P increases the permeability of blood vessels, leading to the characteristic "brawny" oedema (swelling) seen in CRPS.
- —CGRP causes powerful vasodilation, leading to the intense heat and redness.
This creates a self-perpetuating "inflammatory soup" that bathes the nerves, lowering their firing threshold even further. The body becomes trapped in a cycle where the pain causes inflammation, and the inflammation causes more pain.
The Role of the Somatosensory Cortex
The breakdown is not limited to the limb. As the chronic signals bombard the brain, the somatosensory cortex—the area of the brain responsible for mapping the body—begins to "blur." In CRPS patients, the cortical representation of the affected limb shrinks or becomes distorted. This is why many patients report a sense of "alienation" from their limb, sometimes even feeling as though it does not belong to them or is larger/smaller than its physical dimensions. This "cortical remapping" is a biological testament to the fact that CRPS is a whole-body neurological catastrophe.
##
Mechanisms at the Cellular Level
When we descend to the cellular level, the true culprit of CRPS emerges: the glial cell and the auto-antibody. For decades, glia were thought to be mere "glue" holding neurons together. We now know they are the primary immune cells of the central nervous system, and in CRPS, they are the "engines of chronic pain."
Glial Activation and the Cytokine Storm
In the spinal cord of a CRPS patient, glial cells (microglia and astrocytes) become "primed" and "activated." Once activated, they release a torrent of pro-inflammatory cytokines, such as Tumour Necrosis Factor-alpha (TNF-$\alpha$) and Interleukin-1 beta (IL-1$\beta$).
These cytokines are neurotoxic in high concentrations. They heighten the sensitivity of the surrounding neurons, creating a state of "pathological excitation." This glial activation is the reason why CRPS can "spread" from one limb to another. Since the glia in the spinal cord are interconnected, the inflammatory signals can travel up and down the spinal column, igniting pain in previously healthy areas of the body. This is not a "psychological" spread; it is a cellular contagion.
The Auto-antibody Smoking Gun
The most revolutionary development in CRPS research is the discovery of auto-antibodies against G-protein coupled receptors (GPCRs). Research, notably by Goebel and colleagues, has identified that a significant percentage of CRPS patients possess IgG auto-antibodies that specifically target:
- —$\beta$2-Adrenergic Receptors
- —$\alpha$1-Adrenergic Receptors
- —Muscarinic M2 Receptors
These receptors are the "steering wheel" of the autonomic nervous system. When auto-antibodies bind to these receptors, they can either over-stimulate or block them, leading to the profound vascular instability and sweating abnormalities seen in the clinical setting.
Experimental studies have shown that when IgG antibodies from CRPS patients are injected into mice, the mice develop the same sensory hypersensitivity and swelling characteristic of the human disease. This confirms that CRPS is, at its core, an autoimmune-driven autonomic assault.
Mitochondrial Dysfunction and Oxidative Stress
Finally, at the mitochondrial level, CRPS represents a failure of energy production. The chronic ischaemia (lack of oxygen) caused by dysfunctional blood vessels leads to the accumulation of Reactive Oxygen Species (ROS). These free radicals damage the delicate machinery of the mitochondria in the peripheral nerves. Without adequate ATP (energy), the nerves cannot maintain their "resting potential" and begin to fire uncontrollably. This creates a state of metabolic crisis within the affected tissue, leading to the muscle wasting (atrophy) and bone density loss (Sudeck’s atrophy) often seen in Stage III CRPS.
##
Environmental Threats and Biological Disruptors
In our modern industrialised world, the human organism is under constant assault. For a "normal" person, these stressors may cause fatigue or minor illness. For the individual predisposed to CRPS, they act as the "second hit" that prevents the nervous system from ever recalibrating.
The Impact of Stealth Infections
Many CRPS cases are preceded by a period of immune "priming." Stealth infections—such as Epstein-Barr Virus (EBV), Lyme Disease (Borrelia), or Mycoplasma—can leave the immune system in a state of hyper-vigilance. When a physical injury occurs, the immune system, already on a "war footing," overreacts. This molecular mimicry, where the body’s response to a virus begins to target its own nerve receptors, is a primary driver of the autoimmune cascade in CRPS.
Heavy Metals and Neurotoxicity
The presence of neurotoxic heavy metals—specifically mercury, aluminium, and lead—acts as a catalyst for glial activation. These metals accumulate in the central nervous system and act as "hitchhikers" on the pathways meant for essential minerals. Once lodged in the brain or spinal cord, they induce chronic oxidative stress, making the "wind-up" of the nervous system significantly more difficult to reverse. In the UK, historical exposure to lead piping and industrial pollutants remains a silent factor in the severity of chronic pain cases.
Electromagnetic Fields (EMFs) and Calcium Channel Signaling
The emerging field of bio-electromagnetics suggests that constant exposure to high-frequency EMFs (from 5G infrastructure, Wi-Fi, and smart devices) may interfere with Voltage-Gated Calcium Channels (VGCCs) in our cells. Since CRPS is essentially a disorder of "electrical" signaling in the nerves, the presence of external fields that force calcium into the cells can exacerbate the "hyperexcitability" of the nociceptors. While mainstream science remains hesitant to link EMFs to CRPS, the biological mechanism—calcium influx leading to nitric oxide elevation and peroxynitrite damage—is well-documented in biophysics.
The Gut-Brain-Nerve Axis
Modern dietary disruptors, particularly glyphosate and processed seed oils, damage the intestinal lining, leading to "Leaky Gut" (intestinal permeability). This allows lipopolysaccharides (LPS) from gut bacteria to enter the bloodstream. LPS is a potent activator of the immune system and has been shown to cross the blood-brain barrier, further priming the glia for the CRPS cascade. A compromised microbiome is almost always found in the background of chronic, non-healing pain patients.
##
The Cascade: From Exposure to Disease
The progression of CRPS is often described in three stages, but this is a simplification of a complex, overlapping biological cascade.
Phase 1: The Initial Insult and the Failure of Resolution
It begins with a trauma. This trauma does not have to be severe; a simple ankle sprain or a minor surgical procedure like a carpal tunnel release can suffice. Under normal conditions, the body initiates the Pro-Resolution Phase of inflammation, involving specialised pro-resolving mediators (SPMs) that "switch off" the pain. In the CRPS-prone individual, this "off switch" is broken. Instead of resolution, the body enters a state of sustained sympathetic discharge.
Phase 2: The "Wind-up" and the Peripheral-Central Shift
Within weeks, the pain begins to spread beyond the territory of the original nerve injury. This is the Peripheral-to-Central shift. The spinal cord becomes "remodeled." The constant barrage of pain signals causes the NMDA receptors in the spinal cord to become permanently activated. This is the "wind-up" phenomenon, where the volume of the pain is turned to 11 and the dial is snapped off.
At this stage, the Autonomic Breakdown becomes visible. The limb may sweat excessively (hyperhidrosis) or stop sweating entirely. Hair and nail growth may accelerate or cease. The body’s "thermostat" for that limb is now controlled by a broken computer.
Phase 3: The Atrophic Lockdown
If the cascade is not interrupted, the condition enters the atrophic stage. The constant lack of proper blood flow and the toxic "inflammatory soup" lead to the death of local tissues. Muscles wither, joints become stiff and "frozen" (ankylosis), and the skin becomes thin, shiny, and brittle. The nervous system has now essentially "divorced" the limb. The pain remains, but the tissue is dying.
It is at this stage that many UK patients are told there is "nothing more that can be done," a statement that ignores the plastic nature of the nervous system and the potential for recovery through intensive, multi-modal intervention.
##
What the Mainstream Narrative Omits
The current medical model for CRPS is fundamentally flawed because it is based on symptom suppression rather than systemic restoration. The mainstream narrative, dictated largely by pharmaceutical interests and legacy medical training, omits several critical truths.
The Failure of the "Psychosomatic" Label
For decades, and still today in many UK hospitals, CRPS patients are told their pain is a manifestation of anxiety, depression, or "secondary gain" (seeking attention or compensation). This is a convenient fiction that allows the medical system to ignore its own failure to treat the condition. While chronic pain certainly *causes* depression and anxiety, these are downstream effects, not the cause. To label a patient with objectively measurable skin temperature changes and bone loss as "psychosomatic" is a form of medical gaslighting that delays life-saving treatment.
The Danger of Opioids
The mainstream response to CRPS often involves heavy doses of opioids (Oxycontin, Fentanyl, Morphine). However, the biological reality is that opioids can cause Opioid-Induced Hyperalgesia (OIH). In CRPS, where the glia are already hyper-active, opioids can actually *activate* the Toll-Like Receptor 4 (TLR4) on glial cells, making the pain worse over time. The "standard of care" is, in many cases, fuel on the fire.
The Suppression of the Auto-antibody Evidence
Despite the compelling evidence that CRPS is an autoimmune condition, there is a distinct lack of funding for clinical trials involving Intravenous Immunoglobulin (IVIG) or Plasmapheresis (plasma exchange) for CRPS. Why? Because these treatments are expensive and cannot be easily patented by Big Pharma. It is far more profitable to keep a patient on a lifetime of Gabapentin and antidepressants than to clear their blood of the auto-antibodies that are driving the disease.
The Iatrogenic Factor
Many cases of CRPS are iatrogenic—caused by medical intervention. Poorly managed post-operative pain or the accidental nicking of a nerve during a routine procedure are common triggers. The medical establishment is hesitant to highlight the true incidence of CRPS following elective surgeries, as it would necessitate a radical change in surgical protocols and informed consent.
##
The UK Context
In the United Kingdom, the CRPS landscape is particularly challenging. The National Health Service (NHS), while designed for acute care, is woefully unequipped to handle the complexity of a multi-system autonomic breakdown.
The NHS "Postcode Lottery"
The quality of care for a CRPS patient in the UK depends entirely on their proximity to one of the few specialised "Pain Management Programmes" (PMPs), such as those in Bath or London. In many regions, the only treatment available is a referral to a generalist physiotherapist who may inadvertently cause more damage by pushing the patient through "Aggressive Physical Therapy," which can trigger a massive flare in a sensitised nervous system.
The Economic Burden
A 2018 study estimated that the cost of chronic pain to the UK economy is over £10 billion per year in lost productivity and healthcare costs. CRPS represents a disproportionate slice of this, as it often strikes people in their prime working years (ages 30-50).
The UK’s Department for Work and Pensions (DWP) often fails to recognise CRPS as a fluctuating disability. Because the "invisible" nature of the pain does not always manifest in obvious physical deformity in the early stages, many UK sufferers are forced into harrowing "Work Capability Assessments," which exacerbate the stress-response and, consequently, the pain itself.
The Lack of Preventative Protocols
In some European countries, high-dose Vitamin C is standard protocol following a wrist fracture to prevent the development of CRPS. In the UK, this simple, low-cost intervention is rarely implemented in A&E departments. The British medical system remains reactive rather than proactive, waiting for the "breakdown" to occur rather than fortifying the organism against it.
##
Protective Measures and Recovery Protocols
Recovery from CRPS is possible, but it requires a "scorched earth" approach to the underlying biology. We must calm the glia, clear the auto-antibodies, and retrain the brain.
1. Calming the Glial Engines
The first priority is to stop the cytokine storm in the central nervous system.
- —Low Dose Naltrexone (LDN): In micro-doses (1.5mg to 4.5mg), Naltrexone acts as a glial cell stabiliser by blocking the TLR4 receptors. This is one of the most effective, yet underutilised, tools in the CRPS arsenal.
- —Palmitoylethanolamide (PEA): A fatty acid amide that has been clinically shown to reduce mast cell and glial activation. It is a natural "body-own" substance that helps restore homeostasis.
2. Addressing the Auto-antibodies
If the case is severe and autoimmune-driven, systemic intervention is required.
- —IVIG and Plasmapheresis: These treatments aim to dilute or remove the rogue IgG antibodies. While difficult to access in the UK, they can be transformative for those in the early to mid-stages of the disease.
- —Anti-Inflammatory Nutrition: A strict elimination diet—removing gluten, dairy, seed oils, and refined sugars—is non-negotiable. Many CRPS patients find relief on a Ketogenic or Carnivore diet, which provides the brain with stable energy and reduces the systemic "burn."
3. Neurological Retraining
The brain’s map must be redrawn.
- —Graded Motor Imagery (GMI): This involves three stages: Left/Right discrimination, Explicit Motor Imagery, and Mirror Box Therapy. This "sneaks" past the brain’s pain guard, allowing the motor cortex to engage without triggering the nociceptive alarm.
- —Vagus Nerve Stimulation: Techniques to increase "vagal tone" can help shift the body from a sympathetic state to a parasympathetic state. This can include deep diaphragmatic breathing, cold water immersion (carefully applied), and specific biofeedback devices.
4. Environmental Detoxification
The patient must reduce their "total toxic load."
- —EMF Mitigation: Turning off Wi-Fi at night and reducing exposure to mobile devices can help lower the electrical "noise" the nervous system has to process.
- —Chelation and Gut Repair: Addressing heavy metal toxicity and healing the gut lining are essential for long-term immune stability.
5. Pharmaceutical Alternatives
Moving away from opioids and towards "nerve-quieting" agents that don't cause hyperalgesia.
- —Ketamine Infusions: When administered correctly, Ketamine can "reset" the NMDA receptors in the spinal cord, essentially rebooting the system. This is becoming more available in the UK through private clinics, though it remains difficult to access on the NHS.
##
Summary: Key Takeaways
CRPS is a window into the fragility and the complexity of the human biological system. It is the point where the nervous system and the immune system become indistinguishable, locked in a cycle of mutual destruction.
- —CRPS is an Autoimmune Disorder: The discovery of auto-antibodies against adrenergic receptors proves that the "pain" is a symptom of a systemic immune hijack.
- —The Autonomic Breakdown is Real: The temperature changes, swelling, and skin issues are not "in the mind"; they are the physical manifestation of a broken autonomic conductor.
- —The Mainstream Model is Failing: Relying on opioids and psychological dismissal is a biological dead end.
- —The UK System Requires Reform: From preventative Vitamin C to better access to IVIG and LDN, the NHS must evolve to treat CRPS as a multi-system failure.
- —Recovery is a Multi-Modal Journey: There is no "magic bullet." Healing requires glial stabilisation, immune modulation, neurological retraining, and environmental detoxification.
As we move forward in our understanding of pain science, CRPS will no longer be seen as a "mystery." It will be seen as the ultimate test of our ability to restore order to a biological system in chaos. For the researcher, it is a challenge to be solved; for the patient, it is a battle for the very sovereignty of their body. At INNERSTANDING, we remain committed to exposing the truths that the standard narrative ignores, providing the roadmap for those seeking to escape the prison of autonomic breakdown.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Complex Regional Pain Syndrome: Deciphering the Autonomic Breakdown"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Chronic Pain & Pain Science — products curated by our research team for educational relevance and biological support.

Magnesium L-Threonate

Magnesium Blend – The Most Important Mineral

Energy Blend Supports
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper