
Rifaximin Resistance: Evaluating the Limitations of the UK's Primary Treatment
While Rifaximin is the NICE-approved standard for SIBO, its efficacy is often short-lived if the underlying motility cause is ignored. We examine why antibiotic monotherapy frequently fails in the long-term clinical setting.
Overview
The landscape of gastroenterology in the United Kingdom has, for the last decade, been dominated by a single pharmacological protagonist: Rifaximin. Marketed under brand names such as Targaxan and Xifaxan, this non-systemic antibiotic has been heralded as a "smart drug" for the small intestine, specifically targeted at Small Intestinal Bacterial Overgrowth (SIBO) and Irritable Bowel Syndrome with Diarrhoea (IBS-D). Under the National Institute for Health and Care Excellence (NICE) guidelines, it remains the primary, and often only, tool in the NHS arsenal for addressing the microbial imbalances that plague millions of British citizens.
However, a growing body of clinical evidence and a mounting chorus of disillusioned patients suggest that the mainstream narrative—that SIBO is a simple infection to be "cleared"—is fundamentally flawed. While Rifaximin is undeniably effective at reducing the absolute bacterial load within the *lumen* of the small intestine, its efficacy is frequently ephemeral. For many, the completion of a two-week course marks not the end of their journey, but the beginning of a cycle of relapse. This cycle highlights a critical misunderstanding of intestinal ecology: we are treating the "smoke" of bacterial overgrowth while the "fire" of physiological dysfunction continues to burn.
The primary limitation of Rifaximin lies not necessarily in the drug’s chemical potency, but in its application as a monotherapy. In the UK's clinical setting, the focus is almost entirely on the eradication of bacteria, ignoring the underlying failures of the Migrating Motor Complex (MMC), the protective mechanisms of gastric acid, and the intricate signaling of the enteric nervous system. When we evaluate "resistance," we must look beyond traditional microbiological definitions. We are witnessing a clinical resistance, where the drug remains effective at killing bacteria in a petri dish, but fails to provide a long-term cure because the host environment remains an open invitation for reinvasion.
In the UK, approximately 20% to 30% of the population experience symptoms consistent with IBS, yet it is estimated that up to 80% of these cases may actually be undiagnosed or poorly managed SIBO. Despite the widespread use of Rifaximin, relapse rates are reported to be as high as 40% within the first three months post-treatment.
This article serves as an exhaustive evaluation of Rifaximin’s role in modern SIBO management. We will dissect its molecular behaviour, its impact on the gut-liver axis, and the biological "blind spots" that allow SIBO to persist despite aggressive antibiotic intervention.
##
The Biology — How It Works
To understand why Rifaximin fails, we must first understand how it is designed to work. Rifaximin is a semi-synthetic derivative of Rifamycin, an antibiotic class that works by inhibiting bacterial protein synthesis. What distinguishes Rifaximin from its cousins, such as Rifampicin, is its unique chemical structure—specifically the addition of a pyrido-imidazo ring.
This structural modification renders the molecule virtually insoluble in water and prevents it from being absorbed through the intestinal lining into the bloodstream. In a standard clinical dose, less than 0.4% of the drug enters systemic circulation. This is the cornerstone of its clinical appeal: it stays where the problem is—the gut—and spares the rest of the body from the side effects typically associated with systemic antibiotics, such as nephrotoxicity or systemic yeast overgrowth.
The Bile-Dependent Catalyst
Rifaximin is a bile-dependent antibiotic. It requires the presence of bile acids to become "activated" or, more accurately, to become soluble enough to interact with bacterial cell walls. This is a critical biological detail that is often overlooked in the UK’s standard "one size fits all" dosing. Because bile is primarily released into the duodenum (the first part of the small intestine), Rifaximin is most active in the very area where SIBO is most prevalent.
Once dissolved in bile micelles, Rifaximin targets the bacterial DNA-dependent RNA polymerase (RNAP). It binds to the beta-subunit of this enzyme, effectively jamming the machinery that the bacteria use to transcribe DNA into RNA. Without the ability to produce proteins, the bacteria cannot grow, replicate, or maintain their cellular integrity.
Eubiotic vs. Antibiotic
One of the most fascinating biological aspects of Rifaximin is its supposed "eubiotic" effect. Unlike broad-spectrum antibiotics like Ciprofloxacin or Amoxicillin, which act like a "carpet bomb" to the entire microbiome, Rifaximin appears to be more selective. Studies have shown that it does not significantly deplete the beneficial *Lactobacillus* or *Bifidobacterium* populations in the colon. Instead, it focuses its lethality on the gram-negative and gram-positive aerobes and anaerobes that have migrated from the colon into the small intestine.
However, this selectivity is also its Achilles' heel. By design, Rifaximin is a gentle regulator. If the bacterial overgrowth is entrenched in biofilms—protective "slime cities" built by bacteria to shield themselves—Rifaximin’s gentle approach may be insufficient.
##
Mechanisms at the Cellular Level
At the cellular level, the efficacy of Rifaximin is mediated by more than just bacterial death. It interacts significantly with the host’s own cellular receptors, specifically the Pregnane X Receptor (PXR).
The PXR Pathway: A Double-Edged Sword
The Pregnane X Receptor is a nuclear receptor primarily expressed in the liver and the intestines. When Rifaximin binds to PXR, it initiates a series of anti-inflammatory cascades. It inhibits the activity of Nuclear Factor-kappa B (NF-κB), the master switch for inflammation. By suppressing NF-κB, Rifaximin reduces the production of pro-inflammatory cytokines like TNF-alpha and Interleukin-6 (IL-6).
This explains why many UK patients feel an immediate sense of relief from "brain fog" and systemic fatigue when taking Rifaximin; the drug is actively lowering the inflammatory load of the gut lining. Furthermore, PXR activation helps to maintain the integrity of tight junctions—the proteins that hold the intestinal cells together. In this sense, Rifaximin acts as a temporary "patch" for Leaky Gut (Intestinal Permeability).
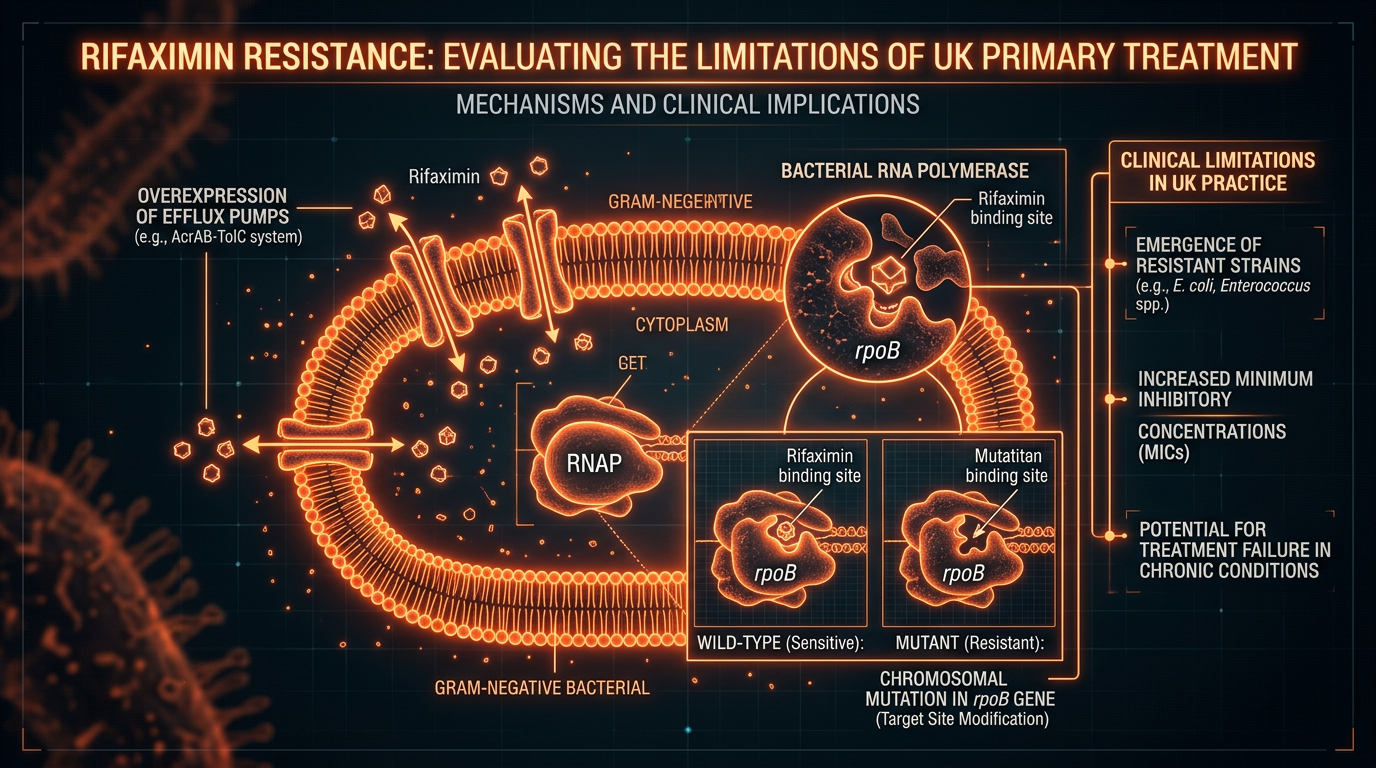
The Problem of Efflux Pumps
The primary mechanism of true bacterial resistance to Rifaximin is the development of efflux pumps. Bacteria are remarkably adaptive organisms. When exposed to Rifaximin, some species, particularly *Acinetobacter* and *Enterobacteriaceae*, can upregulate genes that encode for these pumps. These pumps act like biological sump pumps, actively ejecting the Rifaximin molecule from the bacterial cell before it can reach the RNA polymerase.
Microbiological resistance is often linked to mutations in the rpoB gene, which alters the binding site of Rifaximin. While this is rare in the general population, the repetitive use of Rifaximin—common in the UK due to high relapse rates—provides the evolutionary pressure necessary for these resistant strains to flourish.
Methane-Producing Archaea
Another cellular limitation involves methanogens, such as *Methanobrevibacter smithii*. These are not bacteria, but Archaea—a different kingdom of life altogether. Archaea have different cell wall structures and different RNA polymerase configurations. Consequently, Rifaximin alone is notoriously poor at treating Intestinal Methanogen Overgrowth (IMO), the condition often responsible for stubborn constipation. In the UK, NICE does not currently provide a specific secondary protocol for methane-dominant cases (which usually requires the addition of Neomycin or Metronidazole), leading to a high rate of perceived "Rifaximin failure."
##
Environmental Threats and Biological Disruptors
The efficacy of any SIBO treatment is dictated by the environment of the host. In the modern British context, several environmental and biological disruptors undermine the success of Rifaximin before the patient even takes the first pill.
The PPI Epidemic
Proton Pump Inhibitors (PPIs) like Omeprazole and Lansoprazole are among the most prescribed medications in the UK. By suppressing stomach acid, these drugs remove the body’s first line of defence against bacterial ingestion. Stomach acid is a biological steriliser; without it, every meal introduces a fresh wave of bacteria into the small intestine. Patients taking Rifaximin while remaining on high-dose PPIs are essentially trying to bail out a leaking boat without first plugging the hole.
Glyphosate and Xenobiotics
The British food chain is heavily saturated with xenobiotics, most notably glyphosate (the active ingredient in many herbicides). Glyphosate acts as a selective antibiotic, disrupting the shikimate pathway in beneficial gut bacteria while allowing pathogenic, SIBO-associated species like *Clostridia* to thrive. This environmental pressure creates a "dysbiotic momentum" that Rifaximin must fight against. If the patient’s diet continues to be high in glyphosate-treated grains and processed foods, the microbial terrain will remain skewed toward overgrowth.
Bile Acid Malabsorption (BAM)
As mentioned, Rifaximin requires bile for solubility. However, many SIBO patients suffer from Bile Acid Malabsorption or poor bile flow (cholestasis). If the bile is too thin or the flow is obstructed by a sluggish gallbladder, Rifaximin remains in its crystalline, inactive form. It passes through the small intestine without ever engaging with the bacteria. This is a significant factor in why some patients report zero change in symptoms despite a full course of the medication.
##
The Cascade: From Exposure to Disease
The failure of Rifaximin monotherapy is best understood by looking at the "SIBO Cascade." This is the sequence of events that leads to the disease and, crucially, the sequence that Rifaximin fails to reverse.
- —The Insult: The cascade begins with an insult to the gut—this could be a bout of food poisoning (post-infectious SIBO), chronic stress, or surgery. This insult triggers the production of antibodies (anti-CdtB and anti-vinculin) that attack the Interstitial Cells of Cajal (ICC).
- —The Stasis: The ICC are the pacemakers of the gut. When they are damaged, the Migrating Motor Complex (MMC)—the "cleansing wave" that occurs between meals—is impaired.
- —The Accumulation: Without the MMC, the small intestine becomes a stagnant pond. Debris, undigested food, and bacteria from the colon begin to accumulate.
- —The Fermentation: Bacteria ferment these food particles, producing gases (hydrogen, methane, hydrogen sulphide) that cause bloating and pain.
- —The Rifaximin Intervention: The patient takes Rifaximin. The bacteria are killed. The gas levels drop. The patient feels better.
- —The Relapse: Rifaximin does nothing to repair the Interstitial Cells of Cajal or the MMC. Within weeks of stopping the antibiotic, the "stagnant pond" begins to fill up again. Because the underlying motility is still broken, the bacteria return.
This cascade demonstrates that Rifaximin is an interruption, not a cure. In the UK, the clinical focus ends at step 5. The "Truth" that the mainstream narrative omits is that without addressing the motility failure in step 2, the patient is destined for a lifetime of Rifaximin dependence.
##
What the Mainstream Narrative Omits
The mainstream medical narrative in the UK, reinforced by pharmaceutical marketing and simplified clinical pathways, omits several critical truths about SIBO and its treatment.
The Myth of Non-Resistance
The pharmaceutical industry often claims that "resistance does not develop to Rifaximin." This is a semantic trick. While *systemic* resistance (the kind that would make an ear infection untreatable) is rare, local microbial adaptation is well-documented. Bacteria can hide in the mucosal layer or within biofilms where Rifaximin concentrations are lower than the minimum inhibitory concentration (MIC). This allows a sub-population of "persister cells" to survive and recolonise the gut as soon as the treatment ends.
The Importance of the "Kill Phase" vs. the "Repair Phase"
NICE guidelines focus almost exclusively on the "Kill Phase." There is virtually no mention of the "Repair Phase" (healing the gut lining) or the "Prokinetic Phase" (stimulating the MMC). By ignoring these phases, the NHS is effectively providing half a treatment. A senior biological researcher would argue that treating SIBO without a prokinetic is like mopping the floor while the tap is still running.
The Hydrogen Sulphide Blind Spot
Standard NHS breath tests (when they are even available) typically only measure Hydrogen and Methane. They completely miss Hydrogen Sulphide (H2S) SIBO. Rifaximin has limited efficacy against H2S-producing bacteria like *Desulfovibrio*. Patients with this variant often experience severe symptoms but are told their "test is negative," leading to a dismissal of their condition and a failure of standard Rifaximin protocols.
##
The UK Context
The United Kingdom presents a unique set of challenges for the SIBO sufferer. The NHS is a "top-down" system, governed by NICE TA442, which approved Rifaximin for the treatment of IBS-D. However, the path to obtaining this treatment is fraught with bureaucratic and diagnostic hurdles.
The Postcode Lottery
Access to SIBO breath testing in the UK is a "postcode lottery." Some trusts provide lactulose breath testing (LBT), while others rely solely on the Rome IV criteria for IBS, which is a symptom-based diagnosis that does not differentiate between motility issues, microbial overgrowth, or food intolerances. Consequently, many patients are prescribed Rifaximin without a confirmed SIBO diagnosis, while others with clear SIBO are denied it because they don't meet the "IBS-D" criteria.
The Cost of "Whack-a-Mole" Medicine
A single course of Targaxan (Rifaximin) costs the NHS roughly £260-£300. When patients relapse 3 or 4 times a year, the cost becomes significant. Yet, the system remains resistant to funding prokinetic medications like Prucalopride or specialized nutritional therapy, which could prevent the need for repeat antibiotic courses. This is "Whack-a-Mole" medicine—hitting the symptom as it pops up rather than dismantling the machine that produces it.
Statistics from UK-based private laboratories suggest that over 60% of patients seeking private SIBO testing have already undergone at least one round of Rifaximin through the NHS, indicating a systemic failure in long-term resolution.
##
Protective Measures and Recovery Protocols
If Rifaximin is to be used effectively, it must be part of a comprehensive biological strategy. As a senior researcher, I propose that the limitations of Rifaximin can be mitigated by surrounding the "Kill Phase" with protective and restorative measures.
1. Biofilm Disruptors
Before and during Rifaximin treatment, patients should utilise biofilm disruptors. Substances like Bismuth, Alpha-Lipoic Acid, and N-Acetyl Cysteine (NAC) can help break down the protective matrices that bacteria build. By exposing the bacteria, we make them significantly more vulnerable to Rifaximin’s RNA polymerase inhibition.
2. Bile Support
To ensure Rifaximin becomes soluble, bile flow must be optimised. This can be achieved through the use of TUDCA (Tauroursodeoxycholic acid), ox bile supplements, or bitter herbs (like Dandelion root and Gentian) taken before meals. Ensuring that Rifaximin is taken with a small amount of fat can also trigger the gallbladder to release the bile necessary for the drug’s activation.
3. The Prokinetic Mandate
The most critical protective measure is the immediate introduction of a prokinetic following the completion of Rifaximin. In the UK, this might include:
- —Pharmaceuticals: Low-dose Prucalopride (Resolor) or Erythromycin.
- —Natural Agents: High-dose Ginger root and Artichoke leaf extract.
These agents stimulate Phase III of the Migrating Motor Complex, ensuring that the bacteria killed by Rifaximin are actually swept out of the small intestine and into the colon where they belong.
4. Vagus Nerve Optimisation
The MMC is under the control of the Enteric Nervous System, which communicates with the brain via the Vagus Nerve. Chronic stress—a staple of modern British life—shuts down Vagus Nerve activity, halting the MMC. Recovery protocols must include Vagal stimulation, whether through deep breathing, cold exposure, or gargling, to ensure the "gut-brain" signal is strong enough to maintain motility.
5. Phased Nutrition
The "Low FODMAP" diet is often used in the UK to manage symptoms, but it is not a cure. In fact, long-term Low FODMAP dieting can starve beneficial bacteria in the colon. A more biological approach is the Bi-Phasic Diet, which uses a strict fermentable-fibre-free phase during the Rifaximin "Kill" period, followed by a gradual reintroduction to "feed" the remaining healthy flora and test the resilience of the MMC.
##
Summary: Key Takeaways
The evaluation of Rifaximin resistance in the UK reveals a profound gap between clinical guidelines and biological reality. While Rifaximin is a sophisticated and relatively safe tool, its failure as a monotherapy is predictable based on the mechanics of intestinal motility.
- —Rifaximin is a "Cleanser," not a "Fixer": It effectively reduces bacterial numbers but does nothing to address the underlying cause of stasis (MMC failure).
- —Microbiological vs. Clinical Resistance: While true genetic resistance is slow to emerge, clinical resistance—where symptoms return because the environment remains unchanged—is rampant.
- —The PXR Connection: Rifaximin's benefit is partly due to its anti-inflammatory effects on the host, which may mask the fact that the bacteria have not been fully eradicated.
- —The Necessity of a "Systems Approach": Successful treatment requires the integration of biofilm disruptors, bile support, and, most importantly, post-treatment prokinetics.
- —UK Clinical Reform: There is an urgent need for the NHS to move beyond the "Kill-only" paradigm and include prokinetic support and comprehensive breath testing (including Methane and H2S) in standard care.
For the SIBO sufferer in the UK, the path to health lies in understanding that Rifaximin is merely a window of opportunity. It clears the path, but the patient and the practitioner must do the work to ensure the path stays clear. We must stop viewing SIBO as an "infection" to be eradicated and start viewing it as a functional failure to be rehabilitated. Only then will we break the cycle of relapse and move toward true intestinal eubiosis.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Rifaximin Resistance: Evaluating the Limitations of the UK's Primary Treatment"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper
