The PCOS Myth: Endocrine Disruptors vs Genetics
Polycystic Ovary Syndrome is often treated as a genetic inevitability rather than a response to environmental xenoestrogens. We dissect how the NHS overlooks chemical triggers in cosmetic and food supplies.
Overview
For decades, the medical establishment has categorised Polycystic Ovary Syndrome (PCOS) as a mysterious, primarily genetic, and incurable chronic condition. Affecting an estimated 1 in 10 women in the United Kingdom, it is the leading cause of female infertility and a significant precursor to Type 2 diabetes and cardiovascular disease. Yet, despite its prevalence, the clinical approach remains stubbornly archaic. Patients are routinely told that their ovaries are "faulty," their weight gain is a personal failure of "willpower," and their only recourse is a lifetime of hormonal contraceptives and Metformin.
At INNERSTANDING, we challenge this reductionist perspective. The "PCOS Myth" is the notion that this condition is a hard-wired genetic destiny. Emerging biological research suggests a more sinister reality: PCOS is, in many cases, an environmental "phenocopy"—a physiological state that mimics a genetic disorder but is actually triggered by chronic exposure to Endocrine Disrupting Chemicals (EDCs) and xenoestrogens.
The National Health Service (NHS), hamstrung by outdated diagnostic guidelines and a lack of integrated toxicological screening, continues to treat the symptoms while ignoring the chemical catalyst. We are witnessing a massive misdiagnosis pattern where the "polycystic" morphology is merely a symptom of a system overwhelmed by synthetic oestrogens, phthalates, and bisphenols. This article provides a deep dive into the molecular mechanics of how our environment is re-engineering female biology.
Fact: Research indicates that women with PCOS have significantly higher blood levels of Bisphenol A (BPA) compared to those without the condition, suggesting that environmental exposure is not a background factor, but a primary driver of the disease state.
---
The Biology — How It Works
To understand why the genetic narrative is insufficient, one must first understand the delicate orchestration of the female endocrine system. PCOS is traditionally defined by the Rotterdam Criteria, which requires two out of three symptoms for diagnosis: irregular or absent periods (anovulation), clinical or biochemical signs of high androgens (hyperandrogenism), and the presence of "cysts" (undeveloped follicles) on the ovaries.
The HPO Axis: The Master Conductor
The female reproductive cycle is governed by the Hypothalamic-Pituitary-Ovarian (HPO) axis. The hypothalamus releases Gonadotropin-Releasing Hormone (GnRH) in specific pulses. These pulses signal the pituitary gland to release Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH).
In a healthy system:
- —FSH stimulates the growth of ovarian follicles during the first half of the cycle.
- —LH triggers the final maturation and release of the egg (ovulation).
- —Oestrogen and Progesterone provide feedback to the brain to keep the system in balance.
The PCOS Breakdown
In the "PCOS" state, this pulse frequency is disrupted. The pituitary gland begins to over-produce LH relative to FSH. This high LH-to-FSH ratio prevents the follicles from maturing properly. Instead of one egg being released, dozens of follicles begin to grow but then "arrest" in a half-developed state, appearing as "cysts" on an ultrasound.
Furthermore, these arrested follicles and the surrounding theca cells produce excessive amounts of testosterone and androstenedione. This hyperandrogenism creates the hallmark symptoms: acne, hirsutism (excessive hair growth), and thinning scalp hair.
The missing link in the mainstream narrative is *why* this axis becomes deranged. While genetics can predispose a woman to sensitivity, the trigger is increasingly identified as the presence of exogenous chemicals that "hijack" these hormonal receptors, tricking the brain into thinking it is permanently in a state of high oestrogen or high insulin.
---
Mechanisms at the Cellular Level
The "Genetic Myth" falls apart when we look at the molecular interface. PCOS is not a flaw in the DNA sequence; it is a flaw in signal transduction.
Oestrogen Receptor Alpha and Beta (ERα/ERβ)
Xenoestrogens (foreign oestrogens) found in plastics and cosmetics are structurally similar enough to natural 17β-oestradiol that they can bind to oestrogen receptors. However, unlike natural hormones, they often bind with different affinities or "jam" the receptor in the "on" position.
- —ERα is primarily involved in the proliferative effects of oestrogen.
- —ERβ often acts as a counterbalance.
EDCs frequently show a preference for one over the other, leading to a state of oestrogen dominance even when blood tests show "normal" levels of endogenous hormones.
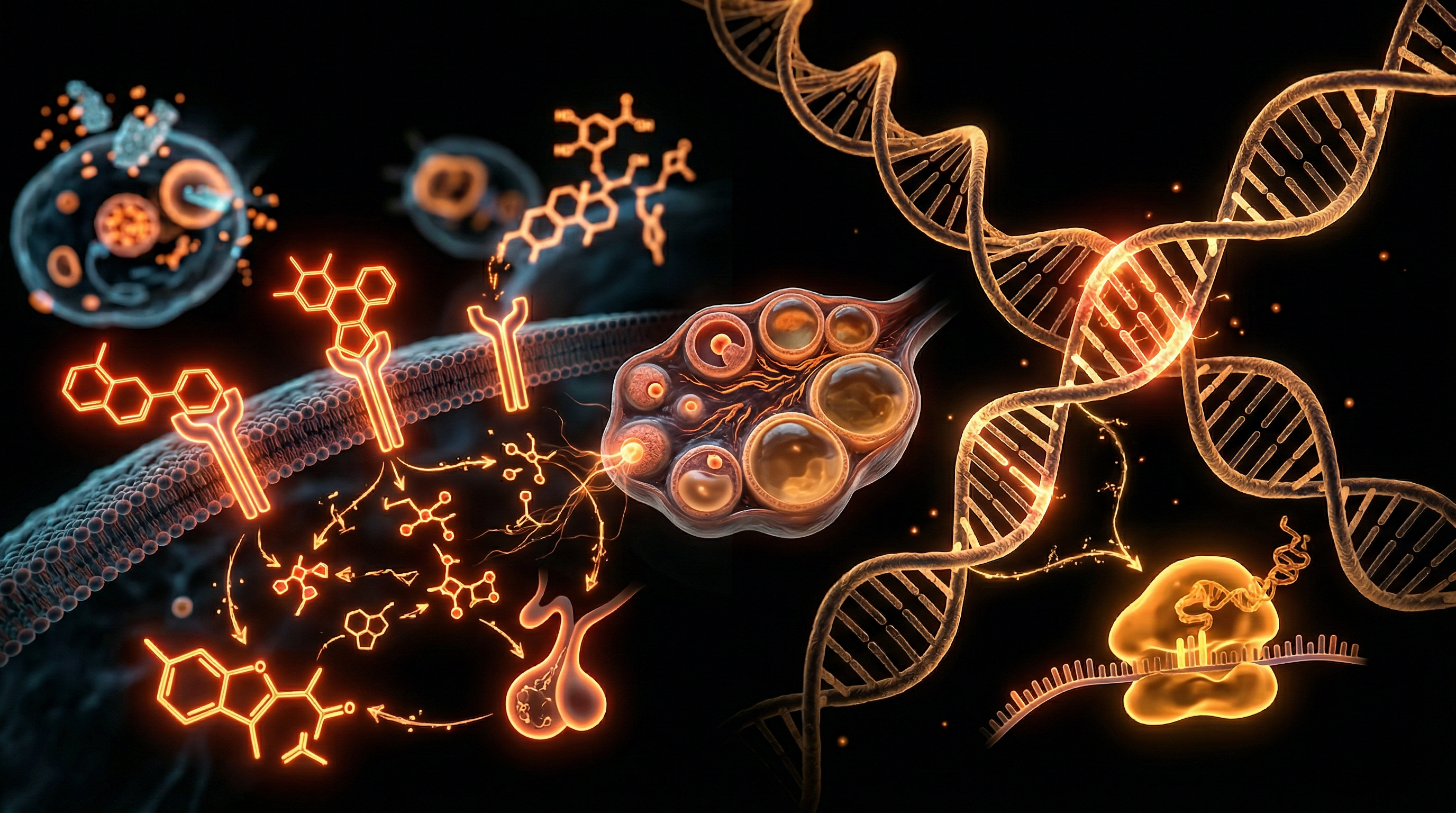
The Insulin Receptor and GLUT4
A critical component of PCOS is Insulin Resistance. The NHS often treats this as a byproduct of obesity. However, cellular biology shows that EDCs like phthalates can interfere with the IRS-1 (Insulin Receptor Substrate 1) pathway. When this pathway is blocked, the cell cannot move GLUT4 (the glucose transporter) to its surface. The result? Glucose stays in the blood, and the pancreas pumps out more insulin. High levels of insulin are directly toxic to the ovaries; insulin acts as a "co-gonadotropin," stimulating the theca cells to produce even more testosterone. This creates a vicious cycle that has nothing to do with genetic coding and everything to do with chemical interference in cellular signalling.
Mitochondrial Dysfunction and Oxidative Stress
Recent proteomic studies have shown that the mitochondria within the ovarian follicles of women with PCOS are often dysfunctional. They produce excessive Reactive Oxygen Species (ROS). This oxidative stress damages the delicate machinery of the oocyte (egg). EDCs are known mitochondrial poisons; they disrupt the Electron Transport Chain, leading to a cellular "energy crisis" that manifests as the fatigue and "brain fog" so common in PCOS patients.
---
Environmental Threats and Biological Disruptors
We live in a "chemical soup" that our ancestors never encountered. The rapid rise in PCOS cases over the last 40 years mirrors the explosion of synthetic chemicals in our daily lives. These are not mere pollutants; they are Metabolic Disruptors.
Bisphenols (BPA, BPS, BPF)
Found in the lining of tin cans, thermal till receipts, and hard plastics, Bisphenol A is a potent xenoestrogen. Even "BPA-free" products often use BPS, which research shows is equally, if not more, disruptive to the endocrine system. BPA has been shown to interfere with the aromatase enzyme, which is responsible for converting androgens into oestrogens. When aromatase is inhibited by BPA, androgens build up, leading to the "male-pattern" symptoms of PCOS.
Phthalates
Used to make plastics flexible and as fixatives in fragrances, phthalates are ubiquitous in the UK high street. They are found in shampoos, perfumes, and food packaging. Phthalates are known to decrease the expression of genes required for oestrogen synthesis while simultaneously increasing the expression of genes for androgen synthesis.
PFAS (Per- and Polyfluoroalkyl Substances)
Known as "Forever Chemicals," PFAS are used in non-stick cookware and water-resistant clothing. These chemicals are structurally similar to fatty acids and can interfere with PPAR (Peroxisome Proliferator-Activated Receptors), which govern fat metabolism and insulin sensitivity. Exposure to PFAS is strongly correlated with a higher risk of developing the metabolic markers of PCOS.
Parabens and UV Filters
Commonly found in sunscreens and "moisturising" creams, chemicals like Methylparaben and Oxybenzone have been detected in the follicular fluid of women undergoing IVF. Their presence in the very environment where an egg matures suggests a direct path of contamination that no "genetic" theory can explain.
---
The Cascade: From Exposure to Disease
The progression from environmental exposure to a clinical diagnosis of PCOS follows a predictable, yet often ignored, biological cascade. This is not an overnight occurrence but the result of bioaccumulation and synergistic toxicity.
Stage 1: The First Hit (Developmental Priming)
The "PCOS Myth" is often reinforced by the fact that the condition can appear in very young women. However, research into fetal programming shows that if a mother is exposed to high levels of EDCs during pregnancy, the female foetus undergoes "epigenetic remodeling." The developing ovaries are "primed" to be hyper-responsive to androgens. This is not a genetic mutation; it is an environmental imprint.
Stage 2: Chronic Low-Dose Exposure
Throughout childhood and puberty, the individual is exposed to a constant barrage of xenoestrogens through:
- —Microplastics in bottled water.
- —Pesticide residues (such as glyphosate) on produce.
- —Synthetic fragrances in household cleaning products.
This constant "background noise" of oestrogen-mimics prevents the HPO axis from ever establishing a healthy rhythm.
Stage 3: The Metabolic Tipping Point
As the liver becomes overwhelmed by the task of detoxifying these synthetic compounds (a process involving Phase I and Phase II detoxification), the body's hormonal clearance slows down.
Scientific Note: The liver uses the cytochrome P450 enzyme system to break down hormones. EDCs compete for these same enzymes. If the liver is busy processing parabens from your lotion, it cannot efficiently clear your body's own oestrogen, leading to "re-circulation" of hormones and the subsequent disruption of the menstrual cycle.
Stage 4: Follicular Arrest and Hyperinsulinaemia
The culmination of this chemical load is the clinical manifestation of PCOS. The ovaries, under the dual pressure of high insulin (from phthalate-induced resistance) and high LH (from xenoestrogen-induced feedback loops), stop ovulating. The follicles "stall," and the androgen-producing machinery goes into overdrive.
---
What the Mainstream Narrative Omits
The NHS and major medical bodies continue to treat PCOS as a management-based condition rather than a resolvable one. This narrative omits several critical truths that challenge the pharmaceutical status quo.
The Failure of the "Weight Loss" Mantra
The most common advice given to UK patients is: "Lose weight, and your symptoms will improve." This is a classic case of confusing cause and effect. In the context of EDCs, weight gain is often a protective mechanism. Many EDCs are lipophilic, meaning they are stored in fat tissue. The body may create and hold onto fat cells to sequester these toxins away from vital organs. When a woman is told to "just eat less," she is fighting a biological survival mechanism triggered by chemical toxicity, not a lack of discipline.
The Contraceptive "Band-Aid"
The Combined Oral Contraceptive Pill (COCP) is the "gold standard" NHS treatment. While it creates a regular "bleed," it does not create a cycle. It functions by shutting down the HPO axis entirely. It masks the symptoms while the underlying environmental drivers—the insulin resistance and the chemical load—continue to worsen. Furthermore, some progestins used in the pill are actually androgenic, potentially exacerbating the issues once the patient ceases the medication.
The Absence of Toxicological Screening
Why does the NHS not test for BPA or phthalate levels in PCOS patients? The answer is twofold: cost and paradigm inertia. Routine toxicology is expensive, and the current medical model is built on "one pill for one ill." Acknowledging that PCOS is an environmental toxicity issue would require a radical overhaul of public health policy, food regulation, and the cosmetic industry—a shift the establishment is not yet ready to make.
---
The UK Context
In the United Kingdom, the PCOS epidemic is compounded by specific national factors that are rarely discussed in the GP's surgery.
The "Forever Chemical" Water Crisis
Recent investigations have shown that UK tap water frequently contains levels of PFAS and nitrates that exceed safety guidelines recommended by independent scientists. The UK's ageing water filtration infrastructure is not designed to remove endocrine-disrupting micro-pollutants. For a woman predisposed to hormonal sensitivity, her morning glass of water may be contributing to her anovulation.
The Post-Brexit Regulatory Gap
Since leaving the European Union, there are significant concerns regarding the UK's version of REACH (Registration, Evaluation, Authorisation and Restriction of Chemicals). There is a risk that the UK will fall behind the EU in banning known endocrine disruptors in consumer goods, leaving British women as "canaries in the coal mine" for chemicals already restricted on the continent.
The Ultra-Processed Food (UPF) Dominance
The UK has one of the highest consumptions of ultra-processed foods in Europe. UPFs are not just high in sugar; they are high in emulsifiers and plasticisers leached from industrial processing equipment. This combination creates a "perfect storm" for insulin resistance—the primary driver of ovarian androgen production.
Statistic: Over 50% of the UK diet consists of ultra-processed foods, which have been linked in multiple studies to increased rates of endocrine disorders and metabolic syndrome in women.
---
Protective Measures and Recovery Protocols
If PCOS is an environmental response rather than a genetic sentence, then recovery is possible through the systematic removal of triggers and the support of the body's natural detoxification pathways.
1. Eliminate the "Big Three" EDCs
- —Fragrance: Switch to "fragrance-free" or essential-oil-based products. "Parfum" on a label is a loophole for thousands of undisclosed phthalates.
- —Plastics: Never heat food in plastic. Switch to glass or stainless steel for water bottles and food storage. Avoid BPA-lined tins; look for "BPA-NI" (Non-Intent) labels.
- —Personal Care: Audit your "daily dozen." The average woman applies 126 unique chemicals to her skin before leaving the house. Use databases like EWG or "Think Dirty" to find clean alternatives for shampoos, deodorants, and makeup.
2. Support Hepatic Clearance
The liver must clear both internal hormones and external xenoestrogens.
- —Cruciferous Vegetables: Broccoli, kale, and Brussels sprouts contain Indole-3-Carbinol (I3C) and Sulforaphane, which support Phase II liver detox and the healthy metabolism of oestrogen into the "good" 2-hydroxyoestrone pathway.
- —Calcium D-Glucarate: This supplement prevents "beta-glucuronidase"—an enzyme produced by gut bacteria—from "un-zipping" detoxified oestrogens and sending them back into the bloodstream.
3. Sensitise the Insulin Receptor
Instead of relying solely on Metformin, focus on biological sensitisers:
- —Myo-Inositol & D-Chiro Inositol: Research shows a 40:1 ratio of these isomers can be as effective as Metformin for improving ovulation and reducing androgens, with zero side effects.
- —Magnesium: Magnesium is a cofactor for over 300 enzymatic reactions, including the binding of insulin to its receptor. Most UK adults are chronically deficient.
4. Water and Air Filtration
Invest in a high-quality water filter (Reverse Osmosis or multi-stage carbon) that specifically targets PFAS and hormones. Ensure your living space is well-ventilated to reduce the inhalation of flame retardants and volatile organic compounds (VOCs) from furniture and carpets.
---
Summary: Key Takeaways
The conventional understanding of PCOS as a genetic lottery is a myth that serves the pharmaceutical industry while failing the patient. By shifting the perspective from "faulty genes" to "environmental response," we empower women to take control of their health.
- —PCOS is a Functional Disorder: It is a systemic response to a signal-heavy environment. The ovaries are not "broken"; they are reacting to the chemical and insulin signals they are receiving.
- —EDCs are the Hidden Drivers: Xenoestrogens like BPA and phthalates bypass the body’s natural regulation, creating a state of hormonal chaos that mimics genetic PCOS.
- —The NHS Model is Insufficient: Current UK protocols focus on symptom suppression (the Pill) rather than address the underlying toxicological and metabolic triggers.
- —Detoxification is Recovery: By reducing the "body burden" of EDCs and supporting the liver and gut, women can often restore natural ovulation and reverse the metabolic markers of the condition.
The path forward for women’s health in the UK must include an "Environmental First" approach. We must stop asking why women’s bodies are failing and start asking what our environment is doing to them. Only then can we move beyond the PCOS myth and toward true biological sovereignty.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The PCOS Myth: Endocrine Disruptors vs Genetics"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper