Methylation Defects: The MTHFR Diagnostic Gap
Common genetic variants affecting methylation are ignored by the NHS, leading to chronic health failures. We discuss the biological importance of the folate cycle in detoxification and DNA repair.
# Methylation Defects: The MTHFR Diagnostic Gap
Overview
In the landscape of modern medicine, we are witnessing a profound divergence between genomic capability and clinical application. At the heart of this chasm lies methylation—a fundamental biochemical process that occurs billions of times every second in the human body. As a senior biological researcher, it has become increasingly apparent that the Methylenetetrahydrofolate Reductase (MTHFR) genetic variant represents one of the most significant diagnostic gaps in contemporary healthcare, particularly within the National Health Service (NHS).
Despite a burgeoning body of evidence linking methylation defects to a spectrum of chronic conditions—ranging from cardiovascular disease and recurrent miscarriage to clinical depression and neurodegenerative decline—the mainstream medical establishment remains tethered to an archaic "one-size-fits-all" nutritional and genetic model. This article explores the biological intricacies of the folate cycle, the systemic failures of the current diagnostic framework, and the silent epidemic of "unexplained" chronic illness stemming from ignored genetic polymorphisms.
We are not merely discussing a "niche" genetic quirk. Estimates suggest that up to 40% to 50% of the global population carries at least one mutation of the MTHFR gene. By failing to screen for these variants or understand their implications, the medical system effectively blindfolds itself to the root cause of systemic inflammation and cellular dysfunction.
Key Statistic: Approximately 44% of the population carries one copy of the MTHFR C677T variant, which can reduce the efficiency of the folate-to-methyl-folate conversion by up to 30%. Those with two copies (homozygous) may suffer a 70% reduction in enzyme activity.
The Biology — How It Works
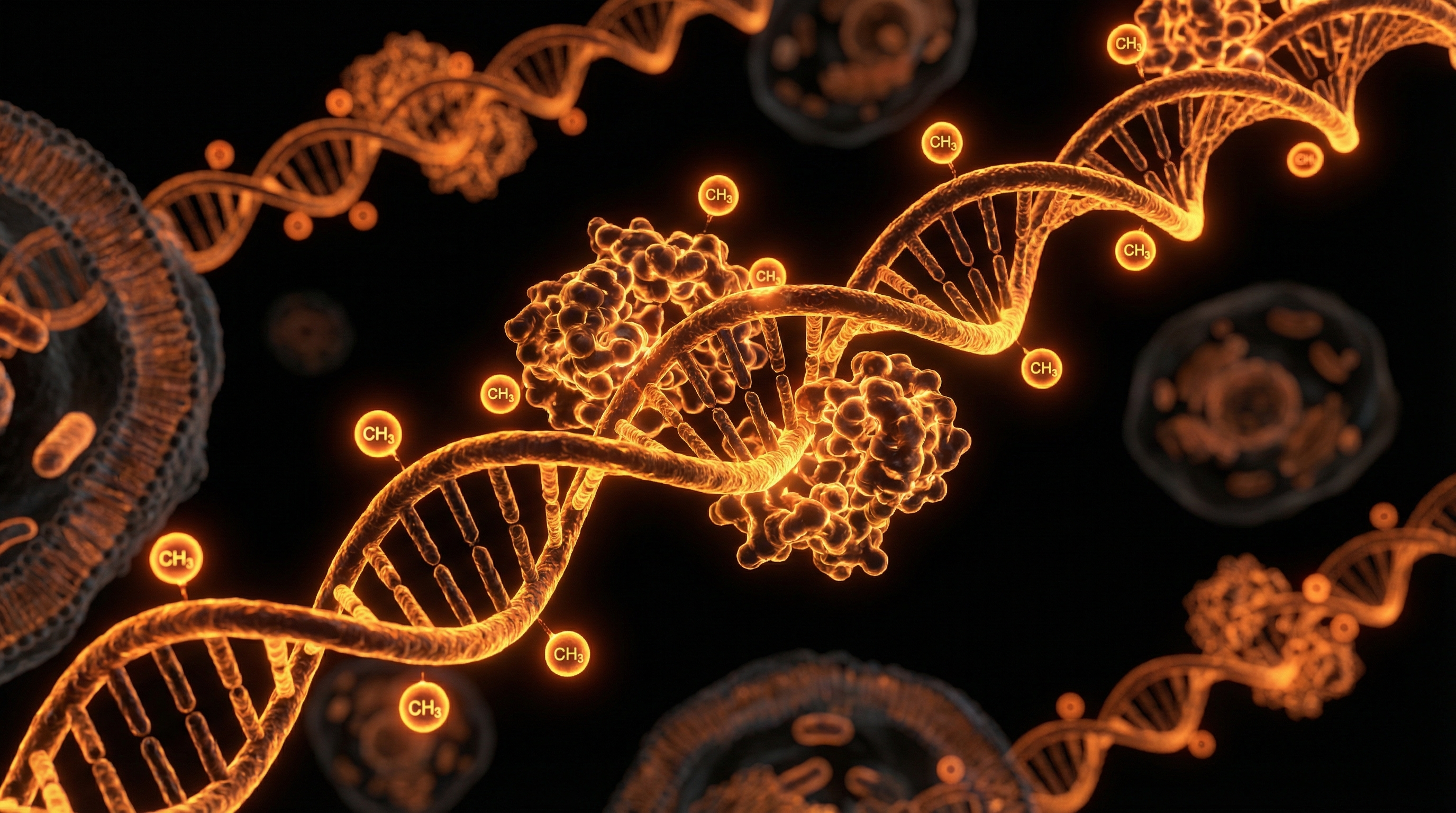
To understand the "defect," one must first understand the "engine." Methylation is essentially the donation of a methyl group (one carbon atom and three hydrogen atoms, CH3) from one molecule to another. Think of it as a universal chemical "switch" that turns genes on or off, repairs DNA, and facilitates the transport of energy.
The One-Carbon Metabolism Cycle
The process is governed by the One-Carbon Metabolism cycle, a complex gears-within-gears mechanism involving the Folate Cycle and the Methionine Cycle.
- —The Folate Cycle: This begins with the intake of dietary folates. Through a series of enzymatic conversions, folate is transformed into 5-Methyltetrahydrofolate (5-MTHF). The final, critical step in this conversion is managed by the MTHFR enzyme.
- —The Methionine Cycle: 5-MTHF then hands off its methyl group to Vitamin B12 (Cobalamin). B12, in turn, passes it to Homocysteine, converting it back into Methionine.
- —SAMe Production: Methionine is then converted into S-adenosylmethionine (SAMe), which is the body's primary universal methyl donor.
The Role of MTHFR
The MTHFR gene provides the instructions for making the MTHFR enzyme. If the gene is mutated—specifically at the C677T or A1298C positions—the enzyme's shape is slightly altered. In biochemistry, shape is function. An altered shape means the enzyme runs more slowly or breaks down prematurely.
When the MTHFR enzyme is sluggish, the entire "belt" of the assembly line slows down. The body cannot efficiently produce 5-MTHF, leading to a shortage of methyl groups. This creates a "bottleneck" where Homocysteine (a toxic amino acid) begins to accumulate in the blood, while SAMe (the fuel for DNA repair and neurotransmitters) begins to dwindle.
Mechanisms at the Cellular Level
The implications of a methylation defect are not localised; they are cellularly pervasive. If we zoom into the cell, we can observe four primary mechanisms that fail when the MTHFR diagnostic gap is ignored.
1. Epigenetic Regulation and DNA Repair
Methylation is the primary mechanism for epigenetic silencing. By attaching methyl groups to specific regions of DNA, the body "mutes" certain genes—such as those that promote cancer (oncogenes) or trigger autoimmune responses. Without adequate methylation, these "bad" genes can be "expressed" or turned on. Furthermore, the synthesis of thymidine (a building block of DNA) requires folate. A lack of methyl-folate leads to DNA strand breaks and mutations, a precursor to both aging and malignancy.
2. Neurotransmitter Synthesis and Mood
The production of Serotonin, Dopamine, Adrenaline, and Noradrenaline is heavily dependent on a co-factor called BH4 (Tetrahydrobiopterin). The recycling of BH4 is directly linked to the folate cycle.
- —A1298C Variant: This specific mutation is particularly implicated in the BH4 pathway. Defects here are frequently seen in patients with chronic anxiety, ADHD, and treatment-resistant depression.
- —COMT Interactions: Methylation also regulates the Catechol-O-methyltransferase (COMT) enzyme, which breaks down stress hormones. Poor methylators often "overheat" with adrenaline, leading to chronic "fight or flight" states.
3. Detoxification and Glutathione
One of the most critical pathways branching off the methionine cycle is the Transsulfuration Pathway. This is where the body produces Glutathione, the "Master Antioxidant."
- —When the MTHFR enzyme fails, the body struggles to convert homocysteine into cysteine, the precursor to glutathione.
- —A lack of glutathione means the body cannot effectively neutralise heavy metals, pesticides, or reactive oxygen species (ROS), leading to systemic oxidative stress.
4. Phospholipid Production and Cell Membranes
Methylation is required to produce Phosphatidylcholine, a major component of cell membranes and the myelin sheath that protects nerves. Chronic demyelinating conditions and "brain fog" are often symptoms of a failure in this specific methylation branch.
Callout: Without sufficient methyl-folate, the body is forced to choose between DNA repair and detoxification. In the hierarchy of survival, DNA repair often wins, leaving the body's toxic burden to accumulate unchecked.
Environmental Threats and Biological Disruptors
The tragedy of the MTHFR variant is not just the genetic inheritance, but how our modern environment interacts with it—a concept known as Gene-Environment Interaction (GxE).
The Folic Acid Paradox
Perhaps the most egregious failure in public health is the mandatory fortification of foods with Synthetic Folic Acid. To a healthy individual, folic acid is a cheap, stable version of folate. To an MTHFR sufferer, it is potentially toxic.
- —DHFR Saturation: Synthetic folic acid must be converted by the enzyme Dihydrofolate Reductase (DHFR). This enzyme is slow and easily saturated.
- —Unmetabolised Folic Acid (UMFA): In people with MTHFR defects, synthetic folic acid remains in the bloodstream as UMFA. UMFA can actually *block* folate receptors, preventing what little natural methyl-folate is available from entering the cells. This is known as "clogging the receptors."
Endocrine Disruptors and Heavy Metals
We live in an era of unprecedented chemical exposure. Bisphenol A (BPA), phthalates, and heavy metals like mercury and aluminium require glutathione for clearance. For those with methylation defects, their "detoxification bucket" is already full.
- —Aluminium from vaccines or cookware and mercury from dental amalgams can bind to the same sites required for B12 and folate transport, further crippling the cycle.
- —Alcohol is a potent methyl-drain; it consumes massive amounts of B-vitamins and SAMe to be processed by the liver, often leaving an MTHFR carrier depleted for days after a single drink.
Chronic Stress and Cortisol
Stress is a "methyl-sink." The production and subsequent breakdown of cortisol and adrenaline require methyl groups. In a high-stress modern environment, an MTHFR carrier "burns through" their methyl supply faster than they can replenish it, leading to the "burnout" common in chronic fatigue syndromes.
The Cascade: From Exposure to Disease
The medical establishment often treats symptoms in isolation. A patient has high blood pressure, they get an ACE inhibitor. They have depression, they get an SSRI. They have infertility, they get IVF. The MTHFR perspective reveals that these are often not separate diseases, but a cascade of failures originating from the same biochemical source.
Cardiovascular Failure
Elevated Homocysteine is an independent risk factor for heart disease, even more predictive than cholesterol in some studies. Homocysteine acts like "broken glass" in the arteries, causing micro-tears (endothelial dysfunction) that the body then tries to "patch" with cholesterol.
Fact: Research indicates that individuals with the homozygous C677T variant have significantly higher risks of stroke and venous thromboembolism due to impaired homocysteine metabolism.
The Reproductive Crisis
The NHS provides folic acid to pregnant women to prevent Neural Tube Defects (NTDs). However, if the mother has an MTHFR defect, she cannot process the folic acid, and the baby remains at risk despite the "supplementation."
- —Recurrent Miscarriage: Methylation is vital for the formation of the placenta and the prevention of micro-clots. Many women labelled with "unexplained infertility" find success only after switching to methylated folate.
- —Epigenetic Imprinting: A mother’s methylation status during pregnancy determines the "epigenetic setting" of the child's genes for life.
Mental Health and Neurodegeneration
The "Folate Trap" in the brain leads to a lack of neurotransmitter production. Because the MTHFR defect limits the conversion of folate to methyl-folate, the brain cannot produce enough SAMe to cross the blood-brain barrier. This is why many patients with depression do not respond to SSRIs; the problem isn't just serotonin reuptake, it's serotonin *production*.
What the Mainstream Narrative Omits
The refusal to integrate MTHFR screening into standard care is often defended by the mantra of "insufficient evidence for clinical utility." However, this narrative omits several critical truths.
The Pharmaceutical Bias
The current medical model is built on patentable molecules. Methyl-folate, Vitamin B12, and Magnesium are natural substances that cannot be patented. There is no financial incentive for a multi-billion-pound pharmaceutical trial to prove that a £15 bottle of methyl-folate can replace an expensive anti-psychotic or blood thinner.
The "Normal Range" Fallacy
The NHS uses "Reference Ranges" for blood tests like Folate and B12 that are based on the population average. If the population is increasingly sick and deficient, the "average" is not "optimal."
- —Serum Folate vs. Red Cell Folate: A standard serum folate test only measures what is in the blood, not what has actually entered the cells. An MTHFR sufferer might have "high" serum folate (because it's stuck in the blood, unable to be used) while being cellularly starved.
The Complexity Taboo
Modern medicine prefers binary outcomes. You either have a disease or you don't. Methylation is a spectrum of efficiency. Doctors are not trained to manage "sub-clinical" deficiencies that manifest as chronic, low-grade systemic dysfunction over decades. They are trained for acute intervention.
The UK Context
In the United Kingdom, the diagnostic gap is particularly pronounced due to the rigid nature of NICE (National Institute for Health and Care Excellence) guidelines.
The NHS Obstacle
The NHS rarely tests for MTHFR polymorphisms or homocysteine levels unless a patient has already suffered multiple miscarriages or a major thrombotic event. This is "reactive" rather than "proactive" medicine.
- —Cost-Cutting: A standard MTHFR genetic test and a homocysteine panel would cost the NHS less than £100. Compare this to the thousands spent on lifetime prescriptions for statins, antidepressants, or the astronomical cost of stroke rehabilitation and IVF.
- —GP Knowledge: Most GPs in the UK receive less than five hours of nutritional training during their entire medical degree. The concept of "biochemical individuality" via MTHFR is often dismissed as "alternative medicine" or "biohacking."
The Fortification Debate
The UK government recently moved toward mandatory folic acid fortification of flour. While intended to prevent spina bifida, this policy ignores the 15-20% of the population who are homozygous for MTHFR and may suffer adverse effects from an increased load of unmetabolised folic acid. This is a public health experiment being conducted without informed consent.
Protective Measures and Recovery Protocols
For those who suspect or have confirmed an MTHFR defect, the path to recovery involves bypassing the genetic "roadblock" through targeted nutrition and lifestyle modifications.
1. Supplementation Strategy
The goal is to provide the body with the "end-products" it cannot make for itself.
- —5-MTHF (Methyl-folate): Bypasses the MTHFR enzyme entirely. It is the bioavailable form the body can use immediately.
- —Methylcobalamin or Adenosylcobalamin: These are the active forms of B12. Avoid *Cyanocobalamin*, which contains a cyanide molecule that a poor methylator will struggle to detoxify.
- —Riboflavin (B2): Vitamin B2 is a critical co-factor for the MTHFR enzyme itself. Sometimes, high-dose B2 can "kickstart" a sluggish enzyme.
- —TMG (Trimethylglycine): Also known as Betaine, this provides an alternative pathway for the body to convert homocysteine back to methionine, bypassing the folate/B12 requirement.
2. Dietary Adjustments
- —Eliminate Folic Acid: Read labels meticulously. Avoid "fortified" cereals, breads, and pastas.
- —High Natural Folate: Consume large quantities of dark leafy greens (spinach, kale, chard), asparagus, and avocado. The word "folate" comes from "foliage."
- —Cruciferous Vegetables: Broccoli and Brussels sprouts contain sulforaphane, which supports the transsulfuration pathway and glutathione production.
3. Lifestyle and Detoxification
- —Support the Liver: Use milk thistle, dandelion root, and castor oil packs to assist a liver that may be struggling with its toxic load.
- —Sauna Therapy: Sweating is a secondary pathway for excreting heavy metals, taking the pressure off the compromised methylation system.
- —Hydration and Electrolytes: Methylation requires adequate cellular hydration. Focus on filtered water with added trace minerals to avoid fluoride, which can interfere with enzyme function.
4. Testing
Since the NHS is unlikely to provide these tests, private functional testing is often necessary.
- —Genetic Testing: Services like 23andMe or AncestryDNA (raw data processed through specialised tools like Strategene or Genetic Genie).
- —Homocysteine Panel: Aim for a level between 5 and 7 umol/L. The NHS "normal" range often goes up to 15, which many researchers consider far too high.
- —Organic Acids Test (OAT): This can provide a snapshot of how your methylation is actually performing in real-time by looking at metabolic byproducts in the urine.
Summary: Key Takeaways
The MTHFR diagnostic gap is a testament to the limitations of a medical system that prioritises protocols over people. By ignoring the fundamental biology of methylation, we are allowing millions to languish in a state of avoidable chronic illness.
- —Methylation is Fundamental: It controls DNA repair, neurotransmitter production, hormone balance, and detoxification.
- —The MTHFR Variant is Common: It is a high-prevalence polymorphism, not a rare disease.
- —Folic Acid is Not Folate: For those with the defect, synthetic folic acid can block receptors and cause toxicity, yet it is mandated in our food supply.
- —The NHS is Lagging: UK health protocols focus on reactive care rather than the biochemical prevention that MTHFR screening allows.
- —Knowledge is Power: Identifying your methylation status allows for simple, inexpensive interventions (like methyl-folate and B12) that can radically alter your health trajectory.
The "MTHFR Diagnostic Gap" is more than a scientific oversight; it is a call to action for a more nuanced, personalised approach to human health. We must move beyond the era of the "average patient" and embrace the reality of our biochemical individuality. The tools for recovery exist; it is only the mainstream narrative that remains broken.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Methylation Defects: The MTHFR Diagnostic Gap"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper