Proton Pump Inhibitors: The Link Between Acid Suppression and Fracture Risk
Long-term use of PPIs for gastric reflux can significantly impair the intestinal absorption of vital bone minerals like calcium and magnesium. Understanding the metabolic trade-off of acid suppression is essential for maintaining long-term skeletal density.

Overview
For decades, the pharmaceutical industry has championed Proton Pump Inhibitors (PPIs) as the gold standard for managing gastroesophageal reflux disease (GORD), peptic ulcers, and general dyspepsia. These drugs, including household names like Omeprazole, Lansoprazole, and Esomeprazole, are among the most frequently prescribed medications in the United Kingdom. However, beneath the surface of symptomatic relief lies a profound biological trade-off that is only now beginning to be fully appreciated by the wider public. At INNERSTANDING, we believe that the suppression of gastric acid—a fundamental physiological process—cannot occur without systemic consequences. One of the most devastating and well-documented of these consequences is the progressive erosion of skeletal integrity.
The link between long-term PPI use and an increased risk of osteoporotic fractures is not merely a statistical correlation; it is a predictable outcome of altered human biochemistry. By fundamentally changing the pH of the stomach, these medications disrupt the delicate mechanism of mineral absorption and hormonal signalling that maintains the human skeleton. We are currently witnessing a silent epidemic of "brittle bone" syndrome among the middle-aged and elderly, many of whom have been maintained on these "acid blockers" for years, often without a clear clinical indication or an exit strategy.
This article serves as a deep dive into the metabolic wreckage caused by chronic acid suppression. We will expose how the inhibition of the H+/K+-ATPase enzyme creates a cascade of malabsorption, hormonal dysregulation, and cellular dysfunction that ultimately culminates in hip, spine, and wrist fractures. To understand the risk, one must first understand the vital necessity of the very substance these drugs seek to eliminate: hydrochloric acid.
Statistics from the MHRA (Medicines and Healthcare products Regulatory Agency) and the NHS indicate that over 60 million prescriptions for PPIs are issued annually in the UK. Studies suggest that long-term users have a 25% to 50% increased risk of vertebral and hip fractures compared to non-users.
##
##
The Biology — How It Works
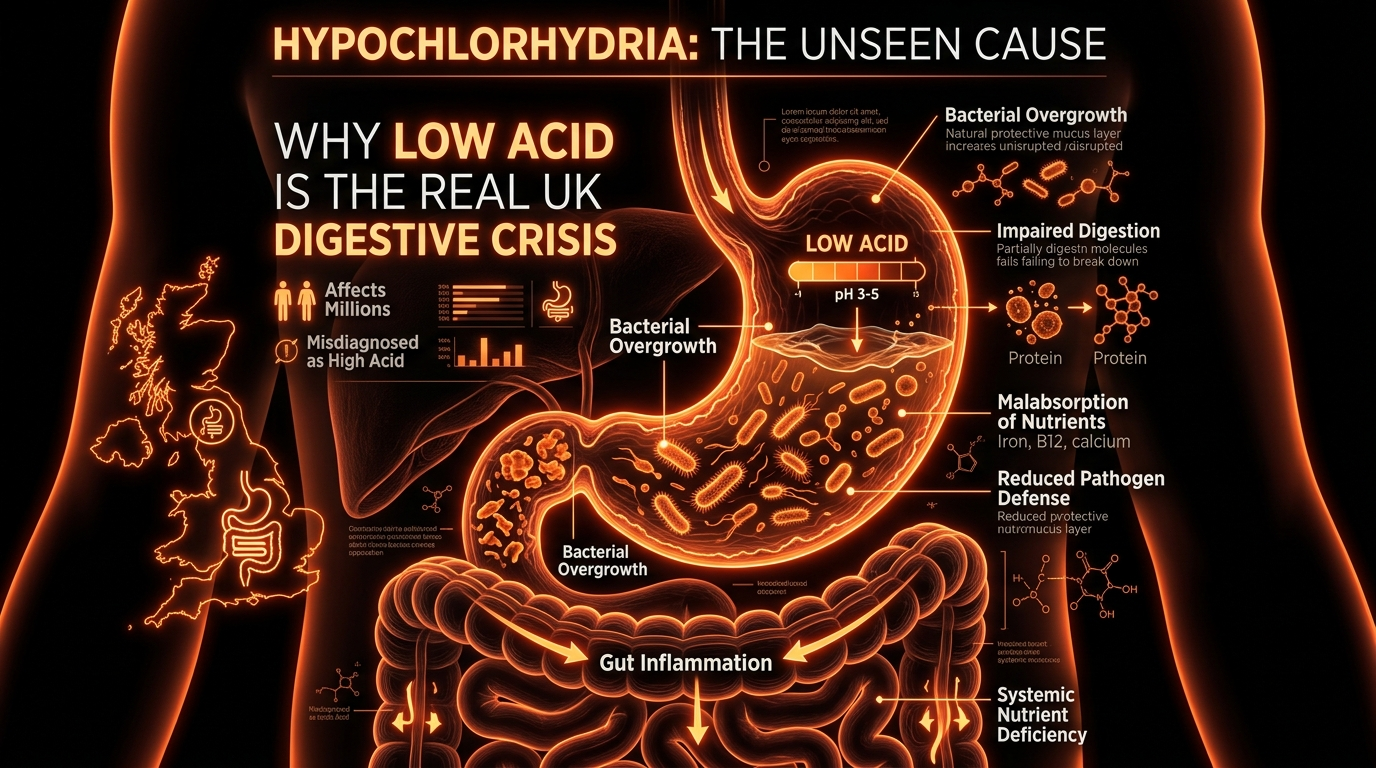
To comprehend why a stomach medication affects the density of a femur, we must first examine the biology of the gastric environment. The human stomach is designed to be an incredibly hostile, acidic environment, typically maintaining a pH between 1.5 and 3.5. This acidity is not a biological "error" or a design flaw; it is a critical requirement for digestion, sterilisation, and nutrient liberation.
The Role of Parietal Cells
The production of stomach acid occurs within specialised cells in the gastric lining known as parietal cells. These cells contain a specific enzyme system called the hydrogen-potassium adenosine triphosphatase (H+/K+-ATPase), commonly referred to as the "proton pump." This pump is the final step in the secretion of hydrochloric acid (HCl) into the stomach lumen. It works by actively transporting hydrogen ions (protons) out of the cell and into the stomach in exchange for potassium ions.
The PPI Mechanism of Action
Proton Pump Inhibitors are prodrugs that are absorbed into the systemic circulation and then travel back to the parietal cells. Once they encounter the acidic environment of the parietal cell’s secretory canaliculi, they are converted into their active form (sulfenamides). These active molecules form a permanent, covalent bond with the cysteine residues of the H+/K+-ATPase enzyme. By "locking" the pump, PPIs effectively shut down the production of acid at the source.
While this is highly effective at stopping the "burn" of reflux, it creates a state of hypochlorhydria (low stomach acid) or even achlorhydria (no stomach acid). The biological cost of this state is immense. Gastric acid is the primary catalyst required to break down complex food matrices and to ionise minerals into a form that the small intestine can actually recognise and absorb.
The Solubilisation of Minerals
Most minerals found in our diet, particularly calcium, do not exist as free ions. They are often bound to proteins or exist in complex salt forms, such as calcium carbonate. In order for calcium to be absorbed in the duodenum (the first part of the small intestine), it must first be "solubilised." This requires a highly acidic environment to break the chemical bonds and release the calcium ions. When PPIs raise the gastric pH toward neutrality (pH 5 or 6), this solubilisation fails. The calcium remains in an insoluble salt form, passing through the digestive tract largely unabsorbed.
##
##
Mechanisms at the Cellular Level
The skeletal system is not a static scaffold; it is a dynamic, living tissue that undergoes constant "remodelling." This process is governed by a balance between osteoblasts (cells that build bone) and osteoclasts (cells that break down bone). PPIs disrupt this balance through several distinct cellular pathways.
Calcium Malabsorption and the PTH Response
As established, PPIs impair the absorption of calcium, particularly from carbonate sources. When the gut fails to deliver sufficient calcium to the bloodstream, the body’s "calcium-sensing" mechanisms detect a drop in serum levels. In response, the parathyroid glands secrete Parathyroid Hormone (PTH).
PTH is the master regulator of bone resorption. Its job is to ensure that blood calcium levels remain stable, even at the expense of the skeleton. High levels of PTH signal the osteoclasts to accelerate the breakdown of bone matrix to release stored calcium into the blood. This condition, known as secondary hyperparathyroidism, is a direct driver of decreased bone mineral density (BMD) in long-term PPI users.
Magnesium Depletion and TRPM6/7 Channels
Perhaps even more alarming than calcium malabsorption is the link between PPIs and hypomagnesaemia (low blood magnesium). Magnesium is a cofactor for over 300 enzymatic reactions, including those that activate Vitamin D and regulate the mineralisation of the bone matrix.
The mechanism here involves the TRPM6 and TRPM7 (Transient Receptor Potential Melastatin) channels in the intestinal lining. These channels are responsible for the active transport of magnesium. Research indicates that the functioning of these channels is pH-dependent. By altering the local pH at the surface of the intestinal epithelium, PPIs inhibit the activity of these channels, leading to systemic magnesium deficiency. Low magnesium levels not only weaken the bone directly but also impair the secretion of PTH, creating a complex state of mineral dysregulation.
The Hypergastrinaemia Hypothesis
The body possesses a feedback loop: when the stomach is not acidic enough, the "G cells" in the stomach lining secrete a hormone called gastrin to signal for more acid. Because the PPIs have physically blocked the pumps, the gastrin levels continue to rise, leading to a state called hypergastrinaemia.
Recent biological research suggests that chronically high gastrin levels may have a direct effect on the parathyroid glands, causing them to grow (hyperplasia) and further driving the cycle of bone resorption. Gastrin may also directly stimulate the precursors of osteoclasts, accelerating the rate at which bone is dissolved.
Direct Inhibition of Bone Proton Pumps
In a fascinating and overlooked piece of cellular biology, it has been discovered that osteoclasts—the cells that dissolve bone—actually utilise their own versions of the H+/K+-ATPase proton pump to create the acidic environment necessary to dissolve bone mineral. While one might assume PPIs would therefore *stop* bone breakdown by inhibiting these pumps, the reality is more complex. The specific isoforms of the pumps in bone are slightly different from those in the stomach, and the systemic disruption of mineral homeostasis far outweighs any potential "protective" effect on the bone cells themselves.
##
##
Environmental Threats and Biological Disruptors
The rise of PPI-induced bone disease cannot be viewed in isolation from our modern environment. We live in an era where digestive dysfunction is ubiquitous, driven by highly processed diets, chronic psychological stress, and the widespread use of other biological disruptors.
The GORD Epidemic
Gastroesophageal Reflux Disease (GORD) is often framed as a disease of "too much acid." However, many functional biological researchers argue that it is frequently a disease of too little acid or poor esophageal sphincter tone. When stomach acid is low, food ferments in the stomach, creating gas and pressure that forces the lower esophageal sphincter (LES) open, allowing what little acid is present to splash into the esophagus.
By prescribing a PPI for this condition, mainstream medicine treats the symptom but exacerbates the underlying biological failure. This creates a "vicious cycle" where the patient becomes dependent on the drug to prevent the "burn," while their mineral status silently collapses in the background.
Synergy with Other Medications
The UK population is increasingly "poly-medicated." When PPIs are combined with other drugs that affect bone health, the risk of fracture skyrockets.
- —Glucocorticoids: Often used for asthma or arthritis, these drugs are notorious for causing osteoporosis.
- —SSRIs: Selective Serotonin Reuptake Inhibitors have been shown to affect bone remodelling.
- —Loop Diuretics: Frequently used for hypertension, these increase the excretion of calcium in the urine.
The intersection of these drugs with PPIs creates a "perfect storm" for skeletal failure, yet patients are rarely warned of these synergistic threats.
##
##
The Cascade: From Exposure to Disease
The progression from the first dose of Omeprazole to a fractured hip in a London hospital is a slow-motion biological disaster. It is a cascade that involves multiple organ systems and physiological checkpoints.
Phase 1: The Digestive Shutdown
Within days of starting a PPI, the gastric pH rises. Protein digestion begins to suffer because the enzyme pepsin requires an acidic environment to be activated. This leads to larger, undigested protein fragments entering the small intestine, potentially triggering inflammation and "leaky gut" (intestinal permeability).
Phase 2: The Nutritional Void
As the months pass, the lack of acid prevents the liberation of Vitamin B12 from dietary proteins. B12 deficiency is a known risk factor for osteoporosis, as it leads to elevated levels of homocysteine, a toxic amino acid that interferes with the cross-linking of collagen in the bone matrix. Without strong collagen, bone becomes brittle, regardless of how much calcium is present.
Phase 3: Hormonal Compensation
The parathyroid glands begin to work overtime. PTH levels remain chronically elevated. The body is now in a state of "metabolic thievery," where the skeleton is being systematically stripped of its minerals to maintain the tight range of serum calcium required for heart and muscle function.
Phase 4: Structural Failure
Micro-fractures begin to develop in the trabecular (spongy) bone, particularly in the vertebrae. These are often asymptomatic until a sudden movement or a minor fall results in a catastrophic fracture. For the elderly, a hip fracture is not just a bone injury; it is a life-altering event with a high mortality rate within the first year of the injury.
##
##
What the Mainstream Narrative Omits
The narrative provided by many pharmaceutical manufacturers and occasionally mirrored by overstretched NHS resources often downplays the "low-level" risks of PPIs. However, there are several "suppressed truths" that must be addressed to fully understand the scope of the problem.
The "Rebound" Trap
One of the most insidious aspects of PPIs is Rebound Acid Hypersecretion (RAH). When a patient attempts to stop taking the drug, the body—which has been frantically trying to produce acid against the chemical blockade—suddenly overproduces gastrin and acid. This leads to a surge of symptoms far worse than the original reflux. Many patients mistake this for their "disease" returning, leading them to believe they must stay on the PPI for life. In reality, it is a drug-induced withdrawal symptom.
The Microbiome Shift
Stomach acid is the first line of defence against pathogens. By neutralising this acid, PPIs allow for the overgrowth of bacteria like Clostridium difficile and Small Intestinal Bacterial Overgrowth (SIBO). These microbial imbalances further interfere with nutrient absorption and create systemic inflammation, which is a known driver of bone loss (osteimmuniology).
The Myth of "Safe" Over-the-Counter Use
In the UK, PPIs like Omeprazole are available over-the-counter (OTC) at chemists. This gives the public a false sense of security. The biological impact of a 20mg dose of Omeprazole is significant, regardless of whether it was prescribed by a GP or bought off the shelf. The lack of medical supervision for OTC users means that mineral levels are almost never monitored, and the "bone-stripping" effect goes entirely unnoticed until a fracture occurs.
##
##
The UK Context
The situation in the United Kingdom is particularly concerning due to the sheer volume of prescriptions and the traditional "set and forget" approach to chronic medication management.
NHS Prescribing Trends
According to data from the NHS Business Services Authority, PPIs consistently rank in the top three most prescribed drug classes by volume. In many GP surgeries, patients have been on these medications for 5, 10, or even 20 years. The NICE (National Institute for Health and Care Excellence) guidelines suggest that PPIs should be used at the lowest effective dose for the shortest possible time, yet this is rarely implemented in the reality of primary care.
The MHRA Warnings
The MHRA has issued several safety updates regarding PPIs. In 2012, they issued a specific warning about the risk of hypomagnesaemia with long-term use. In 2015, they acknowledged the increased risk of fractures, especially when used in high doses or for durations longer than a year. Despite these warnings, the rate of prescribing has not seen a significant decline, and many patients remain unaware of the risks.
The British Orthopaedic Association has noted that the cost of treating fragility fractures is a significant burden on the NHS, estimated at over £4 billion per year. A considerable portion of these fractures could be linked to medication-induced bone loss.
##
##
Protective Measures and Recovery Protocols
For those who have been caught in the PPI trap, the path to skeletal recovery requires a strategic biological approach. One must address the root cause of the reflux while simultaneously rebuilding the mineral reserves of the bone.
1. The Strategic Taper
One should never stop a PPI "cold turkey" due to the rebound effect mentioned earlier. A gradual tapering process, often spanning 4 to 8 weeks, is necessary. This involves slowly reducing the dose while introducing alternative methods of acid management.
2. Restoring Gastric Acidity
The goal is to restore the stomach's natural pH. This can often be supported by:
- —Betaine HCl with Pepsin: Supplementing with hydrochloric acid capsules at the start of protein-heavy meals (this must be done under the guidance of a knowledgeable practitioner).
- —Apple Cider Vinegar: Taking a tablespoon in a small amount of water before meals can provide a gentle acidic "prime" to the stomach.
- —Digestive Bitters: Herbs like gentian or dandelion root stimulate the body’s own production of gastric juices.
3. Bioavailable Mineral Supplementation
Standard calcium carbonate is ineffective when stomach acid is low. For those recovering from PPI use, Calcium Citrate or Calcium Malate are preferred, as they are significantly less dependent on gastric acid for absorption.
- —Magnesium Bisglycinate: This form is highly bioavailable and less likely to cause digestive upset.
- —Vitamin K2 (MK-7): Essential for "directing" calcium into the bones and keeping it out of the arteries.
- —Vitamin D3: Necessary for the expression of calcium-binding proteins in the gut.
4. Lifestyle and Environmental Shifts
- —The "Low-Carb" Connection: Many cases of GORD are exacerbated by high-carbohydrate diets that promote fermentation in the stomach. Reducing refined sugars and grains can often eliminate the need for acid suppression.
- —Stress Management: The vagus nerve controls both the lower esophageal sphincter and acid production. Chronic "fight or flight" mode inhibits proper digestion.
- —Melatonin: Interestingly, melatonin is produced in high amounts in the gut and has been shown to strengthen the lower esophageal sphincter, providing a natural defence against reflux.
##
##
Summary: Key Takeaways
The skeletal consequences of Proton Pump Inhibitor use are a stark reminder that in biology, there is no such thing as a "free lunch." When we chemically suppress a vital function like acid production, the ripples are felt throughout the entire organism.
- —PPIs permanently disable the H+/K+-ATPase enzyme, leading to a state of hypochlorhydria that makes mineral absorption nearly impossible.
- —The fracture risk is cumulative; the longer one stays on these medications, the more the bone matrix is compromised.
- —Calcium and Magnesium are the primary victims, but B12 and protein digestion are also significantly impaired.
- —Secondary Hyperparathyroidism is the biological "thief" that strips the skeleton to maintain blood calcium levels.
- —The UK faces a crisis of over-prescription, with millions of citizens unaware that their "indigestion pill" is weakening their spine.
- —Recovery is possible through a combination of strategic tapering, restoring natural stomach acid, and using bioavailable mineral forms like calcium citrate.
At INNERSTANDING, we urge readers to look beyond the "quick fix" of symptomatic relief and consider the long-term biological integrity of their bodies. The skeleton is your foundation; do not allow it to be dissolved by a misunderstanding of your own digestive fire.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Proton Pump Inhibitors: The Link Between Acid Suppression and Fracture Risk"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Bone & Mineral Health — products curated by our research team for educational relevance and biological support.

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

MSM Sulphur – Nature’s Forgotten Mineral

Fulvic Minerals – Natural Rare Earth Minerals. The essential trace elements missing from modern processed foods.
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper