Heavy Metal Burden: Dementia vs Lead Toxicity
Cognitive decline in the UK elderly is often labeled as Alzheimer's without screening for heavy metal accumulation. We analyze how neurotoxic loads from environmental sources mimic neurodegenerative diseases.
# Heavy Metal Burden: Dementia vs Lead Toxicity
Overview
In the clinical corridors of the National Health Service (NHS), a silent, silver-grey shadow looms over the ageing population of the United Kingdom. Every three minutes, someone in the UK is diagnosed with dementia. By 2025, it is estimated that over one million Britons will be living with this debilitating condition. However, beneath the standardised diagnostic labels of Alzheimer’s Disease, Vascular Dementia, and Lewy Body Dementia lies a neglected clinical reality: the pervasive bioaccumulation of neurotoxic heavy metals, most notably Lead (Pb).
As a senior biological researcher at INNERSTANDING, my investigation into the "Dementia Epidemic" suggests that we are witnessing a massive diagnostic failure. For decades, the UK’s industrial legacy, Victorian-era plumbing, and the prolonged use of leaded petrol have created a "toxic debt" that is now being called in. The cognitive decline observed in the elderly is frequently indistinguishable from chronic, low-level Lead Toxicity. Yet, the current NHS protocols rarely, if ever, mandate a comprehensive heavy metal toxicology screen before assigning a permanent neurodegenerative diagnosis.
This article serves as a technical exposé into the biochemical mimicry between heavy metal burden and dementia. We will dissect how lead and other divalent cations infiltrate the central nervous system, disrupt cellular homeostasis, and why the mainstream medical establishment continues to overlook the environmental "poisoning" of the British mind.
Fact: Lead has no known biological role in the human body. Even at concentrations below current "safe" thresholds, it exerts profound neurotoxic effects, particularly in the ageing brain where the blood-brain barrier is compromised.
---
The Biology — How It Works

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus
Clean Slate is a cellular-level detoxifier that targets heavy metals, pesticides, and environmental toxins to unblock your body's natural defense pathways. It helps reduce systemic inflammation and restores the nutrient absorption sites often compromised by modern toxicity.
Vetting Notes
Pending
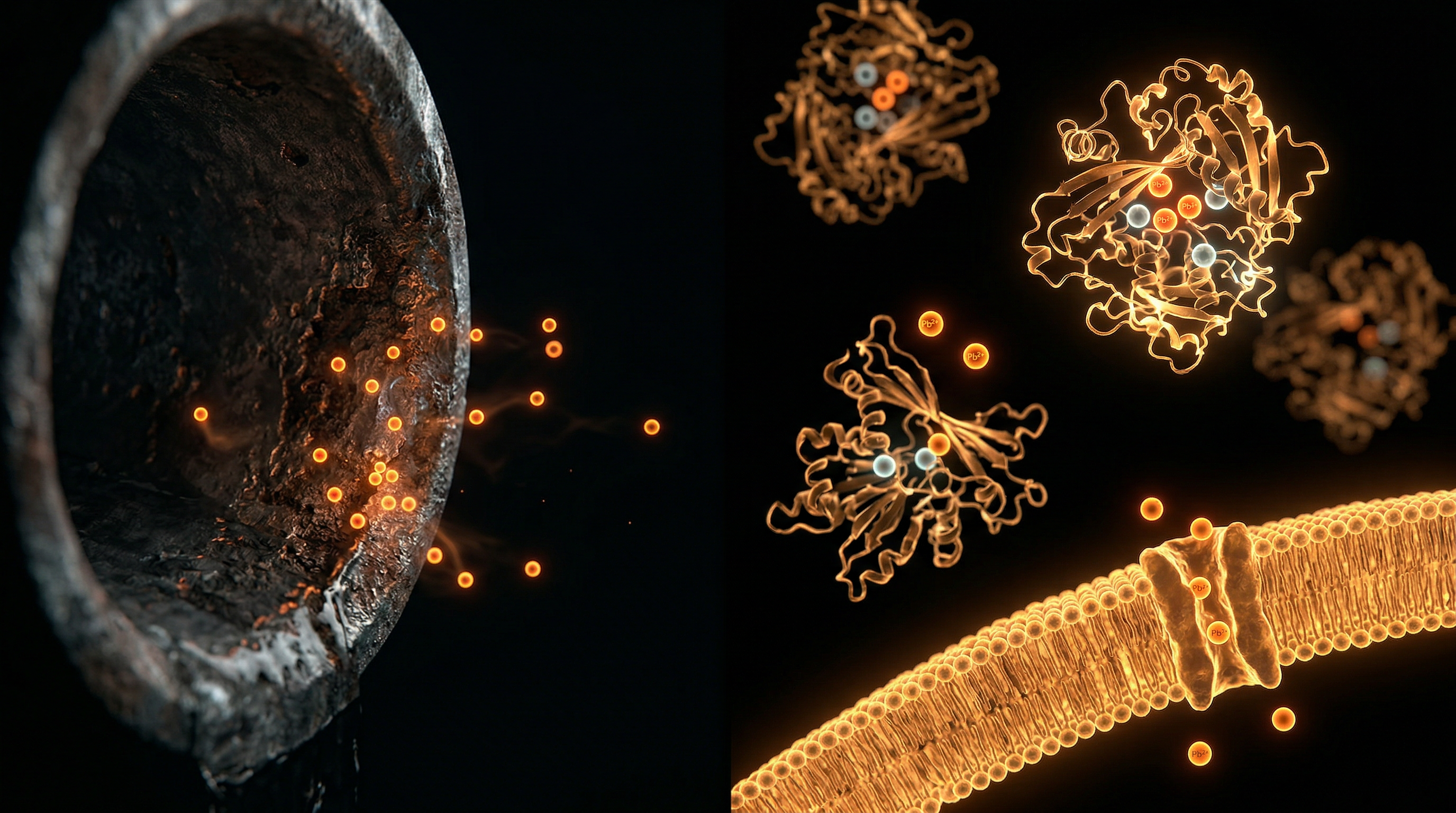
To understand why lead toxicity is so often mistaken for Alzheimer’s, one must first grasp the concept of Ionic Mimicry. Lead ($Pb^{2+}$) is a biological chameleon. Because its ionic radius and charge density are remarkably similar to essential minerals, specifically Calcium ($Ca^{2+}$) and Zinc ($Zn^{2+}$), the body’s transport systems are unable to distinguish the toxin from the nutrient.
The Trojan Horse Effect
The human brain is protected by the Blood-Brain Barrier (BBB), a highly selective semi-permeable border of endothelial cells. Under normal physiological conditions, the BBB prevents toxins from entering the neural parenchyma. However, lead utilizes the Calcium-ATPase pumps and Voltage-Gated Calcium Channels to bypass this barrier. Once inside the brain, lead does not simply sit inert; it integrates into the metabolic machinery of the neuron.
Displacement of Essential Cofactors
Lead's affinity for certain protein binding sites is often thousands of times stronger than that of the natural minerals. When lead replaces zinc in Zinc-Finger Proteins, it alters the structural integrity of DNA-binding proteins, leading to aberrant gene expression. When it replaces calcium in the synaptic vesicles, it triggers the premature release of neurotransmitters, particularly Glutamate, leading to chronic Excitotoxicity. This state of constant low-level excitation is a hallmark of the early stages of cognitive decline, yet it is rarely investigated as a toxicological event.
The Storage Reservoir: Bone-to-Blood Flux
One of the most insidious aspects of lead biology is its residence time. Approximately 90–95% of a lead burden in an adult is stored in the Hydroxyapatite matrix of the bone. In the UK’s elderly population, particularly post-menopausal women, the natural process of Osteoporosis or bone resorption causes this sequestered lead to be released back into the bloodstream. This creates a "secondary exposure" event decades after the original environmental contact, manifesting as sudden-onset cognitive impairment that clinicians reflexively label as "Age-Related Dementia."
---
Mechanisms at the Cellular Level
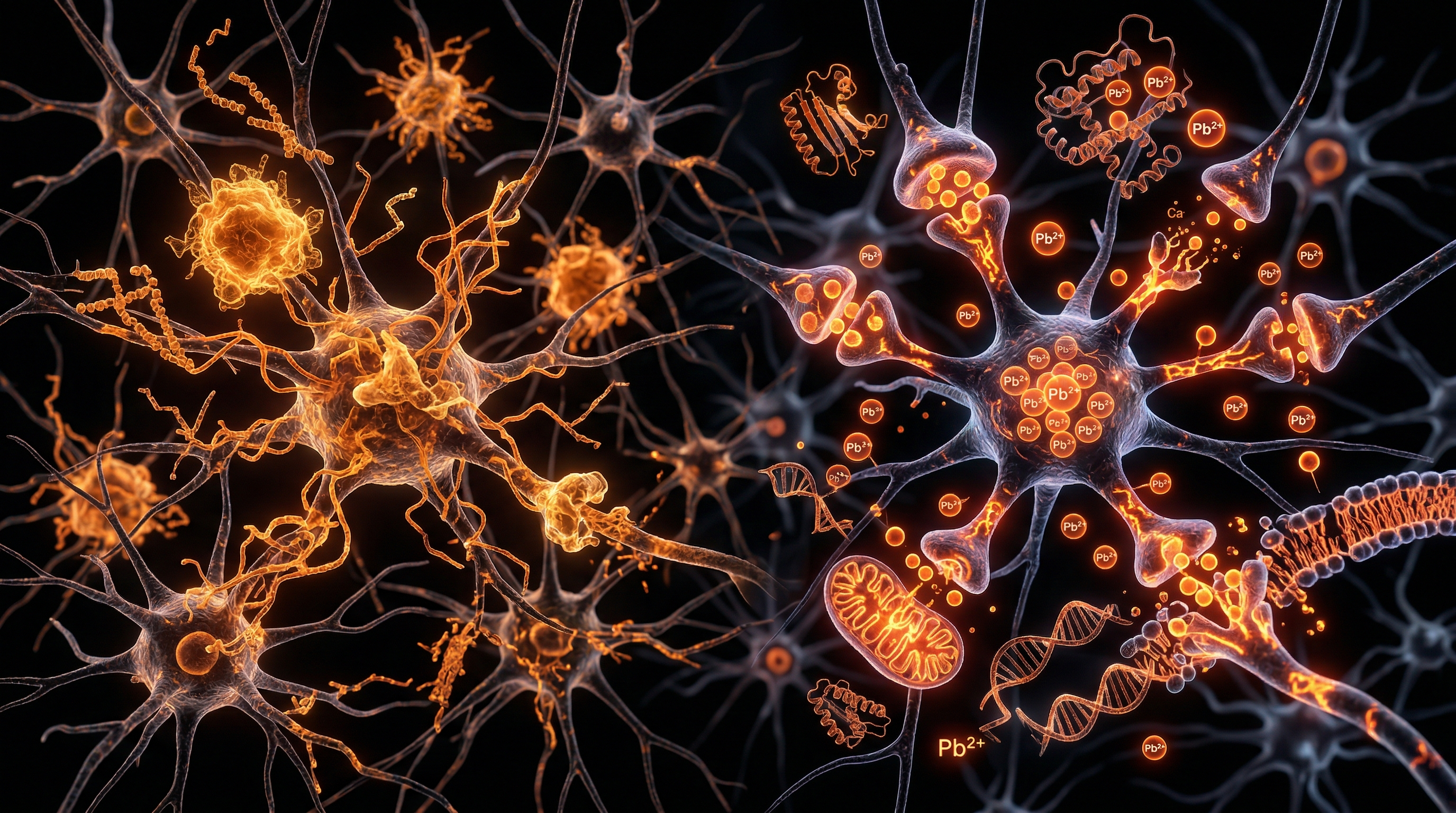
The transition from a healthy neuron to a "demented" one is characterized by several cellular pathologies: oxidative stress, mitochondrial failure, and the accumulation of protein aggregates. Lead acts as a catalyst for every single one of these processes.
Oxidative Stress and Lipid Peroxidation
Lead induces the formation of Reactive Oxygen Species (ROS) while simultaneously depleting the brain’s primary antioxidant, Glutathione (GSH). It binds to the sulfhydryl (-SH) groups of enzymes involved in the antioxidant cycle, rendering them inactive. The resulting oxidative stress leads to Lipid Peroxidation of the neuronal membranes. Since the brain is the most lipid-rich organ in the body, this process effectively "corrodes" the neural circuitry.
Mitochondrial Dysfunction
The Mitochondria are the powerhouses of the cell, and they are primary targets for heavy metal toxicity. Lead interferes with the Electron Transport Chain (ETC) by inhibiting Cytochrome C Oxidase. This leads to a drop in Adenosine Triphosphate (ATP) production. A brain without energy cannot maintain the ion gradients necessary for signal transmission, resulting in the "brain fog" and memory lapses often associated with early-stage Alzheimer's.
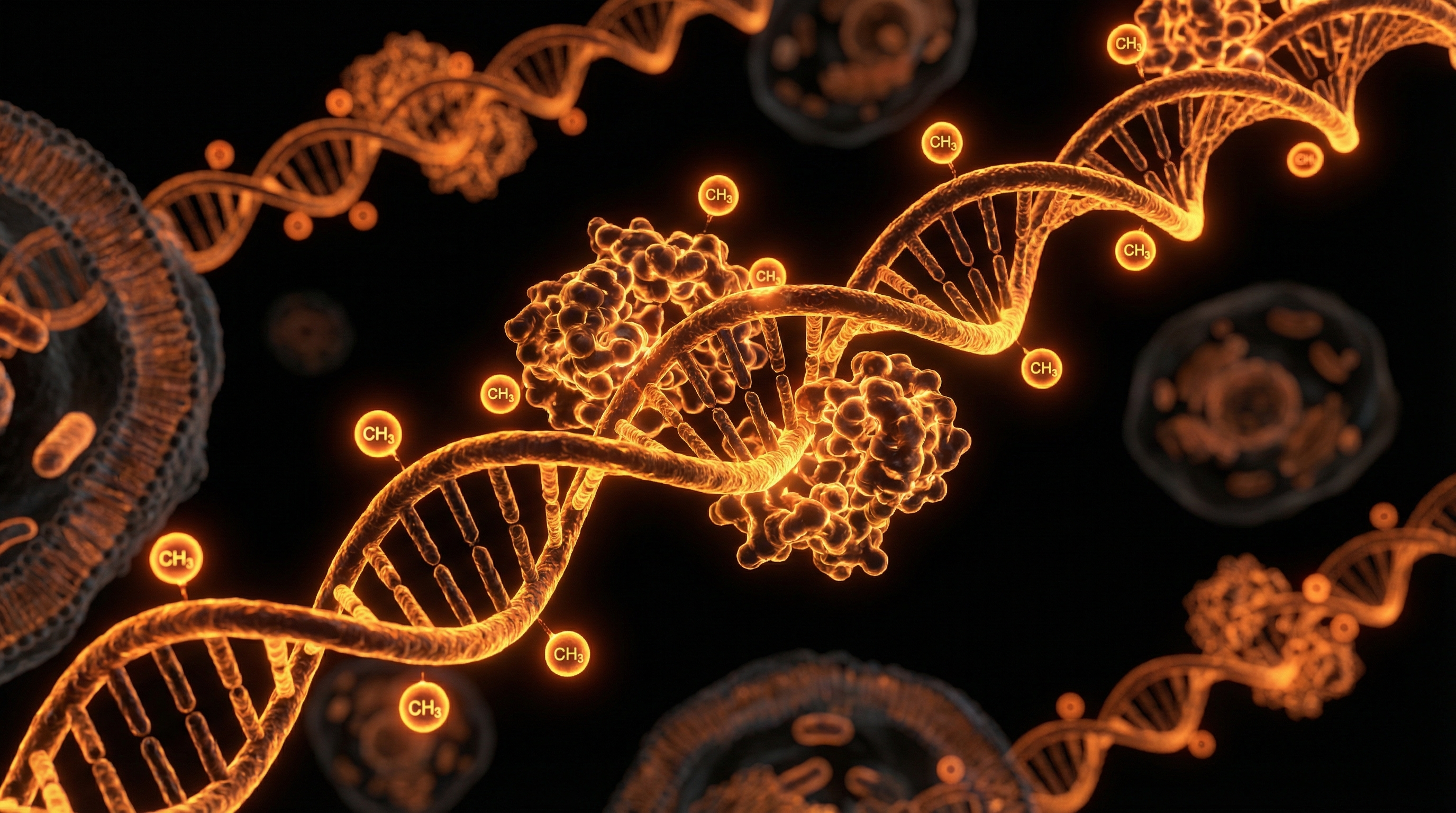
The Amyloid Link
Perhaps the most damning evidence is lead's role in the formation of Beta-Amyloid Plaques. Research indicates that early-life exposure to lead can reprogram the expression of the Amyloid Precursor Protein (APP) and the enzyme BACE1. This is an Epigenetic shift. Lead exposure effectively "primes" the brain to produce the very plaques that are used to pathologically confirm an Alzheimer's diagnosis.
- —Lead and Tau Protein: Lead exposure has been shown to increase the phosphorylation of Tau proteins, leading to the formation of Neurofibrillary Tangles, another classic marker of dementia.
- —Microglial Activation: Heavy metals trigger a chronic inflammatory response in the Microglia (the brain’s immune cells), leading to a state of permanent neuro-inflammation.
---
Environmental Threats and Biological Disruptors
The United Kingdom possesses a unique environmental profile that exacerbates heavy metal accumulation. Our industrial history, though a source of national pride, has left a legacy of contamination that remains largely unaddressed in public health circles.
The Leaded Petrol Legacy
Until the gradual phase-out in the 1990s, the UK burnt thousands of tonnes of Tetraethyl Lead as a fuel additive. This lead did not disappear; it settled in the topsoil of our urban centres and along the verges of our motorways. The "Leaded Generation"—those born between 1950 and 1980—have spent decades inhaling and ingesting particulate lead. This cohort is now entering the age range where dementia diagnoses are most prevalent.
Victorian Infrastructure and Water
A significant portion of the UK’s housing stock predates 1970. In cities like London, Glasgow, and Manchester, Lead Piping is still present in the internal plumbing of older buildings or in the "communication pipes" owned by water companies. While the water is treated with orthophosphates to reduce leaching, changes in water chemistry, pipe disturbances, or the use of water softeners can lead to spikes in lead ingestion.
Statistic: It is estimated that up to 25% of domestic properties in the UK still have some form of lead plumbing. For an elderly person with decreased renal clearance, even "trace" amounts of lead in drinking water are cumulative.
Industrial "Hotspots" and Air Quality
The UK’s history of coal-fired power stations and smelting has left significant concentrations of heavy metals (including Cadmium and Mercury) in the environment. These metals act synergistically with lead, creating a "cocktail effect" where the combined neurotoxicity is greater than the sum of its parts.
---
The Cascade: From Exposure to Disease
The progression from environmental exposure to a clinical diagnosis of "dementia" is a multi-decade cascade. It is not an acute event but a slow erosion of the Neurological Reserve.
Stage 1: Bioaccumulation and Sequestration
During the middle years, the body successfully sequesters lead into the skeletal system. The individual may appear healthy, though they might suffer from non-specific symptoms such as hypertension, irritability, or "mild" kidney dysfunction—all of which are known effects of lead but are rarely connected to it.
Stage 2: The Metabolic Trigger
As the individual ages, several factors trigger the release of bone-stored lead:
- —Hormonal Changes: The drop in oestrogen during menopause increases bone turnover.
- —Nutritional Deficiencies: Low intake of Calcium or Vitamin D forces the body to "mine" the bones for minerals, releasing lead in the process.
- —Physical Inactivity: Weight-bearing exercise maintains bone density; its absence accelerates resorption.
Stage 3: Neurotoxic Influx
The released lead floods the circulatory system. In an ageing body with a less efficient Glomerular Filtration Rate (GFR) in the kidneys, the lead remains in the blood longer, eventually crossing the now-leaky blood-brain barrier.
Stage 4: Symptomatic Mimicry
The patient begins to exhibit:
- —Short-term memory loss (due to hippocampal damage).
- —Executive dysfunction (frontal lobe interference).
- —Personality changes (disruption of neurotransmitter balance).
At this point, a GP will typically conduct a Mini-Mental State Examination (MMSE) and, seeing the decline, refer the patient to a memory clinic. The possibility of lead toxicity is almost never raised.
---
What the Mainstream Narrative Omits
The refusal to integrate toxicology into geriatric psychiatry is not merely an oversight; it is a systemic blind spot. The mainstream narrative focuses almost exclusively on "managing" the symptoms of dementia with drugs like Donepezil or Memantine, rather than investigating potentially reversible environmental causes.
The Pharmaceutical Bias
There is no "patentable" drug for lead detoxification that offers the same profit margins as long-term dementia management. Chelation therapy, the process of removing heavy metals, involves older, off-patent compounds like EDTA or DMSA. Consequently, there is little incentive for large-scale clinical trials within the current medical-industrial complex.
The Myth of "Safe Levels"
The NHS and Public Health England often cite "action levels" for lead in blood (typically 10 µg/dL for adults). However, the World Health Organisation (WHO) and the CDC have admitted that there is no safe level of lead exposure. Low-level chronic exposure (e.g., 2–5 µg/dL) is sufficient to cause cognitive impairment in the elderly, yet these levels are dismissed as "normal" or "insignificant" by standard UK labs.
Misinterpretation of Biomarkers
A standard blood test only shows lead exposure from the last 30–90 days. It does not reflect the Total Body Burden stored in the bones. To accurately assess the lead-dementia link, one would need a K-shell X-ray Fluorescence (KXRF) bone scan or a Provoked Urine Challenge. Neither of these are available on the NHS for routine cognitive screening.
---
The UK Context
The United Kingdom presents a specific set of challenges regarding the heavy metal-dementia nexus. The NHS Long Term Plan focuses heavily on early diagnosis of dementia but fails to address the underlying environmental aetiology.
The Postcode Lottery of Toxicity
Regions with a heavy industrial past—the "Black Country," South Yorkshire, and the Clydeside—show higher rates of dementia. While lifestyle factors like smoking and diet are often blamed, the soil in these areas contains significantly higher levels of lead and cadmium.
The Housing Crisis
As the UK struggles with a housing shortage, many older Victorian and Edwardian terraces are being renovated. These renovations often disturb layers of lead-based paint and old lead piping, aerosolising lead dust that is inhaled by the elderly residents. Without proper PPE or awareness, these minor home improvements can trigger a rapid cognitive decline.
The NICE Guidelines Gap
The National Institute for Health and Care Excellence (NICE) guidelines for dementia (NG97) do not mention heavy metal screening as part of the diagnostic workup. This omission means that thousands of British citizens are potentially being treated for an "incurable" brain disease when they are actually suffering from a "treatable" toxic overload.
---
Protective Measures and Recovery Protocols
If we accept that a significant portion of dementia cases are influenced or caused by heavy metal burden, the clinical approach must shift from "management" to "detoxification and protection."
Nutritional Antagonists
The first line of defence is to ensure the body has an abundance of the minerals that lead tries to displace.
- —Calcium and Magnesium: Competitive inhibition at the gut and cellular level.
- —Selenium: A vital cofactor for Glutathione Peroxidase, which protects neurons from metal-induced oxidative stress.
- —Zinc: Essential for maintaining the blood-brain barrier and DNA repair.
Targeted Chelation and Support
While clinical chelation should only be performed under expert supervision, certain natural compounds can assist in reducing the metal burden:
- —N-Acetyl Cysteine (NAC): Boosts internal glutathione levels to help the liver process toxins.
- —Alpha-Lipoic Acid (ALA): A unique antioxidant that can cross the blood-brain barrier and has been shown to chelate metals within the brain tissue.
- —Modified Citrus Pectin: Shown in small trials to increase the urinary excretion of lead without depleting essential minerals.
Environmental Remediation
For those living in older UK properties:
- —Water Filtration: Using high-quality filters (e.g., reverse osmosis or specialized lead-removal filters) is mandatory.
- —Dust Control: Using HEPA-filtered vacuums to capture lead dust from old paint or outdoor soil.
- —Bone Health: Maintaining bone density through weight-bearing exercise and Vitamin K2/D3 supplementation is critical to prevent the release of stored lead into the blood.
---
Summary: Key Takeaways
The "Dementia Crisis" in the United Kingdom is not a simple biological inevitability. It is, in many cases, the clinical manifestation of an environmental catastrophe.
- —Mimicry: Lead toxicity mimics Alzheimer’s by displacing calcium, inducing oxidative stress, and promoting the formation of amyloid plaques.
- —The Bone Reservoir: The UK's elderly are "self-poisoning" as lead stored in their bones from the mid-20th century is released during age-related bone loss.
- —Diagnostic Failure: The NHS protocols for dementia are incomplete. A diagnosis of Alzheimer's without a heavy metal screen is a speculative diagnosis.
- —Regulatory Silence: The "safe" levels of lead are a myth; any level of neurotoxic metal accumulation contributes to the degradation of the British mind.
- —Hope through Intervention: By identifying the heavy metal burden and utilizing nutritional and chelation protocols, the "irreversible" decline of dementia may, in some cases, be slowed or even partially reversed.
As researchers and citizens, we must demand that the National Health Service updates its diagnostic criteria. We must move beyond the "amyloid-only" narrative and acknowledge the toxic burden that our industrial heritage has placed upon our elders. Only by clearing the lead from the system can we hope to clear the fog from the mind.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Heavy Metal Burden: Dementia vs Lead Toxicity"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on NHS Misdiagnosis Patterns — products curated by our research team for educational relevance and biological support.
Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper