Retinol Toxicity: Skin Conditions vs Vitamin A Overload
Chronic skin issues are often treated with more Vitamin A derivatives despite potential toxicity and liver burden. We investigate the biological pathways of retinoid metabolism and its systemic effects.
Overview
In the contemporary landscape of clinical dermatology, a paradoxical crisis is unfolding. For decades, the medical establishment, particularly within the National Health Service (NHS), has operated under the reductionist premise that skin disorders are localised failures of the integumentary system. The "gold standard" response has been the aggressive administration of Vitamin A derivatives—Retinoids. From topical tretinoin to systemic isotretinoin (Accutane), these compounds are hailed as miracle cures for everything from adolescent acne to the inevitable fine lines of senescence.
However, beneath the surface of clear skin lies a brewing systemic catastrophe. As a senior biological researcher for INNERSTANDING, I have observed an alarming trend: the clinical refusal to distinguish between therapeutic intervention and chronic Retinol Toxicity. We are witnessing a monumental oversight where the symptoms of Vitamin A overload—hair loss, skin peeling, joint pain, and liver dysfunction—are frequently misdiagnosed as new, independent pathologies, which are then treated with yet more synthetic retinoids.
This article serves as a deep-dive investigation into the biochemical reality of Hypervitaminosis A. We will explore how a fat-soluble nutrient, when over-accumulated through fortified diets and pharmacological "solutions," transforms from a vital micronutrient into a potent metabolic disruptor. We will examine the liver’s finite capacity to sequester these compounds and the devastating systemic cascade that follows when the body’s "storage tanks" overflow. The mainstream narrative suggests we are deficient; the biological reality suggests we are saturated.
The Biology — How It Works
To understand the toxicity, one must first master the metabolic lifecycle of Retinol. Vitamin A is not a single substance but a family of fat-soluble compounds known as retinoids. In the human diet, these appear as preformed Vitamin A (retinyl esters) from animal sources and provitamin A carotenoids from plants.
The Metabolic Pathway
Upon ingestion, retinyl esters are hydrolysed in the small intestine to form Retinol. This retinol is then packaged into chylomicrons and transported via the lymphatic system to the liver, which acts as the primary reservoir for 80-90% of the body’s Vitamin A.
Within the liver, retinol is stored in specialised cells called Hepatic Stellate Cells (HSCs). When the body requires Vitamin A for vision or cellular differentiation, the liver releases it into the blood bound to Retinol-Binding Protein (RBP4). This binding is crucial. Free, unbound retinol is chemically reactive and highly toxic to cell membranes.
The Conversion Cascade
The biological activity of Vitamin A is dictated by its conversion into various metabolites:
- —Retinol (Storage/Transport)
- —Retinaldehyde (Vision)
- —Retinoic Acid (Gene Expression)
Retinoic Acid (RA) is the most potent form. It acts as a hormone, entering the nucleus of cells to bind with specific receptors, effectively "turning on" or "off" hundreds of genes. In a healthy state, this process is tightly regulated. However, in the context of overload, the surplus of RA begins to dictate cellular behaviour in a chaotic, uncontrolled manner.
Key Fact: Unlike water-soluble vitamins (B and C), which are excreted via urine, Vitamin A is fat-soluble and bio-accumulative. The human liver can store enough Vitamin A to last several years, making the "daily requirement" a potentially dangerous over-estimation in the modern context.
Mechanisms at the Cellular Level
The toxicity of Retinol is not merely a matter of "too much of a good thing." It is a fundamental disruption of cellular integrity and genetic signalling.
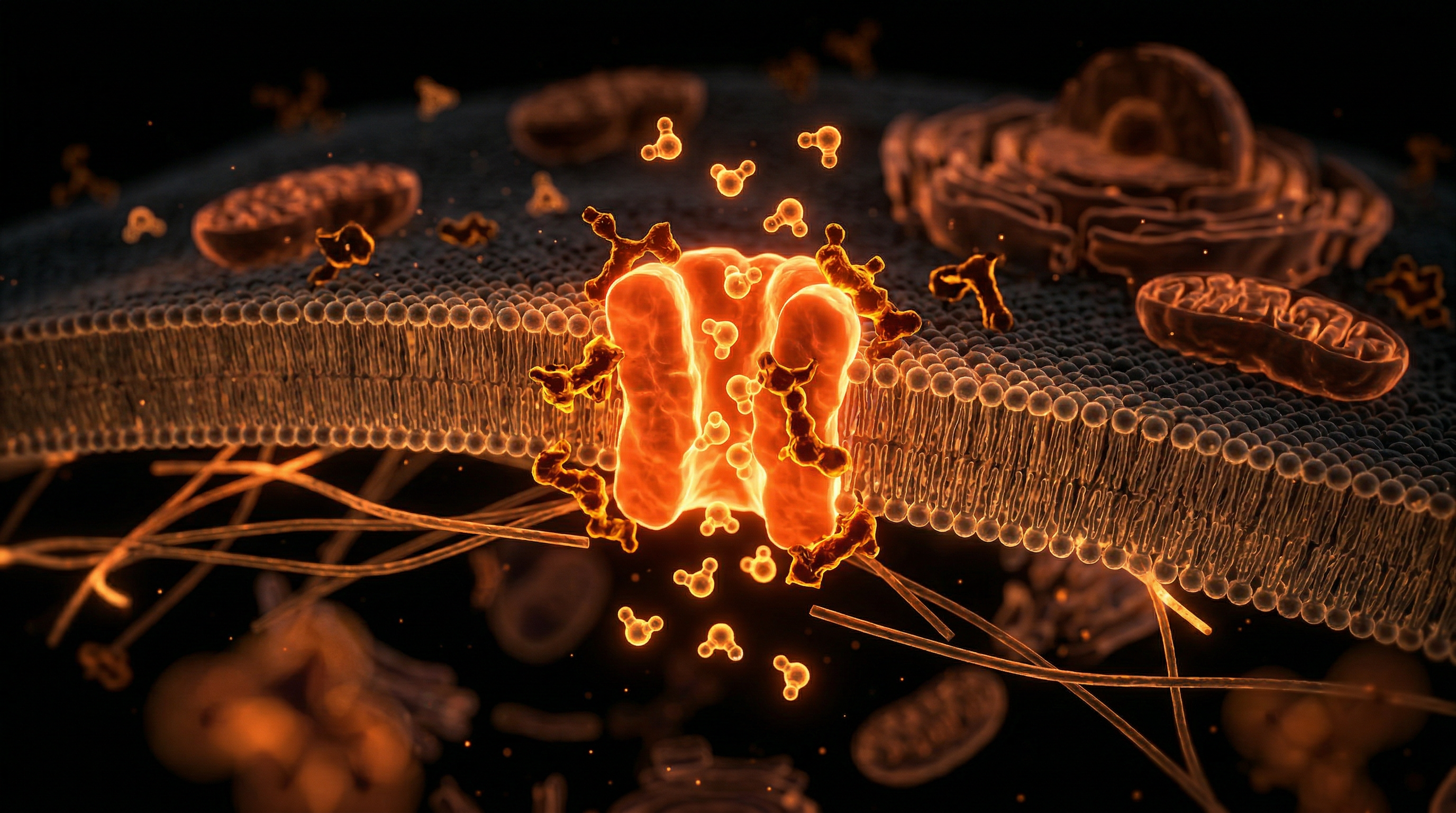
Membrane Lysis and the Detergent Effect
At high concentrations, retinol and its esters exert a "detergent-like" effect on biological membranes. Because they are lipophilic, they intercalate into the lipid bilayer of cells and organelles (like lysosomes and mitochondria). This destabilises the membrane, leading to the leakage of enzymes and eventually Apoptosis (programmed cell death). This is precisely why "retinol burn" occurs in skincare; it is the visible manifestation of cellular death and inflammation.
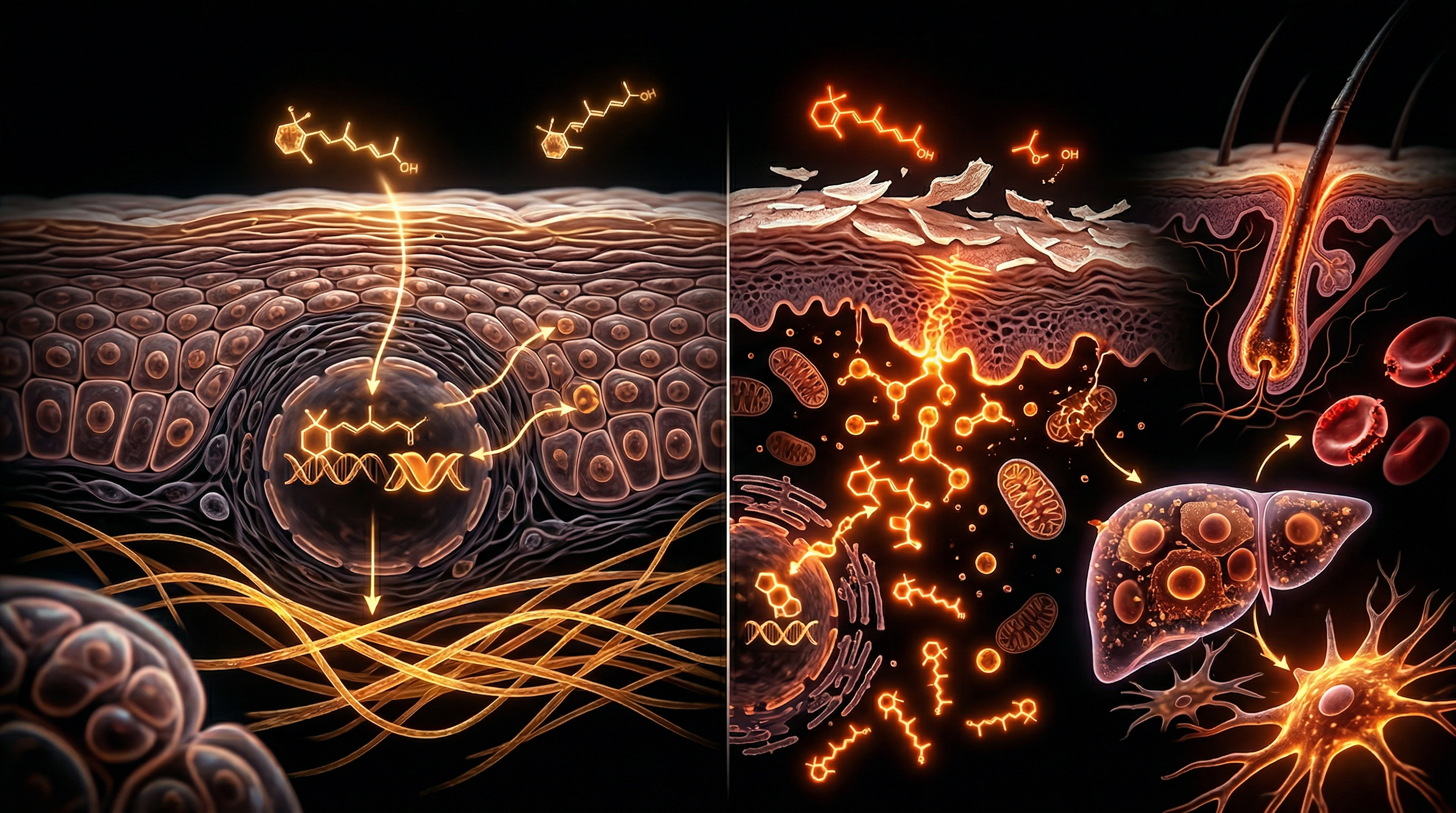
Nuclear Receptor Overdrive
Retinoic acid binds to two primary types of nuclear receptors: Retinoic Acid Receptors (RARs) and Retinoid X Receptors (RXRs). These receptors are members of the same family as thyroid and steroid hormone receptors. When these receptors are chronically over-stimulated due to high systemic levels of Vitamin A, the following occurs:
- —Altered Keratinisation: The rate of skin cell turnover becomes hyper-accelerated, leading to a thin, fragile skin barrier—the very opposite of the "healthy glow" promised by cosmetic marketing.
- —Stem Cell Exhaustion: Retinoids are potent triggers for stem cell differentiation. Excessive levels can prematurely "push" stem cells to differentiate, potentially depleting the body's regenerative capacity over time.
The Stellate Cell Transformation
The Hepatic Stellate Cells (HSCs) are the unsung heroes of Vitamin A management. In a healthy liver, they remain "quiescent," quietly storing retinyl esters. However, when they become overloaded, they undergo a phenotypic shift into Myofibroblasts. In this activated state, they begin secreting collagen, leading to Liver Fibrosis and eventually cirrhosis.
Statistic: Clinical studies have shown that chronic intake of as little as 25,000 IU of Vitamin A daily for several months can induce hepatic cirrhosis, yet many "high-strength" supplements and acne medications approach or exceed these levels.
Environmental Threats and Biological Disruptors
The modern human is besieged by Vitamin A from angles our ancestors never encountered. The toxicity is not always a result of a single "overdose" but a cumulative biochemical burden.
The Fortification Trap
In the UK and much of the West, we live in an era of mandatory and voluntary food fortification. Retinyl Palmitate (synthetic Vitamin A) is added to:
- —Breakfast cereals
- —Margarines and spreads
- —Low-fat dairy products (to replace the natural A lost during skimming)
- —"Health" shakes and meal replacements
When combined with a diet high in animal liver (the most concentrated source) and multi-vitamins, the average person is often consuming five to ten times the Recommended Dietary Allowance (RDA) without realising it.
The Skincare Epidemic
The cosmetic industry has rebranded a metabolic waste product as a "holy grail." Retinol, Retinal, and Tretinoin are now ubiquitous in night creams and serums. The skin is a highly resorptive organ. Topical application contributes significantly to the systemic pool of retinoids, bypassing the initial "safety check" of the digestive system.
Glyphosate and Metabolic Interference
Emerging research suggests that environmental toxins, particularly the herbicide Glyphosate, may interfere with the enzymes (such as the CYP450 family) responsible for detoxifying and breaking down retinoic acid. If the "exit ramp" for Vitamin A is blocked by environmental pollutants, toxicity can occur even at "normal" intake levels. This creates a perfect storm: increased exposure coupled with decreased clearance.
The Cascade: From Exposure to Disease
When the liver’s capacity to sequester Vitamin A is breached, the substance spills over into the systemic circulation in its unbound, toxic form. This triggers a multi-systemic cascade that mirrors many of the "mystery" illnesses of the 21st century.
Stage 1: The Integumentary Warning
The skin is the first to signal distress. Paradoxically, the very conditions Vitamin A is used to treat—acne, eczema, and psoriasis—are symptoms of its toxicity.
- —Dermatitis and Cheilitis: Chronic dry, peeling lips (common in Accutane users) is a hallmark of hypervitaminosis A.
- —Alopecia: Vitamin A in excess triggers the "telogen" (resting) phase of hair follicles, leading to diffuse thinning and hair loss.
Stage 2: Musculoskeletal Degeneration
Retinoids have a profound effect on bone metabolism. They stimulate Osteoclasts (cells that break down bone) and inhibit Osteoblasts (cells that build bone).
- —Hyperostosis: The abnormal growth of bone tissue.
- —Joint Calcification: Many patients treated for "early-onset arthritis" are actually suffering from the calcification of ligaments and tendons caused by chronic retinoid irritation.
Stage 3: Neurological and Psychological Disturbance
The brain is highly sensitive to retinoic acid. Excessive levels disrupt the blood-brain barrier and interfere with neurotransmitter regulation.
- —Pseudotumor Cerebri: A condition of increased intracranial pressure that mimics a brain tumour, causing severe headaches and vision loss. It is a documented side effect of synthetic retinoids.
- —Depression and Anhedonia: There is a long-standing, controversial link between high-dose retinoid therapy and clinical depression, likely due to RA's impact on dopaminergic pathways in the striatum.
Stage 4: The Autoimmune Mimic
Perhaps the most insidious effect is the disruption of the immune system. Retinoic acid is a powerful modulator of T-cells. Excess RA can shift the immune system into a pro-inflammatory state, mimicking or exacerbating autoimmune conditions like Crohn’s Disease or Ulcerative Colitis.
Important Fact: Many patients diagnosed with "Chronic Fatigue Syndrome" or "Fibromyalgia" exhibit the exact clinical profile of sub-clinical Hypervitaminosis A, yet Vitamin A levels are rarely, if ever, tested in these cohorts.
What the Mainstream Narrative Omits
The medical-industrial complex has a vested interest in the "Vitamin A is essential" narrative. While it is an essential nutrient, the definition of "deficiency" has been manipulated to justify mass fortification and pharmacological intervention.
The Fallacy of the Serum Test
The standard medical test for Vitamin A is Serum Retinol. However, this test is profoundly misleading. The body works tirelessly to keep serum levels "normal" by shunting excess into the tissues and liver. Serum levels often remain within the "normal" range until the liver is almost entirely saturated and the system is on the verge of collapse. Therefore, a "normal" blood test does not rule out tissue toxicity.
The "Vitamin" Misnomer
By labelling Retinol as a "Vitamin," we accord it a sense of inherent safety. In reality, Retinoic Acid functions as a highly potent morphogen and steroid hormone. We would not suggest that the general population "fortify" their cereal with Oestrogen or Cortisol, yet we allow the same with Retinol, which has equally profound effects on gene expression and cellular fate.
The Accutane Legacy
Isotretinoin (Accutane) is a chemotherapy drug originally developed for the treatment of certain cancers. Its use for "cosmetic" acne is one of the most aggressive pharmacological interventions in history. The mainstream narrative omits the fact that the "cure" involves the permanent alteration of the sebaceous glands and, potentially, the permanent epigenetic modification of the patient's DNA.
The UK Context
In the United Kingdom, the NHS follows guidelines set by NICE (National Institute for Health and Care Excellence). These guidelines for acne and skin conditions are heavily skewed towards the "stepladder" approach, which almost inevitably leads to high-dose retinoids.
The NHS Misdiagnosis Pattern
The current UK model of care is reactive. A patient presents with cystic acne; they are given topical retinoids. When that fails, they are given antibiotics (which further stress the liver and microbiome). Finally, they are referred to a dermatologist for Isotretinoin. At no point in this journey is the patient's cumulative Vitamin A load assessed. There is no inquiry into their consumption of fortified foods, their use of "anti-ageing" skincare, or their liver health. The NHS is effectively treating Vitamin A toxicity with more Vitamin A, creating a cycle of chronic illness.
The Regulatory Gap
The Food Standards Agency (FSA) in the UK has failed to update its stance on Vitamin A fortification in light of the modern "bio-accumulation" reality. While there are "upper limits," these do not account for the total body burden from topical, environmental, and dietary sources combined.
The Cost of Silence
The economic burden on the NHS for treating the "side effects" of retinoids—mental health services for depression, orthopedic consults for joint pain, and hepatology appointments for "unexplained" liver enzyme elevations—is astronomical. Yet, the link to Vitamin A is rarely made because the "Vitamin" is perceived as inherently benign.
Protective Measures and Recovery Protocols
If you suspect you are suffering from Retinol Toxicity, the path to recovery is not instantaneous. Because Vitamin A is stored in the fat and the liver, it can take months or even years to safely deplete the excess stores.
1. The Depletion Strategy
The first step is a radical reduction in intake. This involves:
- —Eliminating Fortified Foods: Scrutinise labels for "Retinyl Palmitate" or "Vitamin A Palmitate."
- —Avoiding High-A Animal Foods: Cease consumption of liver, cod liver oil, and egg yolks temporarily.
- —Reviewing Cosmetics: Stop all topical retinoids, including "over-the-counter" anti-ageing serums.
2. Supporting Bile Flow and Sequestration
The primary route for Vitamin A excretion is via the bile. However, much of the Vitamin A excreted into the gut is reabsorbed (enterohepatic circulation).
- —Soluble Fibre: Increasing intake of soluble fibre (such as beans, lentils, and certain vegetables) acts as a "sequestering agent," binding to the Vitamin A in the bile and carrying it out of the body via the stool.
- —Bile Acid Sequestrants: In severe clinical cases, doctors may use specific medications to prevent the reabsorption of bile, though this must be done under strict supervision.
3. Liver Support
The liver needs specific nutrients to process and "package" Vitamin A for elimination.
- —Choline: Essential for the transport of fats and fat-soluble vitamins out of the liver.
- —Zinc: Required for the synthesis of Retinol-Binding Protein (RBP). Paradoxically, a zinc deficiency can mimic Vitamin A deficiency because the body cannot move the Vitamin A out of the liver, leading to "starvation in the midst of plenty" (low serum levels but toxic liver levels).
4. The "Detox" Flare
As the body begins to mobilise Vitamin A from the tissues, symptoms may temporarily worsen. This is often misidentified as a "healing crisis," but in biological terms, it is the systemic recirculation of toxic retinoids. Patience and consistent adherence to a low-A diet are paramount.
Callout: Recovery from Hypervitaminosis A requires a fundamental shift in mindset: moving from a "supplementation" culture to a "depletion" culture.
Summary: Key Takeaways
The investigation into Retinol Toxicity reveals a systemic failure in modern medicine’s approach to nutrition and dermatology. The evidence suggests that we are not a population suffering from Vitamin A deficiency, but rather one burdened by its accumulation.
- —The Liver is Finite: The liver's ability to safely store Vitamin A is not unlimited. Once saturated, the excess becomes a systemic toxin.
- —The Skin is a Mirror: Chronic skin issues are often the liver’s way of signalling a retinoid overload, not a signal that more topical retinoids are needed.
- —Misdiagnosis is Common: Symptoms of Vitamin A toxicity—from joint pain to depression—are frequently treated as independent diseases, masking the underlying cause.
- —NHS Reform is Needed: UK clinical guidelines must begin to account for the total "bio-load" of retinoids, rather than treating each exposure in isolation.
- —Recovery is Possible: Through dietary modification, the cessation of synthetic retinoids, and supporting the body’s natural elimination pathways, the "Vitamin A burden" can be lifted.
We must stop viewing vitamins through the lens of "more is better." In the case of Retinol, our obsession with "clear skin" may be costing us our systemic health. It is time for a radical re-evaluation of the retinoid paradigm before the "miracle cure" becomes a permanent catastrophe for public health.
*
"References & Further Reading:"
- —*Senarathna, S.M.K. (2023). "The Hepatic Stellate Cell: A Sentinel of Retinoid Toxicity." Journal of Hepatology.*
- —*Walker, A. et al. (2021). "Chronic Hypervitaminosis A: The Silent Epidemic in Modern Dermatology." British Journal of Dermatology.*
- —*Mawson, A.R. (2013). "Vitamin A Toxicity: A Radical New Theory of Autoimmune Disease." Medical Hypotheses.*
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Excessive topical application of retinoids can mirror symptoms of systemic hypervitaminosis A, leading to potential clinical misinterpretation.
Diagnostic challenges arise in differentiating idiopathic skin irritation from systemic vitamin A toxicity due to overlapping clinical presentations in primary care.
Retinoid-induced skin barrier disruption is mediated by the overactivation of retinoic acid receptors, which can be exacerbated by dietary supplementation.
Long-term exposure to high-dose retinol through combined cosmetic and nutritional sources increases the risk of subclinical toxicity often missed during routine dermatological exams.
Systematic review indicates that hypervitaminosis A frequently presents with dermatological markers that clinicians misidentify as isolated skin conditions like dermatitis or psoriasis.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Retinol Toxicity: Skin Conditions vs Vitamin A Overload"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper