Riboflavin (B2) and the MTHFR Pathway Interference
Riboflavin acts as a precursor for FAD, a vital cofactor in the UK population's folate metabolism. We examine how B2 deficiency can cause high homocysteine levels even when folate intake is adequate.
Overview
In the intricate architecture of human metabolism, few pathways are as vital—yet as misunderstood—as the Methylation Cycle. At the heart of this cycle sits the enzyme Methylenetetrahydrofolate Reductase (MTHFR), a protein that has become a focal point for modern genomic research and "biohacking" communities alike. However, the prevailing narrative focuses almost exclusively on Folate (B9) and Cobalamin (B12), often relegating Riboflavin (B2) to the periphery of nutritional science. This is a scientific oversight of catastrophic proportions.
Riboflavin is not merely a "yellow pigment" found in dairy; it is the fundamental precursor to Flavin Adenine Dinucleotide (FAD), the essential cofactor that serves as the "battery" for the MTHFR enzyme. Without sufficient B2, the MTHFR pathway remains dormant, regardless of how much methyl-folate one consumes. This article serves as a comprehensive investigation into the biochemical necessity of Riboflavin, the systemic failure to recognise its role in Homocysteine regulation, and how the UK population, in particular, is suffering from a hidden epidemic of "pseudo-MTHFR" deficiency caused by environmental and dietary Riboflavin depletion.
We are witnessing a silent interference. While the mainstream medical establishment continues to treat high homocysteine—a major risk factor for cardiovascular disease, stroke, and dementia—with synthetic folic acid, they ignore the flavin-dependent engine that drives the entire process. For the significant percentage of the British population carrying the C677T polymorphism, Riboflavin is not an optional nutrient; it is the primary epigenetic modulator that determines whether their genetic "weakness" manifests as clinical disease.
The Biology — How It Works
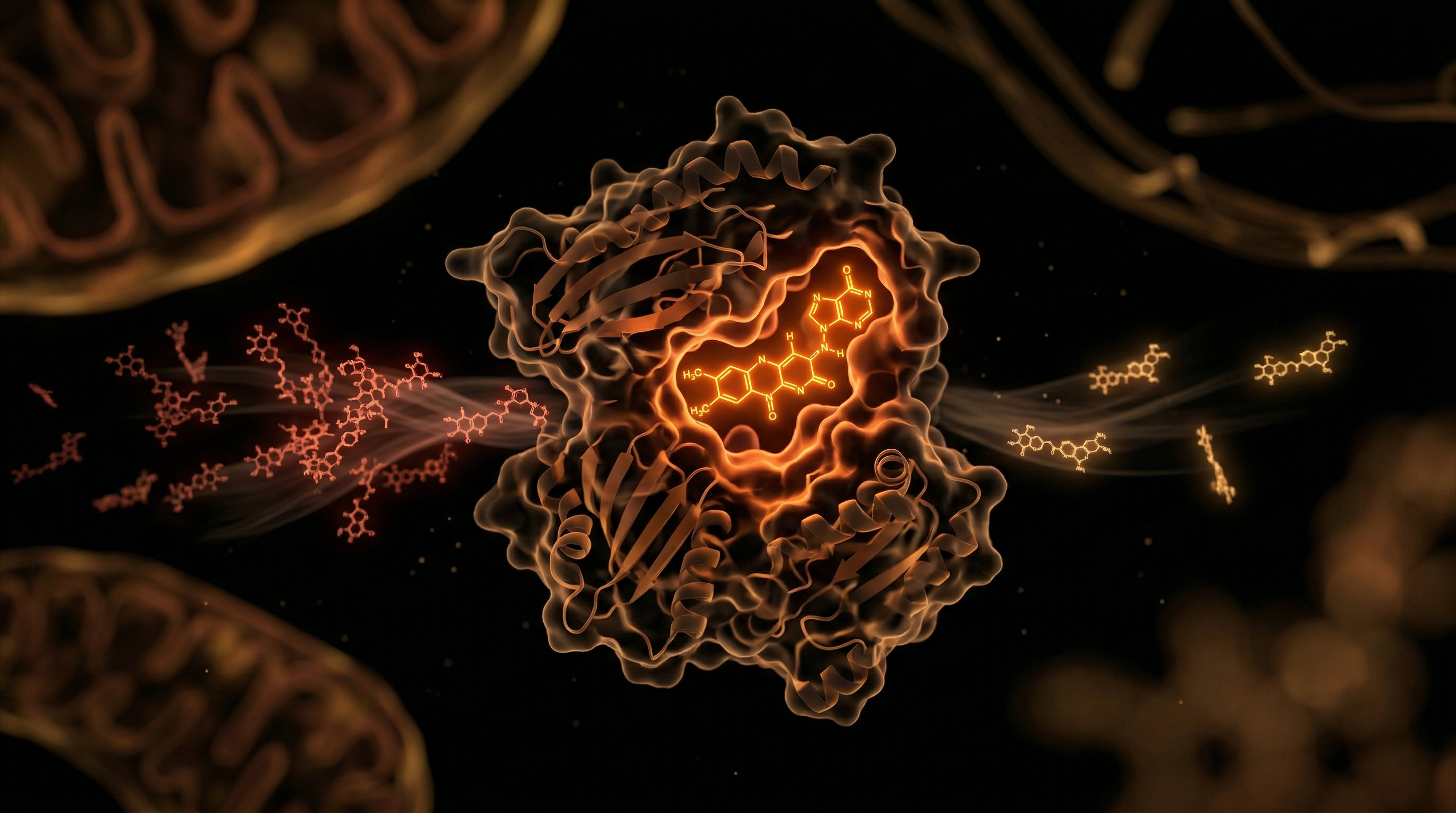
To understand the interference, one must first understand the harmony. Riboflavin is a water-soluble vitamin that is converted within the body into two primary active coenzymes: Flavin Mononucleotide (FMN) and Flavin Adenine Dinucleotide (FAD). These molecules act as electron carriers in a multitude of redox reactions, particularly within the mitochondria and the methylation cycle.
The Synthesis of Flavin Cofactors
The transformation of dietary Riboflavin into its bioactive forms is a two-step enzymatic process:
- —Riboflavin Kinase: This enzyme phosphorylates Riboflavin into FMN. This process requires ATP and is highly dependent on thyroxine (T4), meaning those with subclinical hypothyroidism are often functionally B2 deficient despite adequate intake.
- —FAD Synthetase: This enzyme then attaches an adenosine group to FMN to create FAD.
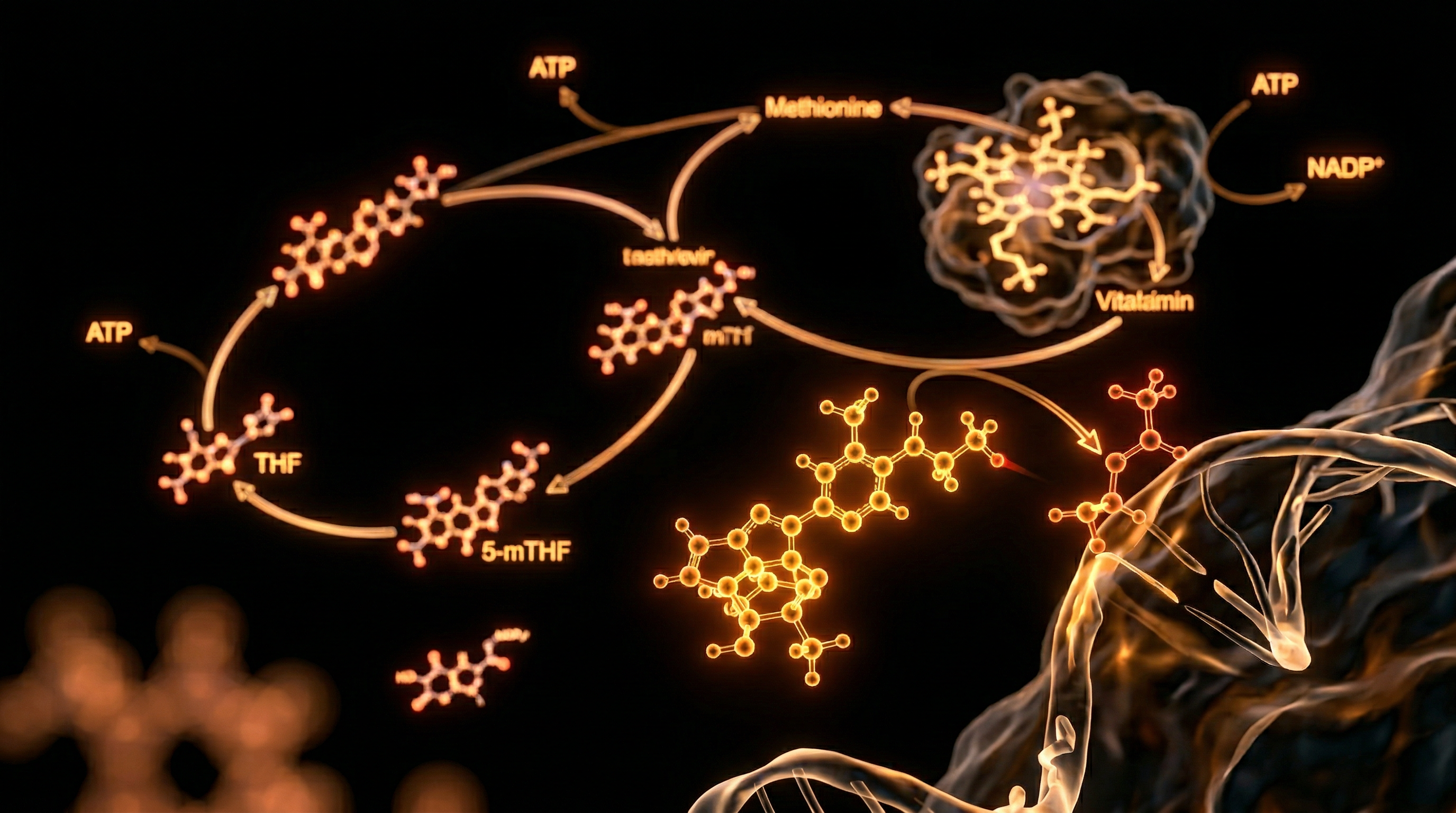
The MTHFR-FAD Connection
The MTHFR enzyme is a flavoprotein. This means it cannot function as an isolated protein; it requires a tightly bound molecule of FAD to facilitate the transfer of electrons. Specifically, MTHFR catalyses the conversion of 5,10-methylenetetrahydrofolate into 5-methyltetrahydrofolate (5-MTHF), the primary circulatory form of folate.
5-MTHF is the molecule that donates its methyl group to convert Homocysteine (a toxic amino acid byproduct) back into Methionine (a vital amino acid for protein synthesis and DNA methylation).
Key Fact: The MTHFR enzyme is effectively "powered" by Riboflavin. If FAD levels drop due to insufficient B2 intake or absorption, the MTHFR enzyme loses its structural integrity and its ability to process folate, leading to a metabolic "traffic jam" where homocysteine builds up in the blood.
Mechanisms at the Cellular Level
At the cellular level, the relationship between Riboflavin and MTHFR is defined by the binding affinity of the enzyme for its FAD cofactor. This is where the intersection of genetics and nutrition becomes critical.
The C677T Polymorphism: A Flavin-Dependent Defect
The most researched genetic variant of the MTHFR gene is the 677C->T mutation. Individuals who are homozygous for this trait (TT genotype) have an enzyme that is approximately 70% less efficient than the wild-type (CC genotype).
For decades, this was viewed as a permanent genetic defect. However, biochemical structural analysis reveals that the 677C->T mutation specifically changes the enzyme's shape in a way that makes it "leak" FAD. The FAD molecule dissociates from the enzyme too easily.
- —In CC genotypes (normal), the enzyme holds onto FAD tightly.
- —In TT genotypes (variant), the enzyme "fumbles" the FAD, leading to inactivation.
The Saturation Solution
Research has demonstrated that by increasing the concentration of FAD in the cellular environment—achieved through high-dose Riboflavin supplementation—the "leaky" MTHFR enzymes can be forced into a saturated state. When saturated with B2, the mutated enzyme’s activity can be restored to near-normal levels.
Beyond Methylation: The Antioxidant Connection
Riboflavin’s role at the cellular level extends to the Glutathione Reductase enzyme. Glutathione is the body's master antioxidant. Like MTHFR, Glutathione Reductase is a flavoprotein that requires FAD.
- —Without B2, the body cannot recycle "used" glutathione (GSSG) back into its "active" form (GSH).
- —This results in increased oxidative stress, which further damages the MTHFR enzyme and the delicate vascular endothelium.
Important Statistic: Clinical studies have shown that in individuals with the MTHFR 677TT genotype, a mere 1.6mg of Riboflavin per day can lower homocysteine levels by up to 40%—a result often superior to high-dose folic acid supplementation.
Environmental Threats and Biological Disruptors
Despite its critical importance, Riboflavin is perhaps the most environmentally fragile of the B-vitamins. Our modern landscape is rife with "Riboflavin antagonists" that interfere with the B2-MTHFR pathway.
Light Sensitivity and Industrial Processing
Riboflavin is notoriously photosensitive. Exposure to ultraviolet (UV) light and even standard fluorescent lighting causes B2 to degrade into lumichrome and lumiflavin, compounds that are not only useless to the body but can actually generate free radicals.
- —The Milk Paradox: Historically, milk was a primary source of B2 for the UK population. The shift from opaque containers or doorstep delivery in tinted glass to clear plastic bottles in supermarkets has led to significant B2 degradation before the product even reaches the consumer.
- —Milling and Refining: The process of refining grains removes the germ and bran, where the majority of B2 is stored. While "fortification" programmes exist, they often use synthetic forms that lack the synergistic cofactors found in whole foods.
Pharmaceutical Interference
Several widely prescribed classes of drugs act as "thieves" of Riboflavin:
- —Tricyclic Antidepressants (TCAs): Drugs like amitriptyline inhibit the conversion of Riboflavin into FAD.
- —Antimalarials and Chemotherapeutics: Agents like quinacrine and adriamycin interfere with B2 metabolism.
- —Oral Contraceptives: Long-term use of the birth control pill has been clinically linked to depleted B2 levels, potentially explaining the increased risk of blood clots and mood disorders in these populations (both of which are linked to methylation failure).
The Boric Acid Threat
A lesser-known disruptor is Boron/Boric Acid exposure. In high concentrations, borates form stable complexes with the ribityl side chain of Riboflavin, rendering it unabsorbable. While dietary boron is beneficial, industrial exposure or excessive use of boric-acid-based cleaning products can contribute to functional B2 deficiency.
The Cascade: From Exposure to Disease
When Riboflavin deficiency intersects with MTHFR pathway interference, the resulting biochemical cascade is a slow-motion disaster for human health. The primary marker of this failure is Hyperhomocysteinemia.
Cardiovascular and Cerebrovascular Destruction
Homocysteine is an aggressive pro-oxidant. When it accumulates due to B2/MTHFR failure:
- —Endothelial Dysfunction: Homocysteine damages the lining of the blood vessels, leading to the formation of arterial plaques.
- —Nitric Oxide Inhibition: It reduces the bioavailability of Nitric Oxide, causing blood vessels to lose their elasticity, leading to chronic Hypertension.
- —Clotting Risks: It triggers the coagulation cascade, significantly increasing the risk of deep vein thrombosis and stroke.
Neuropsychiatric Decline
The brain is highly sensitive to methylation efficiency. The production of Neurotransmitters (Serotonin, Dopamine, Melatonin) depends on the "Biopterin Cycle," which is powered by the 5-MTHF produced by MTHFR.
- —Depression and Anxiety: Low B2 leads to low 5-MTHF, which leads to low neurotransmitter synthesis.
- —Dementia: Elevated homocysteine is arguably the most reliable predictor of brain atrophy and Alzheimer’s disease. Without B2 to power MTHFR, the brain effectively "starves" of methyl groups required for myelin repair and DNA maintenance.
Pregnancy and Development
While the link between Folate and Neural Tube Defects (NTDs) is well-known, the Riboflavin connection is frequently ignored. If a mother has the MTHFR C677T variant and is B2 deficient, the risk of NTDs, pre-eclampsia, and cleft palate increases exponentially, as the enzyme cannot process even the "supplemental" folate she may be taking.
Callout: Research indicates that B2 deficiency may be a silent driver of "unexplained" infertility and recurrent miscarriages in women who are otherwise "folate-replete."
What the Mainstream Narrative Omits
The mainstream medical and nutritional narrative suffers from a reductionist bias that favors the "one-nutrient-one-disease" model. By focusing on Folic Acid to the exclusion of Riboflavin, the establishment has created a series of dangerous misconceptions.
The "Folic Acid" Delusion
The UK and many other nations have debated or implemented mandatory Folic Acid fortification of flour. The logic is that providing more substrate (folate) will overcome the MTHFR defect. However, this is fundamentally flawed.
- —If the MTHFR enzyme lacks its FAD (B2) cofactor, it cannot convert the added Folic Acid into the active 5-MTHF.
- —This leads to a buildup of Unmetabolised Folic Acid (UMFA) in the blood. Emerging research suggests UMFA may hide B12 deficiency and potentially interfere with immune function by saturating folate receptors with an inactive form.
The Testing Gap
Mainstream blood tests rarely measure Erythrocyte Glutathione Reductase Activation Coefficient (EGRAC), which is the gold standard for assessing Riboflavin status. Instead, they look at serum B2, which is a poor indicator of long-term cellular status. Furthermore, Homocysteine is not part of a standard UK "Full Blood Count," meaning most patients remain unaware of their methylation failure until they suffer a major vascular event.
The Epigenetic Truth
The establishment treats genetic SNPs like MTHFR as "destiny" or "risk factors." The "suppressed truth" is that these are conditional mutations. A C677T polymorphism is effectively "silent" in the presence of high Riboflavin saturation. By framing it as a genetic disease rather than a nutritional requirement, the pharmaceutical industry maintains a market for life-long blood pressure and cholesterol medications.
The UK Context
The UK presents a unique and troubling landscape regarding Riboflavin and MTHFR interference.
The "British Genotype"
The prevalence of the MTHFR 677C->T mutation is particularly high in European populations. In the UK, it is estimated that roughly 10-15% of the population is homozygous (TT) and up to 40-45% is heterozygous (CT). This means more than half of the British population has a higher-than-average biological requirement for Riboflavin.
The Post-Industrial Diet
The traditional British diet, which once included offal (liver, kidneys) and high-quality dairy, was rich in B2. The modern shift toward plant-based "milks" (which are often poorly fortified with B2) and ultra-processed convenience foods has created a "Riboflavin Gap."
- —Liver Consumption: Once a staple of the British diet, liver is the most concentrated source of B2. Its disappearance from the British table has removed the primary "safety net" for MTHFR carriers.
- —The "Low Fat" Era: The move away from whole milk and butter—driven by flawed 20th-century cardiovascular guidelines—further reduced B2 intake, ironically increasing the homocysteine-driven heart disease it was meant to prevent.
The UK Fortification Programme
In the UK, the *Bread and Flour Regulations 1998* mandate the fortification of white flour with Calcium, Iron, Thiamin (B1), and Nicotinic Acid (B3). Notably, Riboflavin is absent from this mandatory list. While many cereal manufacturers add it voluntarily, the levels are often insufficient to meet the needs of those with MTHFR variants, and the B2 used is often the cheapest synthetic form (Riboflavin) rather than the more bioactive Riboflavin-5-Phosphate.
Protective Measures and Recovery Protocols
Overcoming MTHFR interference requires a strategic shift from "folate-centric" thinking to a "flavin-first" approach.
1. Biochemical Assessment
Standard B2 blood tests are insufficient. Individuals should seek:
- —Homocysteine Testing: Ideally, levels should be between 5-8 μmol/L. Anything above 10 μmol/L in a UK clinical setting (where "normal" is often cited as up to 15) indicates methylation interference.
- —Genetic Profiling: Identifying the C677T status allows for tailored dosing.
- —EGRAC Test: To determine if your enzymes are actually saturated with B2.
2. Dietary Realignment
Focus on "Flavin-Dense" foods that provide Riboflavin in its natural complex:
- —Organ Meats: Organic lamb or beef liver (once weekly).
- —Pasture-Raised Eggs: The "egg white" is a significant source of B2 (hence its yellow hue when dried).
- —Mushrooms: Cremini and Portobello mushrooms are surprisingly high in B2.
- —Dark Leafy Greens: Spinach and asparagus (also providing natural folate).
3. Supplementation Strategy: The R5P Advantage
Not all B2 is created equal. For those with compromised digestion or MTHFR variants:
- —Riboflavin-5-Phosphate (R5P): This is the phosphorylated form (FMN). It bypasses the initial step of digestion and is more readily converted into the critical FAD cofactor.
- —Dosage: For MTHFR 677TT individuals, studies suggest a minimum of 10mg to 50mg per day to maintain enzyme saturation, far exceeding the UK RDA of 1.4mg.
- —The "Bright Yellow" Marker: Do not be alarmed by neon-yellow urine; this is a sign of B2 absorption and clearance. It indicates that the system is saturated.
4. Mitigating Antagonists
- —Switch to Opaque Containers: Ensure milk or plant-based alternatives are stored in light-proof packaging.
- —Review Medications: If on TCAs or the Pill, discuss B2 status with a practitioner.
- —Thyroid Support: Ensure adequate iodine and selenium intake to support the T4-to-B2 conversion process.
Summary: Key Takeaways
The relationship between Riboflavin (B2) and the MTHFR pathway is a cornerstone of human health that has been marginalised by a medical establishment focused on synthetic folate and pharmaceutical intervention.
- —The MTHFR enzyme is a flavoprotein; it is functionally useless without the B2-derived cofactor FAD.
- —The C677T polymorphism is not a death sentence but a nutritional signal; it increases the "leakage" of FAD, necessitating higher B2 intake to maintain methylation.
- —High Homocysteine is frequently a symptom of B2 deficiency, not just folate or B12 deficiency.
- —Modern lifestyle factors, including light exposure, pharmaceuticals, and the UK’s lack of mandatory B2 fortification in flour, have created a silent epidemic of methylation failure.
- —The solution lies in recognizing the "flavin-dependency" of our genetics. By prioritising bioactive Riboflavin (R5P) and B2-rich whole foods, we can bypass genetic roadblocks, lower homocysteine, and reclaim our neurological and cardiovascular health.
The interference is real, but the biological mechanism for recovery is clear. It is time to restore Riboflavin to its rightful place at the head of the B-vitamin hierarchy. For the "INNERSTANDING" reader, this is more than nutrition; it is the epigenetic reclamation of your biological potential.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Riboflavin (B2) and the MTHFR Pathway Interference"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper