The Ileocecal Valve: Mechanical Failure and Retrograde Colonization
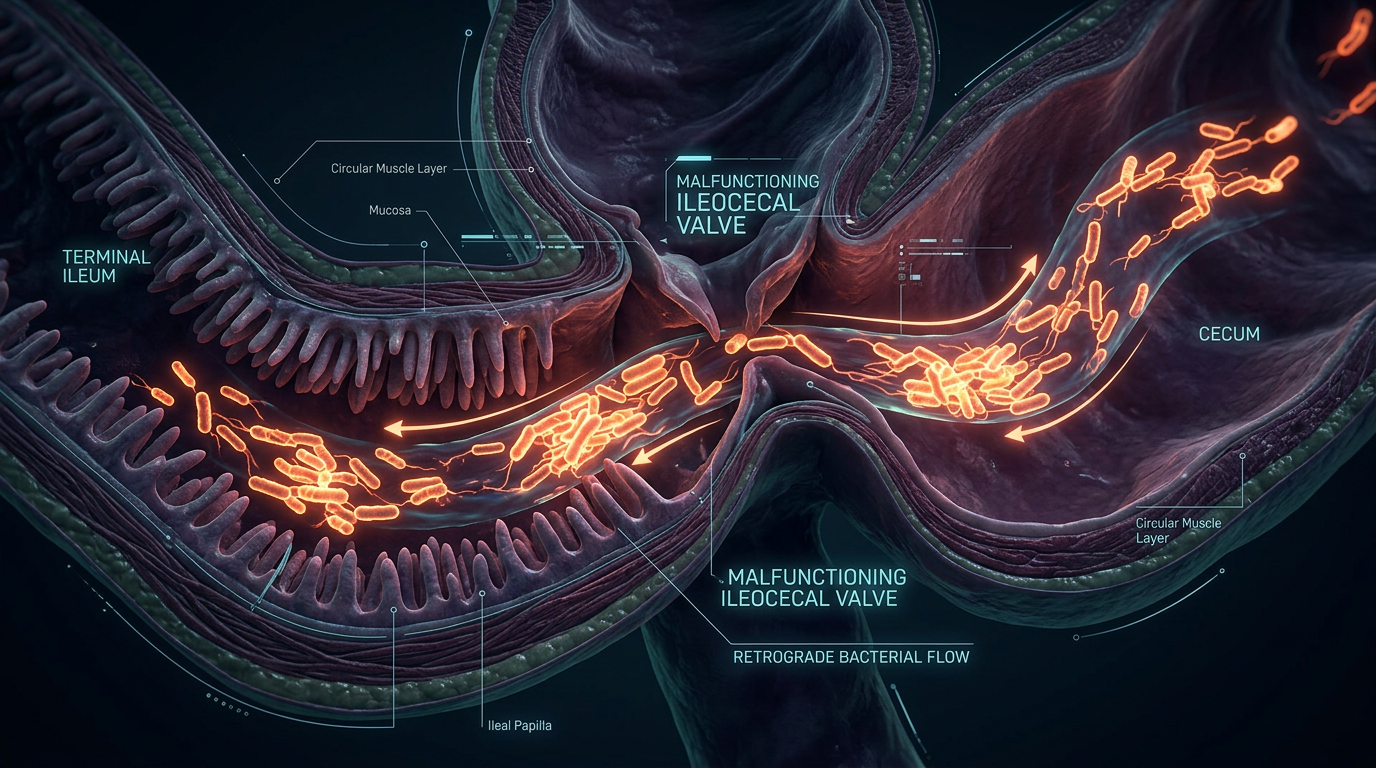
The ileocecal valve acts as a one-way gate preventing colonic bacteria from back-flowing into the small intestine. When this valve becomes stuck open due to inflammation or stress, the small intestine is flooded with unwanted microbes.
Overview
In the intricate architecture of the human digestive tract, precision is not merely a preference—it is a biological imperative. We often speak of the gut as a single, continuous tube, yet this reductionist view ignores the critical compartmentalisation required for health. At the junction where the distal small intestine (the ileum) meets the proximal large intestine (the caecum) lies one of the most vital, yet routinely ignored, structures in clinical medicine: the Ileocecal Valve (ICV).
The ICV is far more than a simple flap of tissue; it is a sophisticated, neuro-muscular gatekeeper. Its primary evolutionary purpose is twofold: to regulate the passage of nutrient-depleted chyme into the large intestine and, more crucially, to prevent the retrograde colonization of the small intestine by the trillion-strong microbial city residing in the colon. When this mechanical and physiological barrier fails, the result is not merely "indigestion"—it is a catastrophic breach of internal borders.
The "stuck open" ileocecal valve represents a fundamental mechanical failure that facilitates a microbial insurrection. In this state, the small intestine, which should remain relatively sterile to facilitate nutrient absorption, is flooded with colonic bacteria. This process, known as retrograde translocation, is the primary driver behind the epidemic of Small Intestinal Bacterial Overgrowth (SIBO). As a senior biological researcher for INNERSTANDING, I contend that the mainstream focus on "killing" bacteria with antibiotics is a flawed strategy if the mechanical gate remains broken. We must look at the structural integrity of the valve itself to understand why modern chronic illness has become an intractable maze.
In the United Kingdom, digestive complaints account for nearly 1 in 10 GP consultations, yet the functional integrity of the ileocecal valve is almost never assessed during standard physical examinations or via NHS diagnostic pathways.
##
The Biology — How It Works
To understand the failure of the ICV, we must first appreciate its masterful design. Anatomically, the valve is situated at the lower right quadrant of the abdomen. It is composed of two lips—the superior and inferior labia—which protrude into the lumen of the caecum. This structure functions as a passive flap valve, where the pressure within the caecum naturally pushes the lips together, sealing the entrance to the small intestine.
However, the ICV is also an active sphincter. It is controlled by a complex interplay of the Enteric Nervous System (ENS), the autonomic nervous system, and local myogenic (muscle-driven) responses.
The Muscular Architecture
The valve consists of a thickening of the circular smooth muscle layer of the ileum. Unlike the rest of the intestinal tract, which relies on rhythmic peristalsis to move contents forward, the ICV maintains a state of tonic contraction. This means it is naturally "shut" until a specific signal commands it to open.
Neural Control and the Gastroileal Reflex
The opening of the ICV is largely governed by the Gastroileal Reflex. When we ingest food, the stomach distends, sending a long-range neural signal to the ileum. This signal triggers the relaxation of the ICV and intensifies ileal peristalsis, allowing the remains of the previous meal to pass into the colon to make room for the new one. This reflex is mediated by the Vagus Nerve—the highway of the parasympathetic nervous system.
If the Vagus nerve is compromised—through chronic stress, physical trauma, or neurotoxicity—the timing of this reflex becomes desynchronised. The valve may remain open far longer than necessary or fail to close entirely, leaving the door wide open for colonic invaders.
The Pressure Gradient
Under normal physiological conditions, the pressure in the distal ileum is significantly higher than the pressure in the caecum. This gradient ensures "one-way traffic." However, when the colon becomes distended due to constipation, gas from fermentation, or poor motility, the pressure within the caecum can equalise or exceed that of the ileum. In this scenario, the mechanical pressure forces the ICV open in reverse, directly injecting colonic bacteria into the ileum.
##
Mechanisms at the Cellular Level
At the microscopic level, the ICV’s function depends on the health of the Interstitial Cells of Cajal (ICCs). These cells are often described as the "pacemakers" of the gut. They generate the electrical slow waves that coordinate smooth muscle contraction and relaxation.
The Role of Calcium Signaling
Contraction of the ICV is a calcium-dependent process. Within the smooth muscle cells of the valve, an influx of calcium ions triggers the binding of calmodulin, which activates myosin light-chain kinase. This molecular "switch" maintains the tonic closure of the valve. Disruptions in mineral homeostasis—specifically deficiencies in magnesium or imbalances in calcium—can lead to either a spastic valve (stuck shut) or an atonic valve (stuck open).
Hormonal Modulation
The ICV is also sensitive to gastrointestinal hormones:
- —Gastrin: Secreted by the stomach, it promotes the relaxation of the ICV to allow chyme transit.
- —Peptide YY (PYY): Often called the "ileal brake," PYY is released when fats reach the ileum. It signals the ICV to slow down or close, ensuring the small intestine has enough time to absorb lipids before they pass into the colon.
- —Motilin: This hormone triggers the Migrating Motor Complex (MMC), the "housekeeping" wave of the small intestine. If motilin levels are low, the MMC fails, and the ICV loses its "rhythm," frequently resulting in a persistent open state.
The Myenteric Plexus Dysfunction
The myenteric plexus, a network of nerves located between the muscle layers of the gut, provides the local intelligence for the ICV. In states of chronic inflammation (such as that caused by a high-sugar or high-processed-fat diet), these nerve endings can become "stunned" or damaged by oxidative stress. When the myenteric plexus fails to send the "close" signal, the ICV remains flaccid, a condition we term Ileocecal Insufficiency.
##
Environmental Threats and Biological Disruptors
The modern world is effectively a laboratory for ICV dysfunction. We are exposed to a myriad of factors that specifically target the neural and muscular integrity of this gatekeeper.
The Impact of Glyphosate
One of the most insidious threats to the ICV is the herbicide glyphosate. As a senior researcher, I have highlighted the role of glyphosate as a potent disruptor of the gut-brain axis. Glyphosate acts as a glycine analogue, potentially misincorporating into proteins and interfering with the synthesis of neurotransmitters like serotonin, 90% of which is produced in the gut. Serotonin is essential for proper intestinal motility and the signaling that keeps the ICV functional. Furthermore, glyphosate targets the Shikimate pathway in gut bacteria, leading to dysbiosis that increases caecal pressure and stresses the valve mechanism.
Ultra-Processed Foods (UPFs) and Emulsifiers
The British diet is now composed of over 50% ultra-processed foods. These products contain emulsifiers (like carboxymethylcellulose and polysorbate 80) that are designed to blend oil and water. In the gut, these same chemicals dissolve the protective mucus layer that shields the ICV. Without this mucus, the valve becomes inflamed, swollen, and loses its ability to form a tight seal.
Chronic Sympathetic Dominance (The Stress Factor)
The body cannot digest and defend simultaneously. When the "Fight or Flight" system (the sympathetic nervous system) is dominant, blood is shunted away from the digestive tract. In this state, the Vagus nerve is suppressed. Since the Vagus nerve is responsible for the tonic control of the gut's sphincters, chronic stress leads to a loss of tone in the ICV. This is why many people report that their SIBO symptoms—bloating and gas—flare up during periods of high emotional stress. It is not "all in their head"; it is a mechanical failure of the ICV due to neurological withdrawal.
Physical Trauma and Adhesions
Modern medicine often overlooks the structural. Abdominal surgeries (such as appendectomies or C-sections), endometriosis, or even old sports injuries can create adhesions—bands of scar tissue that "tether" the intestines. If an adhesion pulls on the caecum or the terminal ileum, it can mechanically distort the shape of the ICV, preventing it from closing.
##
The Cascade: From Exposure to Disease
What happens when the ICV fails and retrograde colonization begins? The sequence is predictable and devastating.
Stage 1: The Microbial Invasion
Bacteria that belong in the large intestine (such as *E. coli*, *Klebsiella*, and *Bacteroides*) migrate through the open valve into the ileum. The ileum is not designed to house these populations. Unlike the colon, which has a thick, double-layered mucus barrier, the small intestine has a thinner, more permeable barrier to allow for nutrient absorption.
Stage 2: Fermentation in the Wrong Place
These colonic bacteria begin to ferment the carbohydrates and fibres that have not yet been absorbed. This fermentation produces gases—hydrogen, methane, and hydrogen sulphide—directly in the small intestine. Because the small intestine is a narrow tube, this gas causes intense pressure and distension, leading to the characteristic "6-month pregnant" bloat seen in SIBO patients.
Stage 3: Deconjugation of Bile Acids
The invading bacteria begin to "deconjugate" bile acids. Bile is essential for fat digestion and for keeping the small intestine clean. When bile acids are deconjugated, they become toxic to the intestinal lining and lose their ability to emulsify fats. This leads to malabsorption of fat-soluble vitamins (A, D, E, K) and fatty stools (steatorrhoea).
Stage 4: Intestinal Permeability and LPS Translocation
The inflammation caused by the bacterial presence and the deconjugated bile acids breaks down the "tight junctions" between the cells of the small intestine. This is Leaky Gut. Colonic bacteria also produce Lipopolysaccharides (LPS)—endotoxins that can now enter the bloodstream.
Statistical evidence suggests that LPS translocation is a primary driver of systemic inflammation in the UK population, linked to the rise in autoimmune conditions, chronic fatigue syndrome, and even "brain fog" via the activation of neuroinflammation.
##
What the Mainstream Narrative Omits
The current medical model treats the gut as a series of chemical reactions, ignoring its nature as a mechanical and biological system. There are three major "omissions" in the mainstream narrative regarding the ICV.
1. The Appendicular Connection
The appendix is often dismissed as a vestigial organ. In reality, it is a "safe house" for beneficial bacteria and a lymphoid organ situated right next to the ICV. The appendix secretes immunoglobulins (IgA) that help regulate the microbial balance at the ileocecal junction. When the appendix is removed (as is common in the UK), the local immune surveillance of the ICV is compromised, making it far more likely for the valve to fail or for retrograde colonization to occur.
2. Visceral Dynamics
GPs rarely, if ever, palpate the abdomen to check the physical tension of the ICV. Osteopaths and visceral manipulators have long understood that "the map is not the territory." You can have "normal" blood tests and still have a valve that is physically spasmed or stuck. Mainstream medicine’s reliance on imaging often misses functional mechanical failures that only show up under dynamic conditions.
3. The Lymphatic Congestion
The area around the ICV is one of the most lymph-dense regions of the body (Peyer's Patches). When the ICV is stuck open, the constant influx of bacteria overwhelms the local lymphatic system. This leads to "clogged" lymphatics in the mesentery, which can cause chronic lower back pain and pelvic congestion—symptoms that are rarely linked back to a faulty ileocecal valve by standard medical practitioners.
##
The UK Context
The United Kingdom faces a unique set of challenges regarding ileocecal health. The convergence of dietary habits, sedentary lifestyles, and a healthcare system under strain has created a "perfect storm" for retrograde colonization.
The NHS Logjam
The typical UK patient with ICV-related symptoms is diagnosed with IBS (Irritable Bowel Syndrome). In the UK, IBS is often treated as a "wastepaper basket" diagnosis—something given when the doctor doesn't know what's wrong but wants to rule out more serious pathology like Crohn's or bowel cancer.
Research indicates that up to 78% of people diagnosed with IBS in the UK actually have SIBO, many of whom have an underlying mechanical failure of the ileocecal valve.
However, SIBO breath testing is not universally available on the NHS, and many GPs are not trained to recognise the symptoms of an open ICV. This leads to years of patient suffering and the over-prescription of proton pump inhibitors (PPIs), which actually worsen the problem by reducing stomach acid—the body’s first line of defence against bacterial overgrowth.
The Sedentary Crisis
Britain is one of the most sedentary nations in Europe. Lack of movement reduces "visceral motility." Without the natural "massaging" of the organs that comes from walking and twisting, the ICV can become physically stagnant. Combined with the "British Slouch"—a posture that compresses the abdominal cavity—the physical space for the ICV to operate correctly is often compromised.
##
Protective Measures and Recovery Protocols
Healing a failed ICV and stopping retrograde colonization requires a multi-pronged approach that addresses the mechanical, the chemical, and the neurological.
1. Manual ICV Release
One of the most effective ways to "reset" the valve is through manual therapy. This can be done by a practitioner or even at home. By applying firm, upwards and medially directed pressure to the area (halfway between the belly button and the right hip bone) during an exhale, one can manually encourage a spasmed valve to relax or an open valve to close. This "physical therapy for the gut" is often the missing piece in SIBO recovery.
2. Restoring the Vagus Nerve
Since the Vagus nerve controls the "gatekeeper," tonifying this nerve is essential.
- —Gargling: Vigorous gargling with water several times a day activates the muscles at the back of the throat, which are innervated by the Vagus nerve.
- —Cold Exposure: Splashing the face with ice-cold water or taking cold showers stimulates the "diving reflex," which increases vagal tone.
- —Deep Diaphragmatic Breathing: Focusing on a long, slow exhale (longer than the inhale) signals the nervous system to shift from sympathetic to parasympathetic mode, allowing the ICV to regain its natural rhythm.
3. Dietary Interventions
To reduce the pressure on the ICV, we must stop the "fermentation factory" in the small intestine.
- —The Low-FODMAP Diet: A temporary reduction in fermentable carbohydrates can lower the gas pressure in the colon, allowing the ICV to close more easily.
- —Prokinetic Agents: Substances like ginger, triphala, or low-dose erythromycin (when prescribed) can stimulate the Migrating Motor Complex, ensuring the small intestine is "swept clean" and preventing bacteria from settling near the valve.
- —Bitters: Using herbal bitters (like dandelion or gentian) before meals stimulates the entire digestive cascade—from stomach acid to bile flow—which naturally reinforces the "one-way" direction of the gut.
4. Antimicrobial Hygiene
While the goal is mechanical repair, the existing overgrowth must be managed. However, instead of broad-spectrum antibiotics, we favour "selective" herbal antimicrobials like Allicin (from garlic), Berberine, and Oregano oil. These help to clear the retrograde colonization without the collateral damage caused by pharmaceutical agents.
5. Managing the "Pressure from Below"
Chronic constipation is the enemy of the ICV. If the colon is full, the valve cannot close. Ensuring adequate hydration, magnesium intake (specifically magnesium citrate or malate), and using a squatty potty to improve the anorectal angle are vital for reducing the back-pressure on the ileocecal junction.
##
Summary: Key Takeaways
The ileocecal valve is the "Gordian Knot" of digestive health. When it fails, the very boundaries of our internal ecosystem are breached. To move beyond the limitations of mainstream GI medicine, we must embrace a more holistic, biological understanding of this gatekeeper.
- —The ICV is a mechanical gate: It prevents colonic bacteria from colonizing the small intestine. Failure leads to SIBO and systemic inflammation.
- —Stress is a physical disruptor: Sympathetic dominance "shuts down" the Vagus nerve, leading to a loss of valve control and a "stuck open" state.
- —Environmental toxins matter: Glyphosate and emulsifiers degrade the neural and mucus-based control systems of the valve.
- —The UK faces an IBS epidemic: Much of this is likely undiagnosed ICV dysfunction and SIBO, exacerbated by a lack of specialized testing.
- —Recovery must be structural: True healing requires manual work, Vagus nerve tonification, and pressure management, not just "killing bugs."
By prioritising the integrity of the ileocecal valve, we transition from merely managing symptoms to addressing the root mechanical failure of the modern gut. The gate must be closed if the internal kingdom is to thrive.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The Ileocecal Valve: Mechanical Failure and Retrograde Colonization"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper