PPI Dependency: Analyzing the MHRA Evidence on Gastric Acid Suppression
The MHRA has issued warnings regarding long-term PPI use, yet these drugs remain among the most prescribed in the UK. Persistent acid suppression disrupts the pH gradient of the small intestine, inviting distal bacteria to migrate upward.
Overview
The modern pharmaceutical landscape is defined by the ubiquity of the "quick fix," yet few interventions have permeated the global collective consciousness—and the human gastrointestinal tract—quite as thoroughly as Proton Pump Inhibitors (PPIs). Marketed as the ultimate solution for gastroesophageal reflux disease (GERD), peptic ulcers, and general "heartburn," PPIs such as Omeprazole, Lansoprazole, and Esomeprazole have transitioned from strictly controlled clinical tools to over-the-counter staples. However, beneath the veneer of symptomatic relief lies a mounting body of evidence suggesting that chronic gastric acid suppression is not merely a benign intervention, but a fundamental disruption of human physiology.
The Medicines and Healthcare products Regulatory Agency (MHRA) in the United Kingdom has, over the last decade, issued increasingly urgent communications regarding the long-term systemic risks of these drugs. From bone fractures and hypomagnesemia to the increased risk of *Clostridium difficile* infections, the regulatory warnings are clear. Yet, despite these red flags, the prescription rates within the NHS remain staggering. We are witnessing a paradox: a pharmaceutical dependency sanctioned by a medical system that acknowledges the risks but struggles to provide an exit strategy.
This article serves as a deep-dive analysis into the biological catastrophe of long-term PPI use. We will explore how the suppression of hydrochloric acid (HCl)—a substance the body spends significant metabolic energy to produce—dismantles the primary immunological barrier of the gut. By flattening the pH gradient of the small intestine, PPIs do not just stop "acid reflux"; they invite a systemic invasion of distal bacteria into the proximal gut, setting the stage for Small Intestinal Bacterial Overgrowth (SIBO), malabsorption, and chronic inflammatory states.
UK Statistics Alert: In 2022/23, more than 65 million prescriptions for PPIs were dispensed in England alone, a figure that has risen steadily despite MHRA safety alerts regarding long-term dependency and adverse effects.
##
The Biology — How It Works
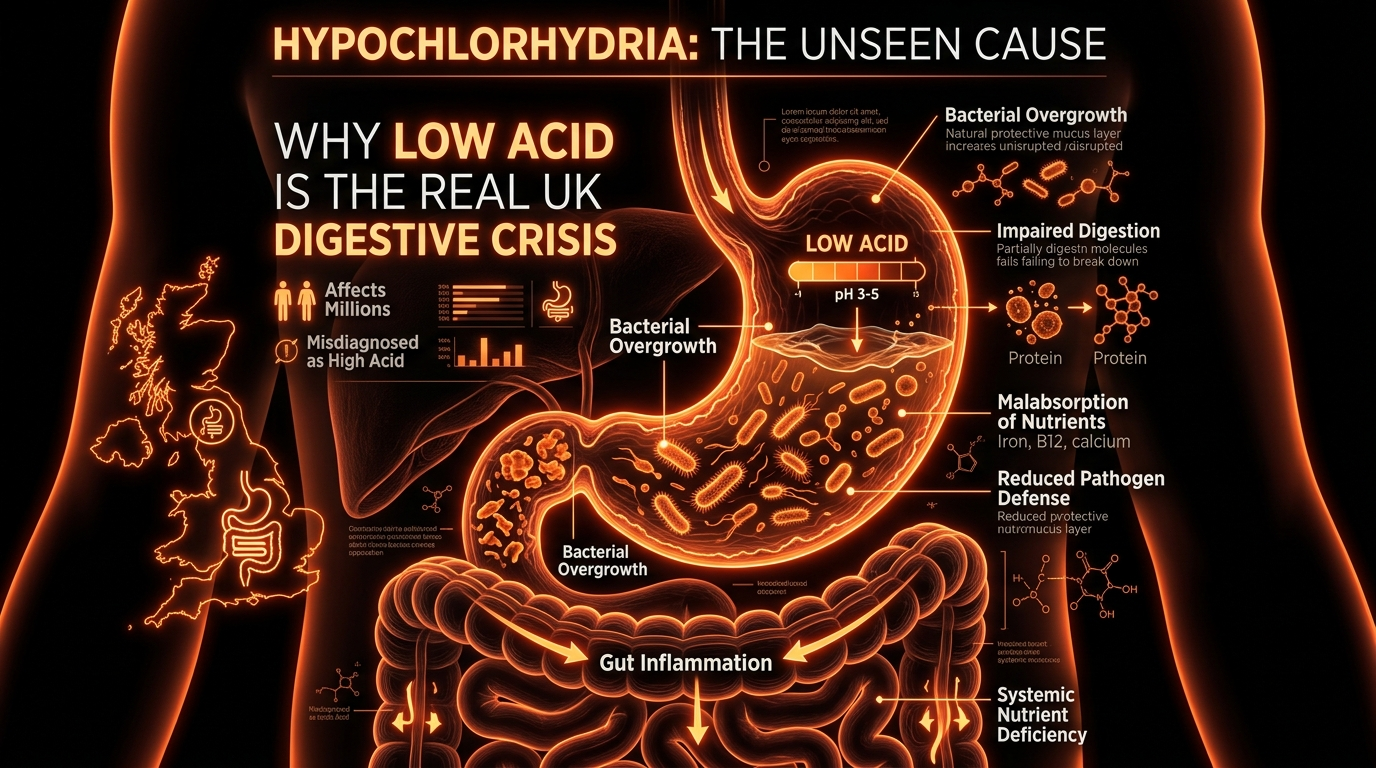
To understand the danger of PPI dependency, one must first appreciate the elegance and necessity of gastric acidity. The human stomach is an evolutionary marvel designed to operate at an incredibly low pH, typically between 1.5 and 3.5. This extreme acidity serves two primary, non-negotiable functions: the denaturation of dietary proteins and the sterilisation of ingested pathogens.
The Role of Hydrochloric Acid (HCl)
The secretion of HCl is managed by the parietal cells (also known as oxyntic cells) located in the gastric mucosa. When we see, smell, or taste food, the vagus nerve and hormonal signals (such as gastrin) stimulate these cells to pump hydrogen ions ($H^+$) into the stomach lumen in exchange for potassium ions ($K^+$). This is the "Proton Pump" mechanism.
The resulting acidic environment is the catalyst for digestion. It activates pepsinogen into pepsin, the enzyme responsible for breaking down proteins into peptides. Without sufficient acid, the enzymatic cascade of digestion is halted at the very first gate. Furthermore, this acidic "bath" ensures that the thousands of bacteria, viruses, and fungal spores we ingest with every meal are neutralised before they reach the delicate environment of the small intestine.
The pH Gradient: The Body’s Internal Border Force
The gastrointestinal tract is not a uniform tube; it is a series of compartmentalised chambers, each with a specific pH requirement. The stomach is highly acidic (pH 1.5–3), the duodenum is slightly alkaline (pH 6–7) to neutralise the chyme, and the distal small intestine and colon maintain a more neutral to slightly acidic profile (pH 6–7.5).
This sharp transition from the extreme acidity of the stomach to the near-neutrality of the duodenum acts as a "chemical firewall." This gradient prevents the trillions of bacteria residing in the large intestine from migrating upwards into the small intestine, where they would otherwise compete for nutrients and cause inflammatory damage. When PPIs are introduced, they don't just "lower" acid; they can raise gastric pH to 5 or 6—effectively dismantling the firewall and turning the entire upper GI tract into a hospitable environment for microbial colonisation.
##
Mechanisms at the Cellular Level
Proton Pump Inhibitors are classified as "prodrugs." They are ingested in an inactive form, designed to survive the stomach's acidity (usually via an enteric coating) and be absorbed in the small intestine. From the bloodstream, they travel back to the parietal cells of the stomach.
Irreversible Inhibition
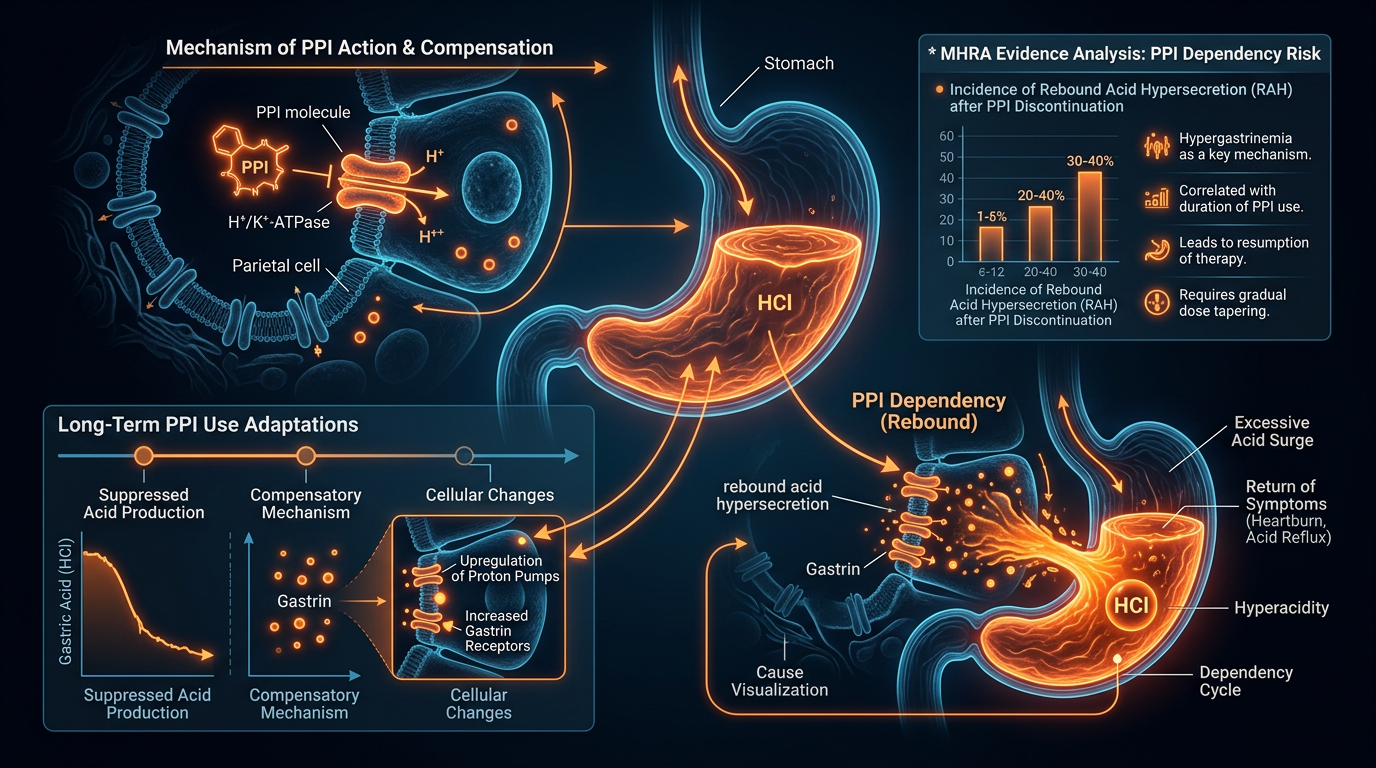
Once inside the acidic environment of the parietal cell’s secretory canaliculi, the PPI is converted into its active form, a sulfenamide. This active metabolite forms a covalent, irreversible bond with the $H^+/K^+$-ATPase enzyme—the proton pump itself. Because the bond is covalent, the "pump" is permanently deactivated. The only way the body can resume acid production is by synthesising entirely new enzymes, a process that takes roughly 24 to 48 hours.
This irreversible nature is why PPIs are so effective, but it is also why they are so dangerous. By shutting down the primary mechanism of acid production at the source, they create a state of "achlorhydria" or "hypochlorhydria" (zero or low stomach acid) that is far more profound and long-lasting than the effects of older drugs like $H_2$ antagonists (e.g., Ranitidine).
The Hypergastrinemia Feedback Loop
The body is not a passive recipient of drug intervention; it possesses sophisticated feedback loops. When the stomach’s internal "pH sensor" detects that acidity has dropped, it signals the G-cells in the antrum of the stomach to secrete massive amounts of gastrin. Gastrin is a hormone designed to stimulate the parietal cells to produce more acid.
However, because the PPI has physically "locked" the proton pumps, the acid never comes. This leads to a state of chronic hypergastrinemia. High levels of gastrin act as a growth factor, causing hyperplasia (overgrowth) of the parietal cells and enterochromaffin-like (ECL) cells. This cellular remodeling is a key driver of PPI Dependency. When a patient attempts to stop the drug, these "primed" and overgrown cells suddenly unleash a massive, dysregulated flood of acid—far more than the person had before starting the medication. This is known as "Rebound Acid Hypersecretion," and it often forces the patient back onto the drug, creating a cycle of lifelong dependency.
##
Environmental Threats and Biological Disruptors
The gut is our primary interface with the external environment. Every day, we consume billions of microbes. In a healthy system, the "gastric fire" of HCl ensures that only the intended nutrients pass through, while the microbial load is incinerated. Long-term PPI use extinguishes this fire, leaving the gates wide open.
The Loss of Luminal Sterility
In the absence of gastric acid, the upper gastrointestinal tract loses its sterility. Research has shown that PPI users have a significantly altered oral and gastric microbiome. Bacteria that are usually confined to the mouth—such as *Streptococcus* and *Staphylococcus*—are found thriving in the stomachs of PPI users.
This lack of sterility is not a minor inconvenience; it is an environmental threat. Without the acid barrier, the risk of foodborne illnesses like *Salmonella* and *Campylobacter* increases significantly. The MHRA has specifically warned about the increased risk of *Clostridium difficile* (C. diff) infections. C. diff is a devastating bacterium that causes severe diarrhoea and colitis; it thrives when the protective "acid barrier" is removed and the commensal microbiome is disrupted.
Environmental Toxins and Undigested Proteins
Furthermore, the lack of acid prevents the proper breakdown of environmental toxins and complex proteins. When large, undigested protein sequences enter the small intestine, they can trigger immune responses. This "molecular mimicry" or general immune activation contributes to the development of food sensitivities and systemic inflammation. The PPI user is not just poorly digesting their food; they are effectively poisoning their internal environment with improperly processed biological material.
MHRA Safety Alert: Since 2012, the MHRA has warned that PPIs may increase the risk of fractures, particularly when used at high doses for over a year in elderly patients. This is due to the acid-dependent nature of calcium and magnesium absorption.
##
The Cascade: From Exposure to Disease
The disruption of the stomach does not stay in the stomach. It triggers a physiological cascade that ripples through the entire digestive system, eventually manifesting as systemic disease.
The SIBO Connection
Small Intestinal Bacterial Overgrowth (SIBO) is perhaps the most direct consequence of chronic acid suppression. The small intestine is designed to be relatively low in bacterial count. When the gastric pH rises, and the "acid gate" fails, distal bacteria from the colon and proximal bacteria from the mouth begin to colonise the small intestine.
Once established in the small intestine, these bacteria:
- —Ferment carbohydrates prematurely, leading to bloating, gas, and pain.
- —Deconjugate bile acids, leading to the malabsorption of fats and fat-soluble vitamins (A, D, E, K).
- —Damage the microvilli, the tiny projections on the intestinal wall responsible for nutrient absorption.
- —Consume B12 and Iron, leaving the host (the human) deficient even if their diet is adequate.
This migration of bacteria turns the small intestine into a site of fermentation rather than absorption, leading to the hallmark symptoms of "IBS" which are, in many cases, actually undiagnosed SIBO caused by PPI use.
The Nutrient Malabsorption Crisis
The chemical environment of the stomach dictates the bioavailability of almost every essential mineral.
- —Vitamin B12: Requires gastric acid and pepsin to be released from food proteins, and then requires "Intrinsic Factor" (also produced by parietal cells) to be absorbed. PPIs hit both ends of this process.
- —Magnesium: The MHRA issued a "Yellow Card" warning in 2012 regarding severe hypomagnesemia in long-term PPI users. Low magnesium can lead to fatigue, muscle cramps, and life-threatening cardiac arrhythmias.
- —Calcium: Calcium carbonate requires an acidic environment to become ionised and soluble. Long-term PPI use is directly correlated with reduced bone mineral density and an increased risk of hip, wrist, and spine fractures.
- —Iron: Non-heme iron (from plant sources) requires acid for optimal absorption. PPI users frequently present with recalcitrant iron-deficiency anaemia.
##
What the Mainstream Narrative Omits
The current medical narrative surrounding PPIs is one of "safety by default." Because these drugs have been on the market for decades, they are often perceived as harmless. However, there are critical biological truths that are frequently omitted from patient consultations and even some clinical guidelines.
The "Aspirin of the Gut" Fallacy
PPIs are often prescribed as "prophylaxis" for patients taking NSAIDs (like Ibuprofen) or Aspirin. While they can prevent gastric erosions, they do nothing to address the damage NSAIDs cause further down in the small intestine. In fact, by inducing SIBO and altering the microbiome, PPIs may actually *exacerbate* the intestinal damage caused by other medications. They are not "stomach protectors"; they are "acid eliminators" with systemic consequences.
The Psychological Component of Dependency
There is a profound "rebound" effect that is rarely explained to patients. When a person tries to stop their 20mg Omeprazole, they experience a massive surge of acid. They interpret this as "my reflux is back" or "I still need the drug," when in reality, it is a drug-induced physiological withdrawal. The medical system frequently misinterprets this withdrawal as a continuation of the original disease, leading to a lifetime of unnecessary prescription.
The Mitochondrial Connection
Emerging research suggests that PPIs may not be as specific to the stomach as once thought. Some studies indicate that PPIs can inhibit proton pumps in other parts of the body, including the lysosomes within our cells. Lysosomes are the "recycling centres" of the cell; they require an acidic environment to clear out cellular waste. By potentially alkalising these lysosomes, PPIs could be contributing to accelerated cellular ageing and the accumulation of damaged proteins, a factor in neurodegenerative and vascular diseases. This is a far cry from the "localised action" promised by pharmaceutical marketing.
##
The UK Context
The United Kingdom presents a unique case study in PPI over-utilisation. Within the NHS, the "Polypharmacy" crisis is in full swing, with many elderly patients taking ten or more medications simultaneously. PPIs are almost always part of this cocktail.
The MHRA Evidence
The MHRA has been diligent in tracking the safety profile of PPIs, yet the translation of these warnings into clinical practice is slow.
- —2008: Warnings regarding the risk of *C. difficile*.
- —2012: Warnings regarding severe hypomagnesemia.
- —2015: Warnings regarding Subacute Cutaneous Lupus Erythematosus (SCLE).
- —Recent: Potential links to acute kidney injury and chronic kidney disease.
The "Yellow Card" system in the UK has accumulated thousands of reports of adverse reactions, yet PPIs remain the first-line treatment for even minor indigestion. There is a systemic reluctance to utilise more nuanced approaches, such as addressing the "Lower Oesophageal Sphincter" (LOS) function, hiatal hernias, or dietary triggers.
The Cost of Convenience
The NHS spends hundreds of millions of pounds annually on PPI prescriptions and the subsequent treatment of their side effects (e.g., fracture repairs, B12 injections, and C. diff treatments). A shift toward "Deprescribing" is beginning to take hold in some Clinical Commissioning Groups (CCGs), but the sheer volume of patients "hooked" on these drugs makes it a daunting task for the average GP.
##
Protective Measures and Recovery Protocols
If you or a patient are caught in the cycle of PPI dependency, the path to recovery is not as simple as stopping cold turkey. Because of the "rebound effect" mentioned earlier, a strategic, biological approach is required to restore the pH gradient and heal the gut.
1. The Gradual Taper
The most critical step in avoiding rebound hyperacidity is a very slow taper. This allows the overgrown parietal and ECL cells to atrophy back to their normal size and density.
- —Step-down therapy: Switching from a PPI to a weaker $H_2$ antagonist (like Famotidine) can provide a "bridge" while the proton pumps begin to function again.
- —Dose reduction: Reducing the dose by 50% every two weeks, or moving to every-other-day dosing, is often more successful than abrupt cessation.
2. Restoring the Acid Gate
Paradoxically, many people with "acid reflux" actually have *too little* stomach acid, not too much. Low acid leads to poor digestion, which leads to gas and pressure that forces the Lower Oesophageal Sphincter open, allowing what little acid is there to splash up.
- —Betaine HCl with Pepsin: Under professional supervision, supplementing with HCl can help "reset" the stomach's pH. This should never be done while on PPIs or if an active ulcer is present.
- —Apple Cider Vinegar/Lemon Water: For mild cases, acidic tonics before meals can assist in the digestive process.
3. Healing the Mucosa
Before reintroducing acid, the stomach lining must be resilient.
- —Deglycyrrhizinated Licorice (DGL): Helps support the mucus lining of the stomach.
- —Zinc Carnosine: A potent compound shown to heal gastric erosions and support the mucosal barrier.
- —Slippery Elm/Marshmallow Root: Provide a soothing, mucilaginous layer to protect the oesophagus during the tapering phase.
4. Addressing SIBO and Dysbiosis
Once the "acid fire" is back online, the "weeds" in the small intestine need to be addressed.
- —Prokinetics: Substances that encourage the Migrating Motor Complex (MMC) to "sweep" the small intestine. This can include ginger, triphala, or low-dose pharmaceutical prokinetics.
- —Antimicrobial Herbs: If SIBO is present, a course of Oregano oil, Berberine, or Allicin may be necessary to clear the bacterial overgrowth that the PPIs invited in.
5. Lifestyle and Mechanical Factors
- —Circadian Rhythm: Acid production follows a circadian rhythm. Eating large meals late at night when acid production is naturally lower is a recipe for reflux.
- —The Diaphragm: The diaphragm acts as a physical support for the LOS. Diaphragmatic breathing exercises can strengthen this "external sphincter" and reduce reflux without the need for drugs.
##
Summary: Key Takeaways
The evidence provided by the MHRA and the broader biological community is unequivocal: Proton Pump Inhibitors are high-potency drugs that carry significant systemic risks when used beyond their intended short-term window (usually 4–8 weeks).
- —The Acid Fallacy: Gastric acid is not a "waste product" or a mistake of evolution; it is a vital biological filter and digestive catalyst.
- —SIBO Risk: By raising gastric pH, PPIs dismantle the body's primary defense against SIBO and distal bacterial migration.
- —Nutritional Depletion: Long-term use inevitably leads to deficiencies in B12, Magnesium, Calcium, and Iron, contributing to osteoporosis and cardiovascular issues.
- —The Dependency Trap: Rebound acid hypersecretion makes it physically difficult to stop PPIs, creating a cycle of permanent pharmaceutical reliance.
- —UK Crisis: The NHS is facing a tidal wave of PPI-related complications, requiring a radical shift toward deprescribing and root-cause GI health.
True healing of the small intestine and the restoration of systemic health cannot occur in an alkaline stomach. We must respect the pH gradient of the human body and recognise that while PPIs may offer a temporary reprieve from the "burn," the long-term biological cost is a price too high to pay. It is time to relight the gastric fire and restore the integrity of the human microbiome.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "PPI Dependency: Analyzing the MHRA Evidence on Gastric Acid Suppression"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper