Giardiasis in the UK: Identifying the Hidden Waterborne Threat to Digestive Health
A comprehensive review of Giardia lamblia, a resilient waterborne parasite common in the UK. This article explains its survival mechanisms, how it causes malabsorption, and the risks associated with wild swimming.

# Giardiasis in the UK: Identifying the Hidden Waterborne Threat to Digestive Health
Overview
In the verdant landscapes of the United Kingdom, from the rugged peaks of the Lake District to the winding currents of the River Wye, a silent, microscopic predator is proliferating. While the British public has embraced "wild swimming" and outdoor pursuits with newfound vigour, a biological hazard remains largely ignored by mainstream health narratives: Giardia lamblia (also known as *Giardia intestinalis* or *Giardia duodenalis*). This flagellated protozoan parasite is not merely a "traveller’s bug" picked up in distant tropical locales; it is a resilient, endemic threat residing in our local waterways, our livestock, and increasingly, our domestic water systems.
Giardiasis is the clinical infection caused by this parasite, and it represents one of the most significant yet under-reported causes of non-bacterial diarrhoea and long-term digestive dysfunction in the UK. At INNERSTANDING, we believe in exposing the biological realities that the National Health Service (NHS) and the Environment Agency often downplay. The reality is that our ageing sewage infrastructure, combined with agricultural runoff, has created a "perfect storm" for *Giardia* to thrive.
The complexity of *Giardia* lies in its sheer resilience. It exists in a dual-stage life cycle that allows it to survive the harshest environmental stressors, including the standard chlorine levels used in municipal water treatment. For the individual, an encounter with this parasite marks the beginning of a profound physiological disruption—a cascade of malabsorption, immune exhaustion, and a fundamental restructuring of the gut microbiome that can persist for years if left unaddressed. This article will deconstruct the biological machinery of *Giardia*, the failure of our current environmental protections, and the path to reclaiming digestive sovereignty.
Fact: *Giardia* is one of the most common intestinal parasites worldwide, yet in the UK, it is estimated that for every one laboratory-confirmed case, dozens go undiagnosed due to the intermittent nature of parasite shedding and the limitations of standard stool microscopy.
##
##
The Biology — How It Works
To understand why *Giardia lamblia* is such a formidable opponent, one must first understand its morphology and life cycle. Unlike many bacteria that rely on rapid binary fission and metabolic versatility, *Giardia* is an elegantly designed specialist. It is a protozoan—a single-celled eukaryote—that has evolved specifically to inhabit the anaerobic environment of the mammalian small intestine.
The Two-Stage Life Cycle
The survival of *Giardia* is predicated on its ability to transition between two distinct forms: the cyst and the trophozoite.
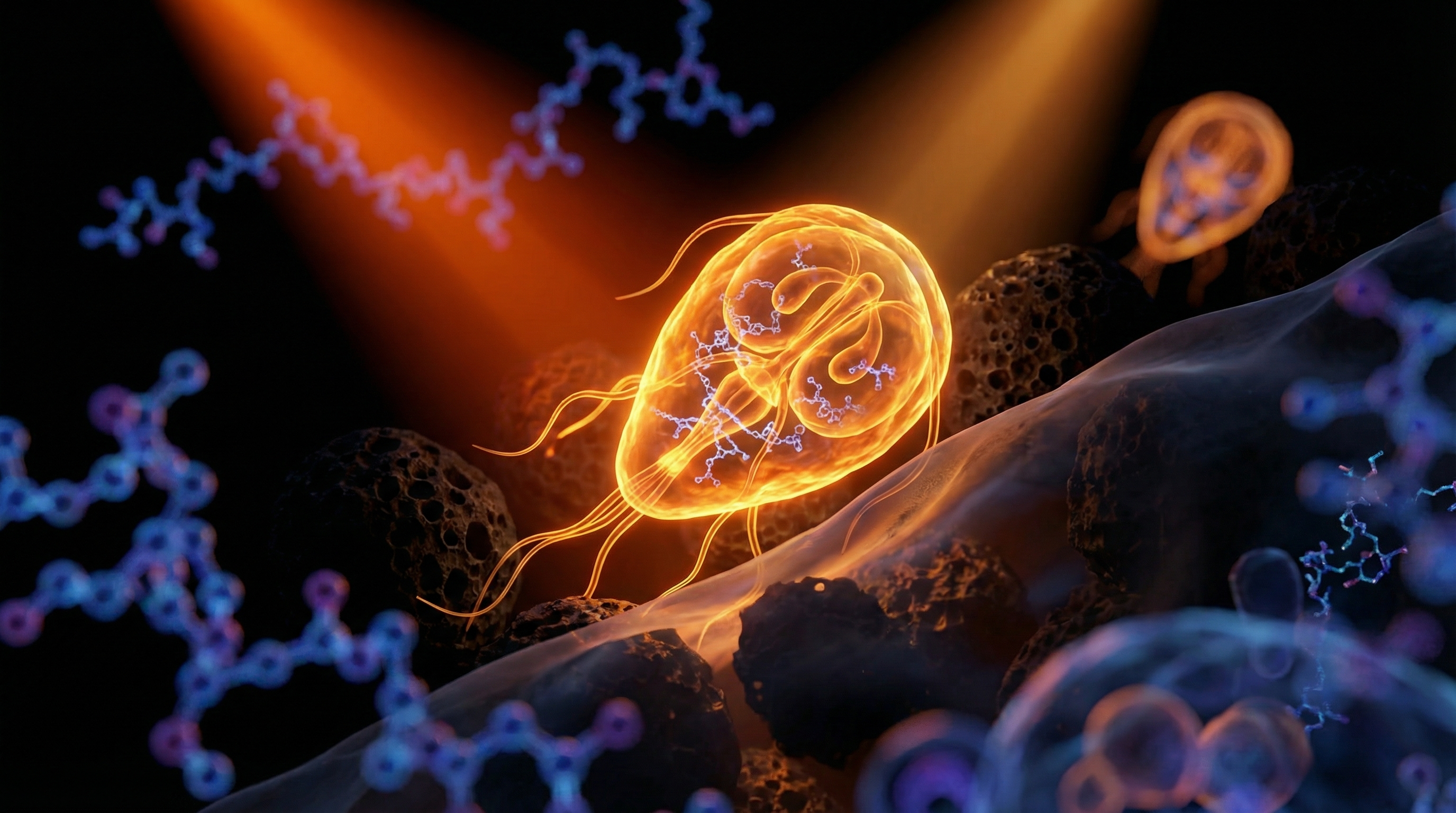
- —The Cyst (The Fortress): The cyst is the infective stage of the parasite. It is roughly oval-shaped and protected by a robust, multi-layered wall composed of chitin, a fibrous substance also found in the exoskeletons of insects. This wall renders the organism nearly impervious to cold temperatures, acidic environments, and most importantly, the oxidative stress of chlorine. A single cyst can survive for months in the cold waters of a Scottish loch, waiting for a host.
- —The Trophozoite (The Predator): Once the cyst is ingested and reaches the stomach, the low pH of gastric acid triggers a process called excystation. The cyst breaks open, releasing two trophozoites into the duodenum, the first part of the small intestine. The trophozoite is the active, motile, and pathogenic stage. It is famously pear-shaped, with two nuclei that give it the appearance of having a "face" under a microscope. It possesses four pairs of flagella—whip-like appendages—that allow it to navigate the turbulent flow of the intestinal lumen.
The Adhesive Disc: A Biological Suction Cup
The defining feature of the *Giardia* trophozoite is its ventral adhesive disc. This is a highly specialised organelle composed of microtubules and microribbons. The parasite uses this disc to physically attach itself to the epithelial lining (the enterocytes) of the host’s small intestine.
The attachment is not merely a passive clinging; it is a powerful mechanical suction. By adhering to the villi—the finger-like projections that increase the surface area for nutrient absorption—*Giardia* creates a physical barrier between the host and their food. This "carpeting" effect is the primary driver of the initial symptoms of the infection, but as we shall see, the damage goes far deeper than simple blockage.
Biological Truth: *Giardia* does not possess mitochondria in the traditional sense. Instead, it has "mitosomes," reduced organelles that reflect its adaptation to the low-oxygen environment of the gut. This unique biochemistry makes it susceptible to specific antibiotics like Metronidazole, but also allows it to evade many standard antimicrobial treatments.
##
##
Mechanisms at the Cellular Level
The "mainstream" view of giardiasis is that it is a simple "stomach bug" that causes temporary diarrhoea. This is a dangerous oversimplification. At the cellular level, *Giardia* initiates a sophisticated assault on the host's physiology that can lead to permanent changes in gut architecture and systemic health.
Disruption of the Brush Border
The small intestine is lined with a "brush border" of microvilli, which house essential enzymes for digestion. *Giardia* induces a profound shortening and blunting of these villi, a process known as villus atrophy. This is not caused by the parasite burrowing into the tissue (it is non-invasive), but rather through a combination of mechanical suction and the induction of host cell apoptosis (programmed cell death).
When the villi are blunted, the production of disaccharidases—the enzymes responsible for breaking down complex sugars—is catastrophically reduced. The most notable victim is lactase. This is why many people who suffer from a *Giardia* infection suddenly become severely lactose intolerant. Even after the parasite is cleared, the lactase deficiency can persist for months as the brush border attempts to regenerate.
Competition for Nutrients: The Arginine Drain
*Giardia* is a metabolic thief. It lacks the pathways to synthesise its own lipids and certain amino acids, so it must scavenge them from the host. One of its primary targets is the amino acid L-arginine.
The parasite possesses an enzyme called arginine deiminase (ADI), which it uses to rapidly consume available arginine in the intestinal lumen. Arginine is a critical precursor for the production of nitric oxide (NO) by the host's immune cells. Nitric oxide is one of the body’s primary defences against parasites—it inhibits their growth and movement. By depleting arginine, *Giardia* effectively disarms the host’s local immune response, allowing it to colonise the gut unimpeded. Furthermore, the loss of arginine contributes to the disruption of protein synthesis and cellular repair in the host.
The Breakdown of Tight Junctions
The integrity of the intestinal barrier is maintained by tight junction proteins such as occludin and zonula occludens-1 (ZO-1). Research has shown that *Giardia* trophozoites secrete proteases that degrade these proteins. The result is "leaky gut" or increased intestinal permeability.
When the tight junctions are compromised, undigested food particles, bacterial endotoxins (such as Lipopolysaccharides or LPS), and other pathogens can enter the bloodstream. This triggers a systemic inflammatory response, explaining why giardiasis is often accompanied by symptoms far removed from the gut, such as:
- —Chronic fatigue
- —Cognitive impairment ("brain fog")
- —Joint pain
- —Skin rashes (urticaria)
##
##
Environmental Threats and Biological Disruptors
In the UK, the narrative surrounding water safety is often one of complacency. We are told our tap water is among the cleanest in the world and our rivers are "improving." However, a closer look at the data from the Environment Agency and the Drinking Water Inspectorate (DWI) reveals a more concerning reality regarding *Giardia*.
The Failure of Chlorination
The primary method of water purification in the UK is chlorination. While chlorine is highly effective against most bacteria (such as *E. coli*), it is notoriously ineffective against *Giardia* cysts. The chitinous wall of the cyst is resistant to standard domestic chlorine concentrations.
Outbreaks in the UK have historically occurred when municipal water treatment plants fail to implement adequate UV irradiation or micro-filtration (sand filters). While large-scale plants are better equipped, private water supplies (wells and boreholes), which serve over a million people in the UK, are frequently inadequately treated for protozoan threats.
Sewage Spills and Agricultural Runoff
The UK’s sewage system is currently in a state of crisis. Combined Sewer Overflows (CSOs) are designed to release untreated sewage into rivers during heavy rainfall to prevent flooding. In 2023 alone, there were hundreds of thousands of such spills. *Giardia* is present in human faecal matter, and these spills introduce concentrated amounts of the parasite directly into recreational waters.
Furthermore, *Giardia* is a zoonotic parasite, meaning it can jump from animals to humans. The UK's high density of sheep and cattle farming contributes significantly to the environmental load. Runoff from pastures carries animal-derived *Giardia* cysts into streams and rivers.
Warning: The "pristine" mountain stream is a biological myth. In areas like the Peak District or the Highlands, the presence of livestock or wild deer upstream means that even the clearest water can be teeming with *Giardia* cysts.
The Wild Swimming Risk
The recent surge in wild swimming and "blue spaces" therapy has led to an increase in exposure. Many swimmers inadvertently swallow small amounts of water. Because the infective dose of *Giardia* is remarkably low—as few as 10 to 25 cysts can cause full-blown disease—a single "gulp" of river water is more than enough to initiate an infection.
##
##
The Cascade: From Exposure to Disease
The progression of giardiasis is often insidious. It does not always present as the "explosive" event people expect, which is why it so often goes undiagnosed for months or even years.
Incubation and Acute Phase
After ingestion, there is an incubation period of typically 1 to 3 weeks. This is significantly longer than common bacterial food poisoning (which usually hits within hours or a few days), often making it difficult for the patient to link their illness to a specific event or swimming trip.
The acute phase is characterised by:
- —Steatorrhoea: Greasy, foul-smelling, pale stools that tend to float. This is caused by fat malabsorption.
- —Extreme Flatulence and "Sulfur Burps": The parasite’s interference with the microbiome leads to the overgrowth of hydrogen-sulphide-producing bacteria.
- —Abdominal Cramping: Often localised in the upper abdomen (epigastric region), where the parasite is most active.
- —Nausea and Anorexia: A general loss of appetite and a feeling of "fullness" even after small meals.
The Chronic Transition
In many individuals, the body fails to clear the parasite entirely. This leads to chronic giardiasis. In this stage, the "explosive" symptoms may subside, replaced by a cycle of intermittent bloating, constipation or soft stools, and progressive weight loss.
The most devastating impact of chronic giardiasis is malabsorption syndrome. The blunted villi cannot absorb critical fat-soluble vitamins (A, D, E, K), Vitamin B12, Folic acid, and Iron. This leads to a secondary wave of health issues:
- —Iron-deficiency anaemia that does not respond to oral supplementation.
- —Osteoporosis or bone density loss due to Vitamin D and Calcium malabsorption.
- —Neurological symptoms stemming from B12 deficiency.
The Microbiome Shift
*Giardia* does not exist in a vacuum. It interacts dynamically with the gut microbiota. The presence of the parasite alters the local pH and nutrient availability, often favouring the growth of pathobionts while suppressing beneficial species like *Lactobacillus* and *Bifidobacterium*. This dysbiosis can persist long after the *Giardia* itself has been eradicated, leading to what is often misdiagnosed as "post-infectious IBS."
##
##
What the Mainstream Narrative Omits
The UK’s approach to giardiasis is reactive rather than proactive, and several critical biological truths are systematically omitted from public health discussions.
The "Shedding" Problem and Testing Failure
The standard diagnostic tool in the NHS is the O&P (Ova and Parasite) stool test. Patients are asked to provide a single stool sample, which is then examined under a microscope.
This method is catastrophically flawed for *Giardia*. The parasite is "shed" intermittently. A patient may have a high "load" of trophozoites in their duodenum but very few cysts being passed in the particular stool sample provided that day. Studies have shown that a single O&P test has a sensitivity as low as 50%.
To be remotely accurate, three samples must be taken on different days, yet this is rarely requested by overstretched GPs. Furthermore, the more modern PCR (Polymerase Chain Reaction) tests, which detect the DNA of the parasite, are far more accurate but are often restricted due to cost. Many patients are told they are "clear" based on one negative O&P test, while the parasite continues to ravage their gut.
The SIBO Connection
There is a profound and often ignored link between giardiasis and Small Intestinal Bacterial Overgrowth (SIBO). By disrupting intestinal motility and damaging the Migrating Motor Complex (MMC)—the "housekeeping" wave of the gut—*Giardia* creates an environment where bacteria from the large intestine can migrate upwards and colonise the small intestine.
When a patient successfully treats *Giardia* but finds their bloating and digestive distress remains, it is frequently because the parasite has left them with a secondary SIBO infection. The mainstream narrative rarely connects these dots, leaving patients in a cycle of "functional" illness with no clear cause.
Post-Infectious Irritable Bowel Syndrome (PI-IBS)
The medical establishment often uses the label "IBS" as a "wastepaper basket" diagnosis for symptoms they cannot explain. Research has shown that up to 40% of patients who suffer from an acute *Giardia* infection will develop long-term PI-IBS. This is not a "psychosomatic" condition; it is the result of permanent changes in gut sensitivity (visceral hypersensitivity) and low-grade mucosal inflammation that remains after the parasite is gone.
Critical Fact: Chronic giardiasis has been linked to the development of food allergies and histamine intolerance. By damaging the gut lining, the parasite allows large proteins to enter the immune system's view, leading to the development of IgE and IgG mediated sensitivities where none existed before.
##
##
The UK Context
The UK presents a unique set of challenges for the management of *Giardia*. Our climate—temperate, damp, and cool—is ideal for the survival of cysts in the environment.
Regional Hotspots
Data suggests that cases are not evenly distributed. Areas with high levels of outdoor tourism and intensive sheep farming show higher rates of infection.
- —The Lake District and Peak District: Popular swimming and hiking spots where water run-off from high-altitude pastures is common.
- —Scotland: Despite the "pure" image of Scottish water, rural areas often rely on private supplies that are not subject to the same rigorous testing as Scottish Water’s main network.
- —The River Wye and Thames: These rivers are currently at the centre of the sewage discharge scandal, making them high-risk zones for waterborne pathogens.
The NHS Burden
The NHS is currently ill-equipped to handle the rise in parasitic infections. The standard "wait and see" approach for diarrhoea is inappropriate for *Giardia*, which does not usually resolve without intervention. Furthermore, there is a lack of specialised training for GPs in tropical and parasitic medicine, leading to the "it’s just a virus" default diagnosis.
Regulatory Oversight
The Food Standards Agency (FSA) and Public Health England (PHE) track outbreaks, but their focus is largely on large-scale food contamination. Small-scale environmental exposure, such as that experienced by a swimmer or a dog walker (dogs are also highly susceptible and can transmit it to owners), often falls through the cracks of surveillance.
##
##
Protective Measures and Recovery Protocols
Given the hidden nature of the threat, individuals must take their digestive health into their own hands. Recovery from giardiasis requires a multi-faceted approach that addresses the parasite, the microbiome, and the structural damage to the gut.
Prevention in the Wild
If you are an outdoor enthusiast in the UK, do not trust the "cleanness" of any wild water source.
- —Filtration: Use a portable water filter rated to at least 0.1 microns. This is small enough to mechanically trap *Giardia* cysts.
- —Boiling: Bringing water to a rolling boil for at least one minute is the only 100% effective way to kill cysts.
- —UV Treatment: Handheld UV devices (like the SteriPEN) are effective, but only if the water is clear; turbidity (cloudiness) can shield the cysts from the UV light.
- —Hand Hygiene: Use soap and water after handling soil or being in areas with livestock. Alcohol-based hand gels are often ineffective against the tough chitin wall of the *Giardia* cyst.
Pharmacological Intervention
If an infection is confirmed, the first line of treatment is typically a nitroimidazole antibiotic:
- —Metronidazole: The most common treatment. It works by entering the parasite and causing DNA strand breakage. However, it is notorious for side effects, including a metallic taste and extreme nausea, and it must never be taken with alcohol (the "disulfiram-like" reaction).
- —Tinidazole: Often more effective and can sometimes be administered in a single, high-dose treatment, reducing the impact on the systemic microbiome.
Natural Antimicrobials and Support
For those with chronic, low-level infections or those looking to support their recovery, several natural compounds have shown significant anti-giardial activity in *in vitro* and *in vivo* studies:
- —Berberine: Found in Goldenseal and Barberry, berberine has been shown to be as effective as metronidazole in some clinical trials, with fewer side effects. It works by inhibiting the growth of trophozoites and preventing their attachment to the intestinal wall.
- —Allicin (from Garlic): A potent antimicrobial that disrupts the metabolic enzymes of the parasite.
- —Oil of Oregano: High in carvacrol and thymol, which can penetrate the lipid membranes of the trophozoites.
The Gut Recovery Protocol
Eradicating the parasite is only half the battle. To prevent the "Cascade" described above, the following steps are essential:
- —Enzyme Replacement: Temporary use of high-quality digestive enzymes (including lactase and lipase) to support nutrient absorption while the brush border heals.
- —Mucosal Repair: Supplementing with L-glutamine, Zinc carnosine, and Deglycyrrhizinated Licorice (DGL) to help seal the tight junctions and repair the villi.
- —Bile Acid Support: *Giardia* thrives in the presence of certain bile salts but is inhibited by others. Ensuring healthy bile flow can help make the small intestine a less hospitable environment for the parasite.
- —Probiotics: Specific strains, most notably *Saccharomyces boulardii* (a beneficial yeast), have been shown to compete with *Giardia* for attachment sites and stimulate the production of Secretory IgA, the gut's primary immune defence.
##
##
Summary: Key Takeaways
The threat of *Giardia lamblia* in the UK is a pressing public health issue that remains shrouded in biological ignorance and regulatory inadequacy. To protect oneself and recover from this hidden invader, one must understand the following:
- —Resilience is Key: *Giardia* cysts are resistant to chlorine and can survive for months in cold UK waters. Standard water treatment is not a guarantee of safety.
- —The "Face" of Malabsorption: The parasite uses its ventral disc to physically block nutrient absorption, leading to deficiencies in fats, vitamins, and minerals.
- —Testing is Flawed: A single negative stool test does not rule out giardiasis. PCR testing and multiple samples are necessary for an accurate diagnosis.
- —The Secondary Wave: The damage caused by *Giardia*—including SIBO, leaky gut, and lactose intolerance—often persists long after the parasite is gone.
- —Environmental Vigilance: The UK’s sewage crisis and agricultural practices make wild swimming and rural water supplies high-risk activities.
- —Comprehensive Recovery: Successful treatment requires more than just antibiotics; it necessitates a structured protocol to repair the gut lining and restore the microbiome.
In an age where we are encouraged to "reconnect with nature," we must do so with our eyes open to the microscopic realities of our environment. *Giardia* is a master of survival, but with the right knowledge and biological interventions, it is a threat that can be identified, exposed, and overcome. At INNERSTANDING, we remain committed to bringing these hidden truths to light, ensuring that your journey toward health is built on a foundation of scientific reality, not mainstream myth.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Giardiasis in the UK: Identifying the Hidden Waterborne Threat to Digestive Health"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Parasites & Pathogens — products curated by our research team for educational relevance and biological support.

Panaceum – Prebiotic Oligosaccharide Complex
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper