Cytokine Storms and Joint Decay: The Molecular Drivers of Osteoarthritis
Osteoarthritis is increasingly understood as an inflammatory metabolic disease rather than simple wear and tear. Suppressed research highlights how pro-inflammatory cytokines drive cartilage degradation in the absence of mechanical injury.
Overview
For decades, the clinical understanding of Osteoarthritis (OA) has been shackled to a primitive mechanical paradigm. It has been described to patients as the inevitable "wear and tear" of an ageing machine—a simple thinning of the "brake pads" of the human body. This reductionist view suggests that if you live long enough, your joints will simply expire through friction and gravity. However, recent biological research, much of it overshadowed by the lucrative industry of prosthetic joint replacement, reveals a far more sinister and complex reality. Osteoarthritis is not a mechanical failure; it is a chronic inflammatory metabolic disease.
We are witnessing a silent epidemic where the joint is no longer a passive victim of movement, but a site of active molecular sabotage. At the heart of this decay is a phenomenon known as a Cytokine Storm—a localized, low-grade, yet relentless immunological assault that systematically dissolves cartilage from the inside out. This article explores the transition from the "wear and tear" myth to the "inflammatory-metabolic" reality, exposing how modern environmental triggers and systemic biological disruptors are turning our own immune systems against our skeletal integrity.
Under the microscope, the OA joint is a battlefield. The chondrocytes—the only cells found in healthy cartilage—which should be maintaining the structural matrix, instead undergo a phenotypic shift. They become "pro-inflammatory secretory cells," pumping out degradative enzymes and signalling molecules that recruit the systemic immune system to join the destruction. When we talk about OA today, we are talking about a failure of cellular signalling and a breakdown in metabolic homeostasis. It is a disease of the modern age, driven by systemic inflammation that finds its most vulnerable expression in the synovial fluid of our weight-bearing joints.
##
The Biology — How It Works
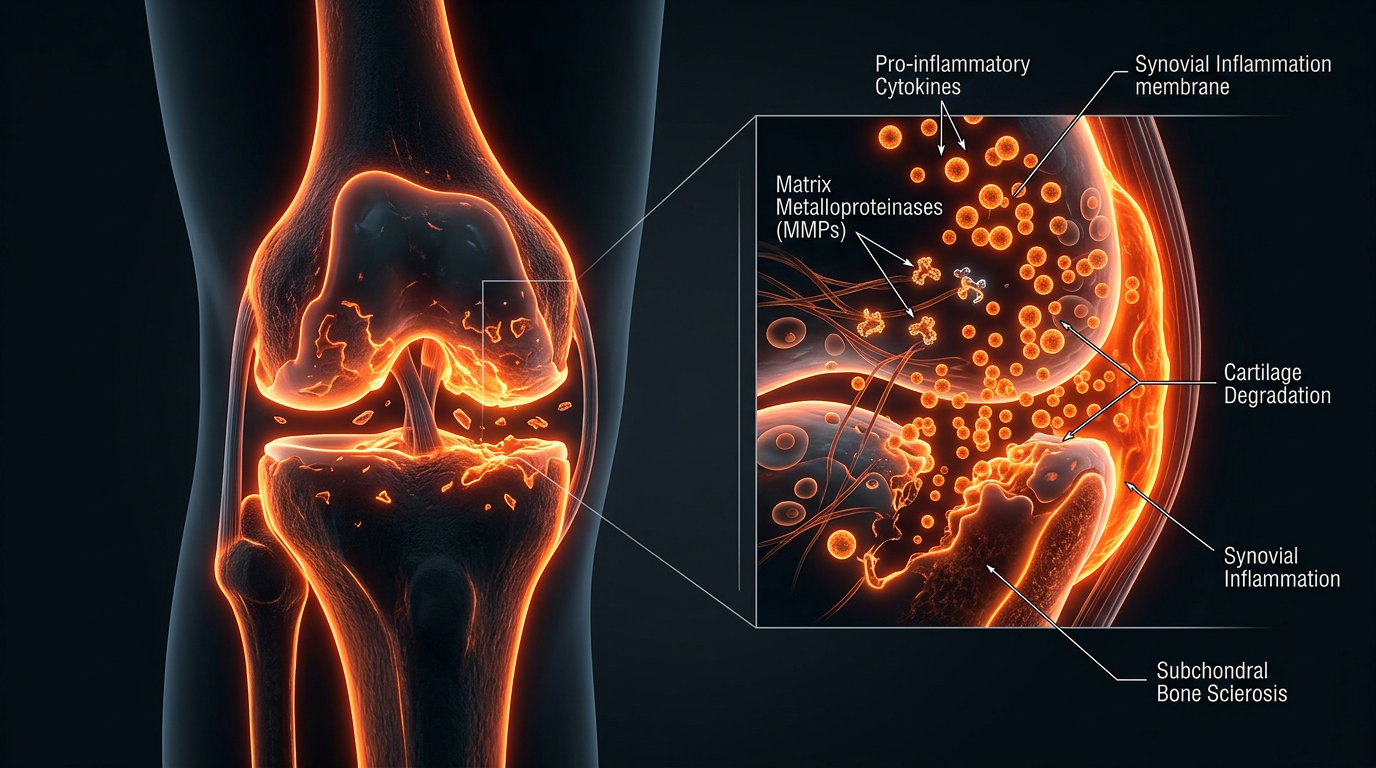
To understand the cytokine storm within a joint, one must first understand the "Joint Organ." A joint is not merely two bones touching; it is a sophisticated ecosystem comprising the articular cartilage, the subchondral bone, the synovium (the lining), the ligaments, and the synovial fluid. In a healthy state, this ecosystem exists in a delicate balance of anabolism (building up) and catabolism (breaking down).
The Chondrocyte: The Architect Turned Arsonist
The chondrocyte is the master regulator of cartilage. Under normal physiological conditions, these cells produce Type II collagen and proteoglycans, which give cartilage its shock-absorbing, frictionless properties. However, in the presence of systemic metabolic stress or chronic low-grade inflammation, these cells "switch." They stop producing the structural matrix and begin secreting Matrix Metalloproteinases (MMPs) and Aggrecanases (ADAMTS).
These enzymes are biological acids; they do not wait for "wear" to occur; they actively digest the cartilage fibres. This process is driven by the primary drivers of the cytokine storm: Interleukin-1 Beta (IL-1β) and Tumour Necrosis Factor-alpha (TNF-α). These cytokines bind to the surface of chondrocytes, triggering a genetic cascade that overrides the cell’s repair mechanisms.
The Synovial Fluid: A Toxic Reservoir
The synovial fluid, which should act as a high-performance lubricant (rich in hyaluronic acid), becomes a medium for inflammatory transport. In an osteoarthritic joint, the fluid is saturated with pro-inflammatory cytokines, chemokines, and "Damage-Associated Molecular Patterns" (DAMPs). These are essentially cellular "alarm bells" that keep the immune system in a state of high alert. As the cartilage begins to fray—not from movement, but from enzymatic digestion—the microscopic fragments are released into the synovial fluid. The synovial membrane detects these fragments as foreign invaders, triggering a secondary wave of inflammation (synovitis), which further increases the production of cytokines. It is a closed-loop system of self-destruction.
UK FACT: According to Arthritis Action, over 10 million people in the UK have osteoarthritis. It is the leading cause of disability, yet current NHS protocols still focus almost exclusively on late-stage pain management rather than early-stage metabolic intervention.
##
Mechanisms at the Cellular Level
The "storm" occurs when the regulatory checkpoints of the cell are bypassed. At the molecular level, the primary culprit is the NF-κB (Nuclear Factor kappa-light-chain-enhancer of activated B cells) signalling pathway. This is the master "on switch" for inflammation.
The NF-κB Pathway and Molecular Sabotage
When IL-1β or TNF-α binds to a chondrocyte, it activates the NF-κB complex. Once activated, this protein moves into the cell nucleus and "unlocks" the genes responsible for destruction. Specifically, it leads to:
- —Upregulation of MMP-1, MMP-3, and MMP-13: These are the primary enzymes that break down the collagen scaffold of the joint. MMP-13, in particular, is a "collagenase" of terrifying efficiency, capable of cleaving the triple helix of Type II collagen, which is otherwise one of the most stable structures in the human body.
- —Nitric Oxide (NO) Production: High levels of NO in the joint induce chondrocyte apoptosis (programmed cell death). As the population of chondrocytes thins, the cartilage loses its ability to repair itself entirely.
- —Prostaglandin E2 (PGE2) Synthesis: This molecule is responsible for the intense pain and sensitisation of the local nerves, leading to the chronic "ache" associated with OA.
The Role of the Infrapatellar Fat Pad (IPFP)
Recent research has highlighted a "hidden" driver of joint decay: the fat pads located within the joint capsule. Long thought to be simple cushions, the IPFP is now recognized as a highly active endocrine organ. In individuals with metabolic syndrome or high systemic inflammation, this fat pad secretes adipokines like leptin and adiponectin directly into the joint space. These adipokines act as "fuel" for the cytokine storm, amplifying the inflammatory signals and accelerating the rate of cartilage loss. This explains why obese individuals often suffer from OA in non-weight-bearing joints, like the hands; the cause is biochemical, not mechanical.
##
Environmental Threats and Biological Disruptors
If OA is a metabolic disease, we must ask: what is disrupting our metabolism? The modern environment is saturated with "Joint-Disrupting Chemicals" and dietary triggers that prime the body for a cytokine storm.
The Omega-6/Omega-3 Imbalance
The British diet has shifted dramatically over the last 50 years. The over-consumption of ultra-processed seed oils (rich in Linoleic Acid) has skewed our cellular membranes towards a pro-inflammatory state. These Omega-6 fatty acids are the direct precursors to arachidonic acid, which the body uses to manufacture the very inflammatory cytokines (IL-6, TNF-α) that drive joint decay. When the ratio of Omega-6 to Omega-3 exceeds 15:1 (the UK average), the body is biologically "locked" into an inflammatory posture.
Endocrine Disruptors and "Obesogens"
We are constantly exposed to phthalates, bisphenols (BPA/BPS), and PFAS ("forever chemicals") through plastics and water supplies. These chemicals interfere with hormone signalling, particularly oestrogen receptors, which play a crucial role in maintaining cartilage health. This is why we see a significant spike in OA cases among post-menopausal women; the loss of protective oestrogen, combined with an onslaught of endocrine-disrupting chemicals, leaves the joints defenceless against the cytokine storm.
Hyperinsulinaemia and Glycation
Chronic elevation of blood sugar leads to the formation of Advanced Glycation End-products (AGEs). These are "sticky" sugar-protein complexes that cross-link with the collagen in our joints, making the cartilage brittle and prone to micro-cracks. Furthermore, high insulin levels directly stimulate the production of IL-6, one of the most potent drivers of systemic inflammation. In essence, a high-sugar diet "caramelises" the joints, making them structurally weak and chemically inflamed.
ALARMING STAT: Research indicates that patients with Type 2 Diabetes are twice as likely to develop Osteoarthritis, regardless of their weight, proving that metabolic dysfunction is a primary driver of joint degradation.
##
The Cascade: From Exposure to Disease
The progression of OA follows a predictable, yet often ignored, molecular cascade. It begins long before an X-ray can detect "bone on bone" contact.
- —The Trigger Phase: This is often a combination of systemic metabolic stress (diet/toxins) and perhaps a minor "micro-insult" (a small twist or repetitive movement). In a healthy body, this would be repaired. In a metabolically compromised body, it triggers the recruitment of macrophages (immune cells) to the synovium.
- —The Amplification Phase: The macrophages release IL-1β and TNF-α. These cytokines enter the cartilage and "flip the switch" on the chondrocytes. The chondrocytes stop building and start destroying.
- —The Feedback Loop: As the cartilage breaks down, "DAMPs" (Damage-Associated Molecular Patterns) are released. These DAMPs bind to Toll-Like Receptors (TLR4) on the synovial cells, which signals the body that there is a "major infection" or injury. The body responds by sending *more* cytokines. The storm is now self-sustaining.
- —The Structural Collapse: Eventually, the cartilage is thinned to the point where the subchondral bone is exposed. The bone, sensing the increased pressure, begins to thicken and grow "osteophytes" (bone spurs) in a desperate attempt to stabilise the joint. This is the stage where the mainstream medical system finally intervenes, usually with surgery.
##
What the Mainstream Narrative Omits
The current medical hegemony regarding OA is one of managed decline. The standard of care—paracetamol, NSAIDs (like Ibuprofen), and eventually joint replacement—is a "end-of-pipe" solution that ignores the biological fire raging upstream.
The NSAID Trap
While Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) reduce pain by inhibiting the COX-2 enzyme, they also inhibit the synthesis of proteoglycans—the very building blocks of cartilage. Long-term use of NSAIDs has been shown in some studies to *accelerate* the progression of OA because they interfere with the natural (albeit stifled) repair mechanisms of the chondrocyte. Furthermore, they damage the gut lining, leading to "leaky gut," which allows bacterial endotoxins (LPS) into the bloodstream, which then travel to the joints and *worsen* the cytokine storm.
The Suppression of Regenerative Biology
There is a profound lack of funding for research into nutritional and biological interventions that could potentially reverse the chondrocyte's phenotypic switch. Why? Because you cannot patent a change in the Omega-6/Omega-3 ratio, and you cannot patent the avoidance of ultra-processed foods. The "Wear and Tear" narrative is highly profitable; it creates a pipeline of patients for the multi-billion pound orthopaedic surgery industry. If OA were recognized as a reversible metabolic condition, the entire infrastructure of joint care would have to be dismantled.
The "Silent" Cartilage
One of the most dangerous omissions is the fact that cartilage has no nerves. You cannot "feel" your cartilage dissolving. By the time you feel pain, the inflammation has already spread to the bone and the synovium. This means that millions of people are currently in the midst of a cytokine storm without knowing it. The "wear and tear" myth encourages people to wait until they are in pain to seek help, at which point the molecular cascade is often too far advanced for simple interventions.
##
The UK Context
The United Kingdom is facing a unique crisis in joint health. Our high rates of metabolic syndrome, combined with a sedentary lifestyle and a diet dominated by supermarket convenience foods, have created a "perfect storm" for OA.
UK STAT: The economic burden of musculoskeletal conditions in the UK is estimated at over £10 billion per year in direct costs to the NHS and lost productivity.
The NHS's "wait and see" approach is particularly damaging. Patients are often told to lose weight and take paracetamol until the joint is sufficiently destroyed to justify the cost of surgery. However, the "lose weight" advice is rarely accompanied by the metabolic education needed to lower the cytokine load. Simply eating "less" of a pro-inflammatory diet will not stop the enzymatic digestion of the joint. We need a radical shift towards Immunometabolic Orthopaedics.
Furthermore, the British "stiff upper lip" culture often means that early symptoms of systemic inflammation—such as morning stiffness, brain fog, and fatigue—are ignored. These are the early warning signs of the cytokine storm. In the UK, we are treating the symptoms of an ageing population while ignoring the fact that our biological "ageing" is being accelerated by our environment.
##
Protective Measures and Recovery Protocols
To stop the cytokine storm, we must address the "Joint Organ" from a multi-directional biological perspective. We must deactivate the NF-κB switch and provide the body with the raw materials for repair.
1. Metabolic Correction: The First Line of Defence
The single most effective way to dampen a cytokine storm is to alter the fatty acid composition of the cell membranes.
- —Aggressive Omega-3 Supplementation: High-dose, high-quality EPA and DHA (fish or algae oil) compete with pro-inflammatory Omega-6 fats, directly reducing the production of IL-1β and TNF-α.
- —Elimination of Seed Oils: Removing industrial vegetable oils (soybean, corn, rapeseed/canola) from the diet removes the primary fuel source for the inflammatory cascade.
- —Gluten and Lectin Reduction: For many, these proteins can trigger "leaky gut," leading to the systemic translocation of endotoxins that aggravate joint inflammation.
2. Targeted Nutracuticals
Certain compounds have shown the ability to interfere with the molecular pathways of OA:
- —Curcumin (with Piperine): A potent inhibitor of the NF-κB pathway. It acts similarly to some pharmaceutical anti-inflammatories but without the degradative effect on cartilage synthesis.
- —Glucosamine and Chondroitin (Sulphate forms): While controversial in mainstream meta-analyses, when used in high-purity sulphate forms, they provide the "bricks and mortar" for the extracellular matrix and have a mild signalling effect that encourages chondrocyte anabolism.
- —Sulforaphane: Found in broccoli sprouts, this compound has been shown to block the enzymes (MMPs) that destroy joints.
3. Mechanotherapy: "Motion is Lotion"
While excessive impact on an inflamed joint is bad, absolute rest is worse. Cartilage is avascular—it has no blood supply. It relies on the "synovial pump" (movement) to drive nutrients in and waste products out.
- —Low-Impact Resistance Training: Controlled loading of the joint signals the chondrocytes to produce more Type II collagen. It also strengthens the surrounding musculature, reducing the mechanical "slap" on the joint surfaces.
- —Photobiomodulation (Red Light Therapy): Specific wavelengths of light can penetrate the joint and stimulate the mitochondria within chondrocytes, increasing cellular energy (ATP) and aiding in the repair process.
4. Circadian Rhythm and Sleep
The repair of cartilage happens almost exclusively during deep sleep. Chronic sleep deprivation increases systemic IL-6 levels. Aligning the body's circadian rhythm and ensuring deep, restorative sleep is a non-negotiable component of joint recovery.
##
Summary: Key Takeaways
Osteoarthritis is far more than a mechanical failure; it is a molecular war. The "Wear and Tear" narrative is a dangerous oversimplification that has led to a global epidemic of unnecessary disability and surgery.
- —The Real Culprit: Localised "Cytokine Storms" (driven by IL-1β, TNF-α, and IL-6) are the primary drivers of cartilage destruction, not simple movement.
- —Molecular Sabotage: The chondrocyte—the joint's architect—is hijacked by inflammatory signals, turning it into a source of degradative enzymes (MMPs) that digest the cartilage from within.
- —Metabolic Roots: OA is intimately linked to metabolic health. High insulin, skewed Omega fatty acid ratios, and environmental toxins prime the joints for decay.
- —The Mainstream Failure: Current UK medical protocols focus on late-stage symptoms and surgical intervention, ignoring the upstream biochemical causes that could be managed or reversed.
- —The Path Forward: Recovery requires an aggressive "Immunometabolic" approach: dampening the NF-κB switch through diet, correcting fatty acid imbalances, and using targeted movement to flush the synovial system.
We must stop viewing our joints as inanimate hinges and start seeing them as living, breathing biological systems that respond to the chemical environment we create. The power to halt joint decay lies not in the surgeon’s scalpel, but in the molecular mastery of our own biology. It is time to move beyond the "wear and tear" myth and address the cytokine storm at its source. Only then can we hope to reclaim our mobility and our health from this insidious disease.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Cytokine Storms and Joint Decay: The Molecular Drivers of Osteoarthritis"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper