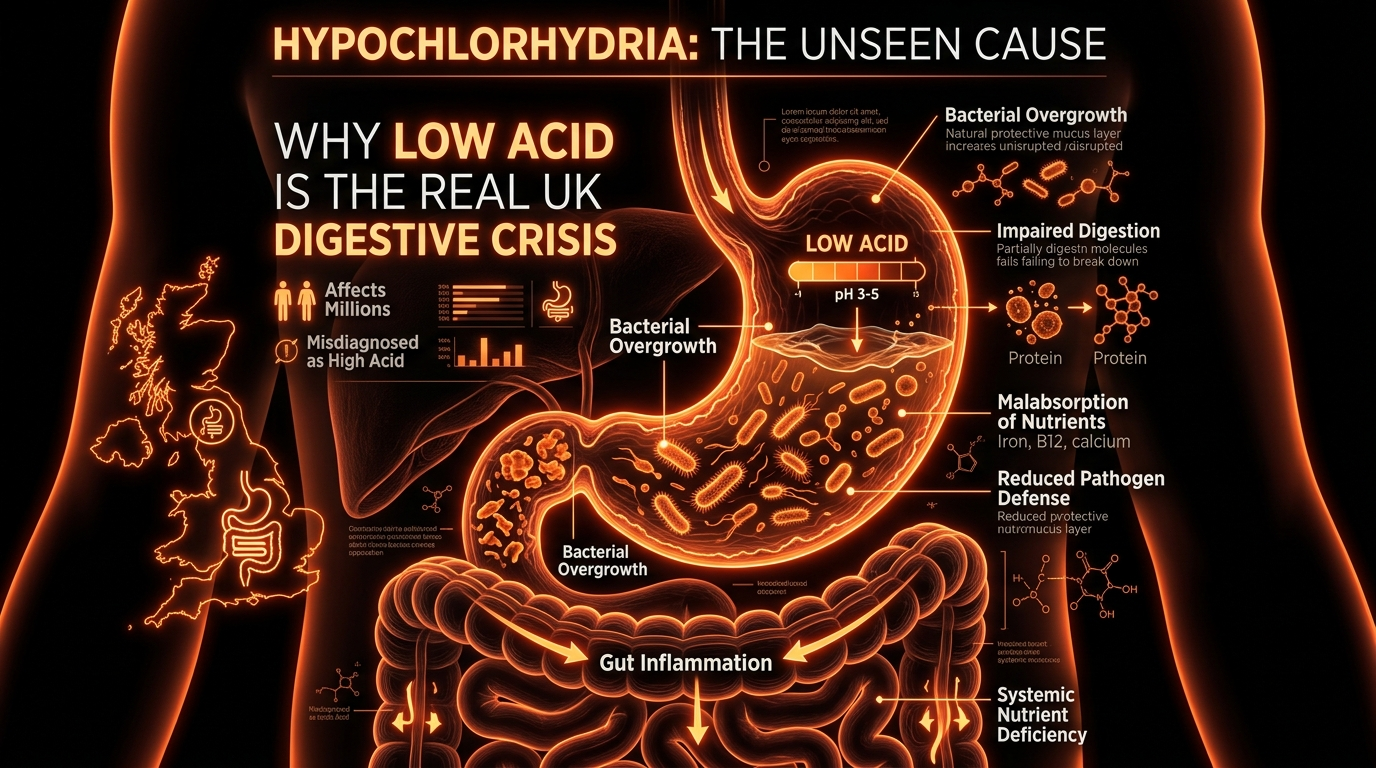
Hypochlorhydria: Why Low Acid is the Real UK Digestive Crisis
Stomach acid acts as a primary chemical barrier against bacterial ingestion; without it, the small intestine remains vulnerable to colonization. We expose why the widespread use of PPIs in the NHS may be fueling a quiet epidemic of overgrowth.
Overview
In the halls of British medicine, a quiet but devastating oversight has taken root. For decades, the primary narrative surrounding digestive distress has been one of excess: too much acid, too much heat, too much "heartburn." The solution, ubiquitous across the National Health Service (NHS), has been the aggressive suppression of gastric acid through Proton Pump Inhibitors (PPIs) and H2 antagonists. However, as a biological researcher, I must present the stark, uncomfortable reality: the UK is not suffering from an epidemic of hyperchlorhydria (excess acid), but rather a systemic crisis of hypochlorhydria—a pathological deficiency of stomach acid.
Stomach acid, specifically hydrochloric acid (HCl), is the primary chemical sentinel of the human body. It is the first line of defence in the innate immune system, designed to sterilise every bolus of food that passes the lips. When this barrier is compromised, the entire downstream architecture of the gastrointestinal tract begins to fail. We are currently witnessing a surge in Small Intestinal Bacterial Overgrowth (SIBO), chronic malabsorption, and autoimmune triggers that can be traced directly back to a failure of the gastric furnace.
This article serves as a comprehensive exposé on the physiological necessity of low-pH gastric juice and the biological catastrophe that ensues when we chemically silence it. In the context of the UK’s current health landscape, where digestive "maintenance" drugs are handed out like confectionery, understanding the mechanisms of hypochlorhydria is no longer just a clinical interest—it is a public health necessity.
UK STATISTIC: In 2022/23, the NHS in England alone issued over 64 million prescriptions for Proton Pump Inhibitors (PPIs), a figure that has risen steadily for two decades, despite growing evidence linking long-term use to increased mortality and systemic infection.
##
The Biology — How It Works
To understand the crisis, one must first appreciate the elegance of the gastric environment. The human stomach is an evolutionary anomaly. While most of our internal fluids maintain a near-neutral pH (around 7.4), the stomach aim for a pH of 1.5 to 3.0. This represents a concentration of hydrogen ions that is nearly a million times higher than that of the blood.
The Phases of Acid Secretion
Digestion is a choreographed event occurring in three distinct phases:
- —The Cephalic Phase: Before food even enters the mouth, the vagus nerve stimulates the stomach based on the sight, smell, or thought of food. This accounts for roughly 30% of total acid production.
- —The Gastric Phase: Once food enters the stomach, distension and the presence of amino acids trigger the release of gastrin, further amping up acid production.
- —The Intestinal Phase: As the acidic chyme moves into the duodenum, feedback loops begin to downregulate acid to protect the small intestine.
The Role of Hydrochloric Acid (HCl)
The primary role of HCl is not, as commonly believed, the complete breakdown of food. Its roles are more nuanced and vital:
- —Protein Denaturation: HCl "unfolds" complex protein structures, exposing their peptide bonds to digestive enzymes.
- —Enzymatic Activation: It converts inactive pepsinogen into the active enzyme pepsin, which is the only substance capable of breaking down collagen and tough connective tissues.
- —Mineral Ionisation: Essential minerals like iron, calcium, magnesium, and zinc are bound to other molecules in food. Only a highly acidic environment can "liberate" these ions so they can be absorbed in the duodenum.
- —The Sterile Barrier: Most pathogenic bacteria, fungi, and parasites cannot survive a pH below 3.0. This ensures that the small intestine—an organ designed for absorption, not defence—remains relatively sterile.
When the pH rises above 4.0, these functions cease. The protein remains putrefied rather than digested, minerals stay locked in their food matrices, and the "gate" to the small intestine is left wide open for microbial invaders.
##
Mechanisms at the Cellular Level
At the heart of the hypochlorhydria crisis are the parietal cells. Located within the gastric pits of the stomach lining, these cells are among the most energy-intensive in the human body. To produce an environment as acidic as a car battery, they must pump hydrogen ions against an incredible concentration gradient.
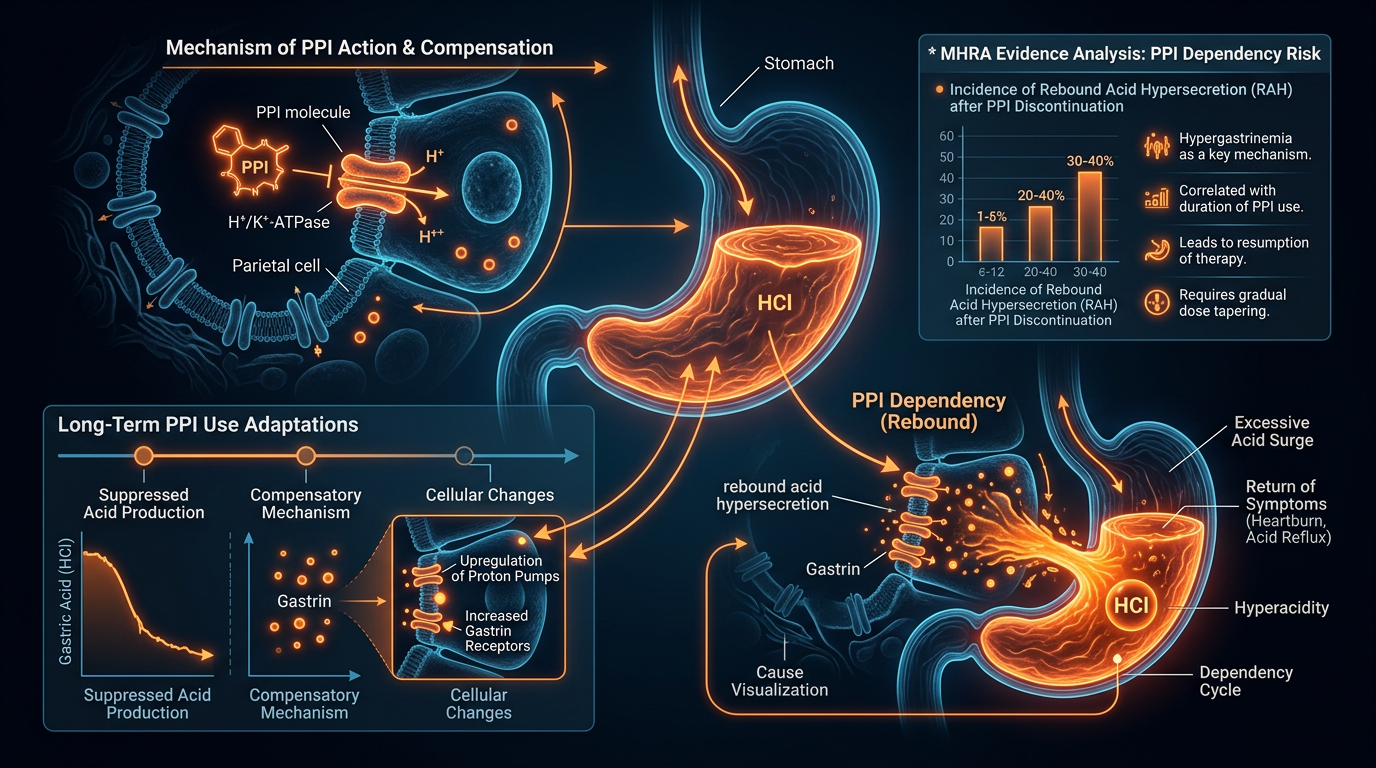
The Proton Pump (H+/K+ ATPase)
The actual mechanism of acid secretion is the H+/K+ ATPase enzyme, commonly known as the "proton pump." This pump exchanges potassium ions from the stomach lumen for hydrogen ions from inside the cell. This process requires massive amounts of Adenosine Triphosphate (ATP), which is why parietal cells are packed with mitochondria.
The Bicarbonate Shift
For every molecule of hydrochloric acid pumped into the stomach, a molecule of bicarbonate is secreted into the bloodstream. This is known as the "alkaline tide." This shift is crucial for maintaining the body's systemic pH balance and ensuring that the pancreas is "signalled" to prepare its own bicarbonate-rich juices to neutralise the acid later in the duodenum.
The Intrinsic Factor
Parietal cells are also the sole source of Intrinsic Factor (IF), a glycoprotein essential for the absorption of Vitamin B12. In cases of chronic hypochlorhydria, whether caused by autoimmune gastritis (Pernicious Anaemia) or PPI use, IF production is often compromised. This leads to a slow, insidious decline in neurological health and red blood cell production, as B12 levels crater.
ALARMING FACT: A stomach with a pH of 5.0—often the goal of PPI therapy—has 1,000 times fewer hydrogen ions than a healthy stomach at pH 2.0. This effectively turns a primary immune barrier into a welcoming reservoir for pathogens.
##
Environmental Threats and Biological Disruptors
The modern Briton lives in an environment that is functionally designed to suppress stomach acid. While PPIs are the most visible culprit, the biological disruption is multi-faceted.
The PPI Epidemic
Proton Pump Inhibitors (Omeprazole, Lansoprazole, Esomeprazole) work by irreversibly binding to the H+/K+ ATPase pump. Once a pump is "switched off" by these drugs, it never switches back on; the cell must produce an entirely new pump to resume acid production. While these drugs were originally designed for short-term use (4-8 weeks) to heal active ulcers, millions of people in the UK have been taking them for years, or even decades. This results in "achlorhydria"—a near-total absence of stomach acid.
Chronic Stress and the Vagus Nerve
The "fight or flight" response is the antithesis of digestion. Chronic sympathetic nervous system activation diverts blood flow away from the digestive tract and inhibits the vagus nerve. Since the vagus nerve is the primary "on" switch for parietal cells, a population living in a state of constant cortisol-driven stress is a population that cannot produce adequate HCl.
H. pylori: The Great Manipulator
*Helicobacter pylori* is a bacterium that has evolved specifically to survive the stomach. It does so by secreting an enzyme called urease, which converts urea into ammonia. This creates a "neutralising cloud" of alkalinity around the bacteria, shielding it from acid. Over time, *H. pylori* can cause chronic inflammation (gastritis) that actually destroys the parietal cells, leading to permanent hypochlorhydria and an increased risk of gastric cancer.
The Ageing Factor
It was once thought that low stomach acid was a natural consequence of ageing. We now understand that this is more likely the result of cumulative damage to the gastric mucosa. However, the data remains clear: by age 60, an estimated 30-40% of the population suffers from some degree of atrophic gastritis or hypochlorhydria, making the elderly particularly vulnerable to the nutrient deficiencies and infections that follow.
##
The Cascade: From Exposure to Disease
Hypochlorhydria is not a localised "stomach problem." It is the first domino in a systemic collapse of the digestive and immune systems. When the gastric barrier fails, a predictable sequence of pathological events—the "cascade"—is triggered.
SIBO: The Upward Migration
The small intestine is supposed to be relatively sparsely populated by bacteria (less than $10^3$ organisms per ml). The primary mechanisms keeping it this way are the Migrating Motor Complex (the "inter-meal sweep") and the acidic bath of chyme coming from the stomach. In the absence of HCl, bacteria ingested with food or migrating upward from the colon are allowed to colonise the small intestine. This is Small Intestinal Bacterial Overgrowth (SIBO). These bacteria begin to ferment carbohydrates in the "wrong" place, producing gases (hydrogen and methane) that cause bloating, pain, and the very reflux symptoms that often lead to *more* acid-suppressing prescriptions.
The Proteolysis Failure
Without active pepsin (which requires low pH), proteins are not broken down into their constituent amino acids. Instead, they remain as large, immunogenic peptides. When these undigested proteins reach the small intestine, they irritate the delicate mucosal lining and contribute to intestinal permeability ("Leaky Gut"). This allows foreign protein fragments to enter the bloodstream, triggering systemic inflammation and potentially autoimmune cross-reactivity.
Micronutrient Starvation
The UK is seeing a resurgence in "sub-clinical" malnutrition despite high caloric intake.
- —Iron: HCl is required to convert ferric iron ($Fe^{3+}$) to the more absorbable ferrous iron ($Fe^{2+}$).
- —Magnesium: Required for over 300 biochemical reactions; its absorption is highly pH-dependent.
- —Vitamin B12: As mentioned, the failure of Intrinsic Factor and the inability to cleave B12 from animal proteins leads to profound deficiency.
CRITICAL BIOLOGY: Low stomach acid creates a "vicious cycle." To produce acid, parietal cells need zinc and B3. If acid is low, you cannot absorb zinc or B3, making it impossible for the body to restore acid production on its own.
##
What the Mainstream Narrative Omits
The mainstream medical approach in the UK, largely dictated by NICE (National Institute for Health and Care Excellence) guidelines, tends to treat symptoms as the disease itself. Heartburn and GERD (Gastro-oesophageal Reflux Disease) are treated as "too much acid," when in reality, they are often symptoms of acid in the wrong place.
The Sphincter Paradox
The Lower Oesophageal Sphincter (LOS) is the valve that keeps stomach contents out of the oesophagus. This valve is pH-sensitive. Paradoxically, it is the *presence* of high acidity in the stomach that signals the LOS to close tightly. When stomach acid is low, the LOS remains "floppy." This allows even a small amount of weak acid to splash up into the oesophagus, causing the burning sensation we call heartburn. By giving PPIs, we make the reflux less "burny" by reducing its acidity, but we worsen the underlying cause—the failure of the sphincter to close due to a lack of acidic stimulus.
The "Silent" Epidemic of Fermentation
The mainstream narrative almost entirely ignores the role of intra-abdominal pressure (IAP). When low acid leads to bacterial fermentation in the small intestine, the resulting gas creates upward pressure on the stomach. This pressure physically forces the (already weak) LOS open. Thus, reflux is often a "pressure problem" caused by "low acid" and "bacterial overgrowth," rather than a "production problem" of having too much acid.
The Financial Incentive of Suppression
PPIs are among the most profitable drugs in history. For the NHS, they are a cheap "fix" for a complex problem. Reversing hypochlorhydria requires intensive nutritional support, lifestyle changes, and often expensive diagnostic testing for SIBO and microbiome health. It is far more "cost-effective" in the short term to suppress the symptom than to rebuild the gastric barrier.
##
The UK Context
The United Kingdom presents a unique "perfect storm" for hypochlorhydria. Our lifestyle and dietary patterns, combined with the structural limitations of the NHS, have created a crisis that is often overlooked in comparison to obesity or heart disease.
The "Beige Diet" and Alcohol Culture
The traditional British diet—high in refined carbohydrates, processed "beige" foods, and low in bitter, stimulatory vegetables—fails to provide the chemical signals necessary for healthy acid production. Furthermore, the UK’s relationship with alcohol is a major factor. While acute alcohol consumption can increase acid, chronic heavy drinking leads to the thinning of the stomach lining and the destruction of parietal cells (atrophic gastritis).
The "Stiff Upper Lip" and Chronic Stress
British culture often prides itself on "soldiering on." This chronic, low-level psychosocial stress keeps the population in a state of sympathetic dominance. As we have explored, you cannot "rest and digest" while you are "fighting or flighting." The result is a nation of people eating on the go, under stress, with inhibited vagal tone and suppressed gastric function.
NHS Resource Constraints
The 10-minute GP consultation is the enemy of digestive health. Diagnosing hypochlorhydria requires a detailed history and, ideally, a Heidelberg pH test (where a patient swallows a pH-sensing capsule). These tests are almost never performed on the NHS. Instead, "Dyspepsia" is the catch-all diagnosis, and PPIs are the catch-all "solution." The "rebound effect"—where stopping PPIs causes a temporary, painful spike in acid—often misleads both patient and doctor into thinking the drugs are "necessary" for life, further entrenching the dependency.
##
Protective Measures and Recovery Protocols
Restoring the gastric barrier is a delicate process that requires moving against the grain of conventional advice. It is not about "neutralising" but about "optimising."
1. The Restoration of Vagal Tone
Before a single supplement is taken, the nervous system must be addressed.
- —Mindful Eating: Simply sitting down and smelling the food before eating can increase cephalic phase acid production by 30%.
- —Vagus Nerve Stimulation: Exercises such as gargling, loud singing, or cold-water exposure can help "reset" the vagal signal to the stomach.
2. Bitter Stimulants
The tongue has bitter receptors that, when activated, trigger a cascade of digestive secretions including gastrin, HCl, and bile. Incorporating "bitters" such as rocket (arugula), dandelion greens, or herbal tinctures (gentian, wormwood) 15 minutes before a meal can prime the stomach for digestion.
3. Exogenous Acidification (Betaine HCl)
For those with confirmed hypochlorhydria, supplemental Betaine Hydrochloride with Pepsin can be transformative.
- —This is a clinical protocol where the patient takes increasing doses of HCl capsules with meals until a warm sensation is felt, then backs off slightly.
- —This "re-acidifies" the stomach, allowing for protein digestion and mineral absorption while providing the signal for the LOS to close.
- —*Crucially, this must never be done in the presence of an active ulcer or if the patient is taking NSAIDs (like Ibuprofen).*
4. Apple Cider Vinegar (ACV)
While less potent than Betaine HCl, raw apple cider vinegar in water before meals provides a mild acetic acid stimulus. For many with mild hypochlorhydria, this is enough to lower the pH into the "activation zone" for pepsin.
5. Managing the PPI Exit
One cannot simply stop PPIs "cold turkey" after long-term use due to the Hypergastrinaemia Rebound Effect. When the drugs are stopped, the body—which has been screaming for acid—suddenly floods the stomach with it, causing intense pain. Weaning must be done slowly, often bridging with H2 blockers (which are less potent) and then natural acidifiers like D-Limonene and slippery elm to protect the mucosa as the pumps come back online.
6. Addressing SIBO and Microbial Balance
Once the "acid gate" is restored, the "intruders" in the small intestine must be dealt with. This often involves a "Kill, Flush, Heal" protocol:
- —Kill: Using herbal antimicrobials (allicin, oregano oil, berberine) to reduce the bacterial overgrowth.
- —Flush: Supporting the Migrating Motor Complex (MMC) with prokinetics (like ginger or 5-HTP).
- —Heal: Providing the nutrients necessary for the gut lining to repair (L-Glutamine, Zinc Carnosine).
##
Summary: Key Takeaways
The UK’s digestive health crisis is not a mystery; it is a predictable biological consequence of systematic acid suppression. By prioritising "comfort" over "function," we have traded temporary relief from heartburn for a lifetime of SIBO, malabsorption, and systemic immune dysfunction.
- —Stomach acid is the primary immunological barrier: Without it, the "sterile" small intestine is left vulnerable to colonisation by pathogenic and commensal bacteria.
- —PPIs are a double-edged sword: While useful for acute healing of ulcers, their long-term use in the UK is a primary driver of the SIBO epidemic.
- —The "High Acid" myth: Most cases of reflux are caused by *low* acid and the resulting failure of the Lower Oesophageal Sphincter to close, coupled with gas pressure from bacterial fermentation.
- —Recovery is possible: Through vagal stimulation, bitter herbs, and cautious acidification, the gastric furnace can be relit, restoring the body's ability to protect itself and extract nutrition from the diet.
The path to Innerstanding requires us to look past the "quick fix" of the prescription pad and respect the evolutionary wisdom of the stomach’s acidic fire. Only then can we address the root cause of the UK’s gut health crisis.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Hypochlorhydria: Why Low Acid is the Real UK Digestive Crisis"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper