
Thyroid Physiology: The Metabolic Master Switch
Thyroid hormone physiology extends far beyond simple TSH and T4 measurement — the conversion of inactive T4 to biologically active T3 by the deiodinase enzyme family, the binding of T3 to nuclear receptors that alter gene expression across every cell type, and the role of reverse T3 as a metabolic brake during physiological stress represent layers of regulation that standard NHS thyroid panels completely miss. Mercury, cadmium, and organochlorine pesticides directly inhibit deiodinase enzymes, creating a state of functional hypothyroidism even with normal circulating T4 levels. Fluoride's competition with iodine at the sodium-iodide symporter further impairs T4 synthesis, contributing to the widespread subclinical hypothyroidism the NHS diagnoses as depression, fatigue, and weight problems.
Overview
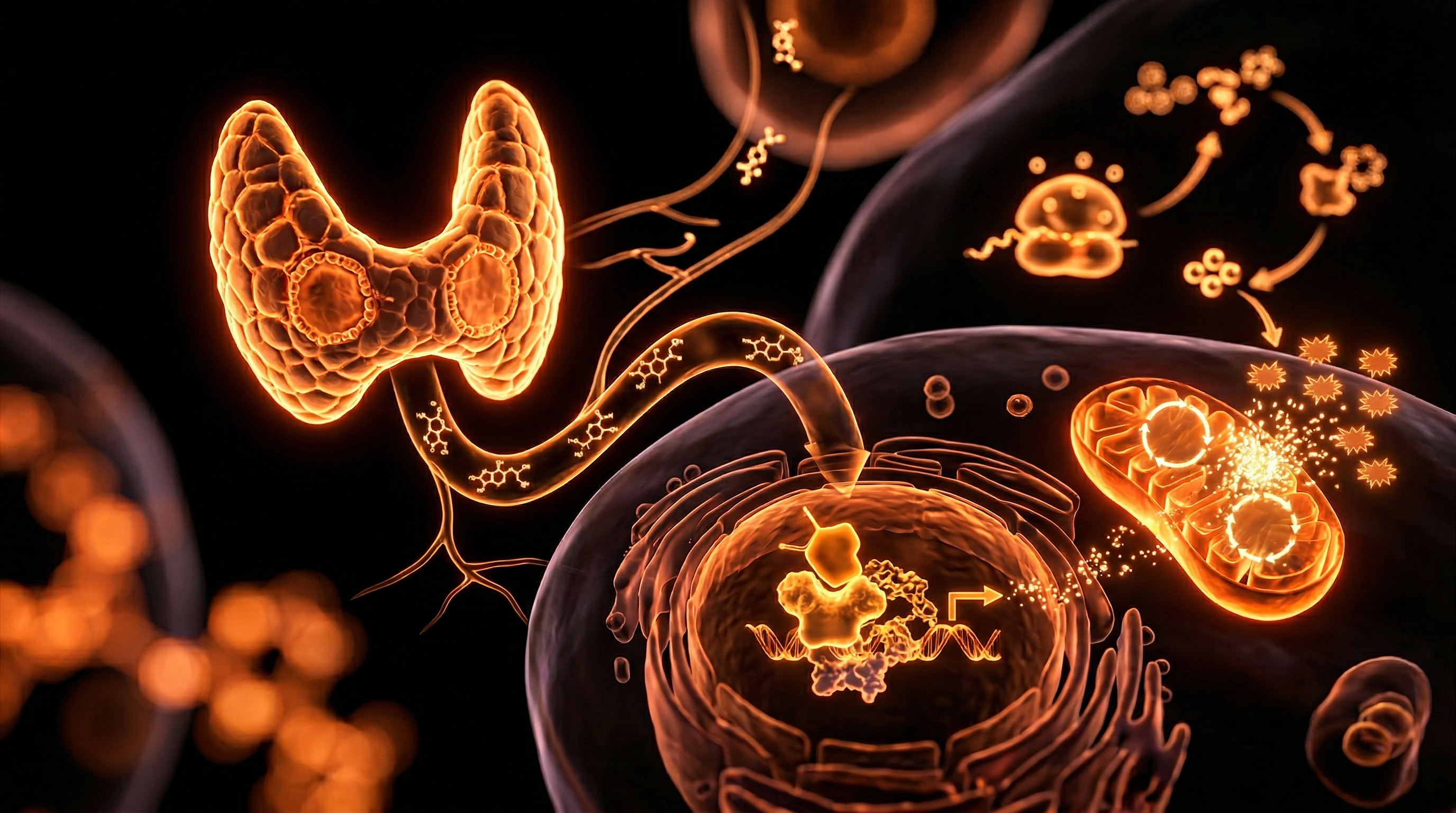
The thyroid gland, a butterfly-shaped endocrine organ nestled at the base of the neck, is frequently reduced in mainstream medical discourse to a simple thermostat. In the standard clinical model, the thyroid is perceived as a binary system: it is either 'on' (euthyroid), 'too high' (hyperthyroid), or 'too low' (hypothyroid), with the Thyroid Stimulating Hormone (TSH) serving as the definitive arbiter of its function. This reductionist view is not merely a simplification; it is a profound biological oversight that leaves millions of patients in the United Kingdom suffering from debilitating symptoms while being told their blood results are "normal."
At INNERSTANDING, we recognise the thyroid for what it truly is: the Metabolic Master Switch. It is the central processing unit of the body’s bioenergetic economy. Every single cell in the human body—from the neurons in the prefrontal cortex to the myocytes in the heart and the hepatocytes in the liver—possesses receptors for thyroid hormone. This system dictates the rate of oxygen consumption, the burning of fuel for heat (thermogenesis), the synthesis of proteins, and the sensitivity of the body to other hormones like adrenaline and cortisol.
The biological reality is that thyroid health is not determined by what the gland produces, but by what the cells receive. The journey from the production of raw Prohormone T4 (Thyroxine) to the delivery of the biologically active T3 (Triiodothyronine) into the nucleus of a cell involves a complex gauntlet of enzymatic conversions, transport proteins, and mineral-dependent catalysts. This article exposes the hidden layers of thyroid physiology—the deiodinase system, the mitochondrial intersection, and the silent interference of environmental toxins—that the NHS and the global medical establishment continue to ignore.
##
##
The Biology — How It Works
To understand the failure of modern diagnostics, one must first master the intricate dance of the Hypothalamic-Pituitary-Thyroid (HPT) Axis. This feedback loop begins in the brain, where the hypothalamus monitors circulating levels of thyroid hormone. When levels are perceived as low, it releases Thyrotropin-Releasing Hormone (TRH), which signals the anterior pituitary gland to secrete TSH.
The Synthesis of Hormone
Inside the thyroid gland, the process of hormone synthesis is a feat of biological engineering. It requires two primary raw materials: the amino acid Tyrosine and the mineral Iodine.
- —Iodine Trapping: The thyroid must concentrate iodine at levels hundreds of times higher than those found in the blood. This is achieved via the Sodium-Iodide Symporter (NIS), a protein pump in the follicular cell membrane.
- —Organification: Once inside, the enzyme Thyroid Peroxidase (TPO) oxidises the iodide and attaches it to a large scaffold protein called Thyroglobulin.
- —Coupling: TPO then 'couples' these iodinated tyrosine residues to form T4 (which contains four iodine atoms) and a small amount of T3 (which contains three).
Fact: While the thyroid gland is the sole producer of T4, it only produces about 20% of the body's required T3. The remaining 80% must be generated in peripheral tissues through the removal of a single iodine atom from T4.
The Transport Myth
Once secreted into the bloodstream, thyroid hormones do not float freely. More than 99% of T4 and T3 are bound to carrier proteins, primarily Thyroxine-Binding Globulin (TBG). These hormones are biologically 'locked' while bound. Only the 'Free' portions—Free T4 (FT4) and Free T3 (FT3)—are capable of entering cells to exert metabolic influence. The mainstream focus on "Total T4" often misses the reality of how much hormone is actually available to the tissues.
##
##
Mechanisms at the Cellular Level
The most critical aspect of thyroid physiology occurs not in the blood, but inside the cytoplasm and nucleus of the target cells. This is where the Deiodinase Enzyme Family acts as the gatekeeper of metabolism. These enzymes are selenoproteins, meaning they require the trace element Selenium to function. Without selenium, the entire metabolic switchboard malfunctions.
The Three Deiodinases: The Logic Gates
- —Type 1 Deiodinase (D1): Located primarily in the liver and kidneys, D1 is responsible for the majority of T4 to T3 conversion that ends up in the systemic circulation. It is highly sensitive to oxidative stress and toxic load.
- —Type 2 Deiodinase (D2): Found in the brain, pituitary, and brown adipose tissue, D2 is the "local" converter. It ensures that the brain has adequate T3 even when systemic levels might be fluctuating. Crucially, the pituitary uses D2 to sense T3 levels; if D2 is working well in the pituitary but D1 is suppressed in the liver, TSH will appear "normal" even if the rest of the body is starving for T3.
- —Type 3 Deiodinase (D3): This is the "metabolic brake." D3 converts T4 into Reverse T3 (rT3), an isomer that is biologically inactive. It also breaks down active T3 into T2. Under conditions of stress, illness, or toxicity, the body upregulates D3 to intentionally slow down metabolism—a state known as Non-Thyroidal Illness Syndrome (NTIS) or "euthyroid sick syndrome."
Nuclear Activation and Gene Expression
Once Free T3 enters the cell, it must cross the nuclear membrane and bind to Thyroid Hormone Receptors (TRα and TRβ). These receptors are already sat upon specific sequences of DNA known as Thyroid Response Elements (TREs).
When T3 binds, it triggers a conformational change that kicks off "corepressor" molecules and recruits "coactivator" molecules. This initiates the transcription of genes that control:
- —Mitochondrial Biogenesis: Increasing the number and efficiency of mitochondria.
- —Na+/K+-ATPase Pumps: The "battery" of the cell, which consumes up to 30% of total cellular energy.
- —Beta-Adrenergic Receptors: Increasing the body's sensitivity to fat-burning signals.
Biological Truth: If T3 cannot bind to its nuclear receptor—due to competition from toxins or lack of cofactors like Vitamin A and Zinc—the patient will exhibit every symptom of hypothyroidism despite having "perfect" blood levels. This is Cellular Hypothyroidism.
##
##
Environmental Threats and Biological Disruptors
We are currently living in a "thyroid-toxic" environment. The delicate machinery of the thyroid and the deiodinase system is uniquely vulnerable to modern industrial pollutants. These are not merely tangential concerns; they are direct inhibitors of metabolic function.
The Halogen Competition: Fluoride and Bromide
Iodine belongs to the halogen group on the periodic table. Other halogens—Fluoride, Bromide, and Chlorine—possess similar atomic radii and electronegativity. This allows them to competitively inhibit iodine uptake at the Sodium-Iodide Symporter (NIS).
- —Fluoride: Historically used in the early 20th century as a drug to *suppress* overactive thyroids, fluoride is now ubiquitous in UK tap water and dental products. It acts as a potent inhibitor of TPO and the NIS, effectively "starving" the thyroid of iodine.
- —Bromide: Found in "brominated" vegetable oils, some soft drinks, and flame retardants in British carpets and furniture. Bromide is a more aggressive competitor for iodine receptors than fluoride, leading to what is termed "Bromine Dominance."
Heavy Metals: Mercury and Cadmium
Mercury and Cadmium have a devastating affinity for Selenium. Because the deiodinase enzymes (D1, D2) are selenoproteins, they require a selenium atom at their active site to strip the iodine off T4.
- —Mercury (from dental amalgams or predatory fish) binds to selenium with an affinity ten thousand times stronger than oxygen. This "sequesters" selenium, rendering it unavailable for thyroid hormone conversion.
- —Cadmium (from cigarette smoke and industrial runoff) accumulates in the thyroid gland itself, inducing oxidative stress and directly inhibiting TPO activity.
Organochlorine Pesticides and Plasticisers
Compounds such as DDT (and its metabolites), PCBs, and BPA (Bisphenol-A) are structurally similar to thyroid hormones. These "endocrine disruptors" can bind to the thyroid transport proteins (TBG), displacing the actual hormones, or worse, bind to the nuclear TR receptors. When BPA binds to a thyroid receptor, it often acts as an antagonist, blocking the real T3 from turning on the metabolic machinery.
##
##
The Cascade: From Exposure to Disease
The progression from environmental exposure to overt clinical disease is a predictable biological cascade that is frequently mischaracterised by mainstream practitioners.
Phase 1: The Functional Shift
Initial exposure to toxins or chronic stress leads to the upregulation of Type 3 Deiodinase (D3). The body begins to shift its production from active T3 to Reverse T3 (rT3). At this stage, a standard NHS test will show a normal TSH and a normal T4. The patient, however, begins to experience "unexplained" fatigue, cold intolerance, and brain fog. This is the body's defensive attempt to conserve energy in a perceived "toxic environment."
Phase 2: The Compensatory Struggle
As conversion efficiency drops, the pituitary may finally begin to raise TSH to "whip" the thyroid into producing more T4. This is the stage of Subclinical Hypothyroidism. The patient is often told to "wait and see" or is prescribed anti-depressants for their low mood, as their TSH might only be slightly elevated (e.g., 4.5 mIU/L), despite the fact that most healthy individuals have a TSH under 2.0.
Phase 3: Systemic Failure
Eventually, the chronic inhibition of TPO by fluoride and the sequestration of selenium by mercury leads to a collapse in hormone production. Mitochondrial function plummets. Because thyroid hormone is required for the conversion of Cholesterol to Pregnenolone (the "mother" of all steroid hormones), the patient now develops high cholesterol and low sex hormones (Libido loss, PCOS, or Low Testosterone).
Alarming Statistic: Research suggests that up to 15% of the UK population may be living with undiagnosed thyroid dysfunction, largely due to the systemic failure to test for anything beyond TSH.
##
##
What the Mainstream Narrative Omits
The current NHS guidelines for thyroid management are, in the view of many independent researchers, scientifically archaic. The reliance on a single biomarker (TSH) to diagnose a multi-systemic metabolic disorder is a failure of basic physiology.
The TSH Fallacy
TSH is a pituitary hormone, not a thyroid hormone. It reflects the pituitary's *perception* of hormone levels, not the actual tissue status of the rest of the body. Various factors can "falsely" suppress TSH, making a patient look healthy on paper when they are biologically hypothyroid:
- —Chronic Inflammation: Cytokines like TNF-alpha can suppress the pituitary's release of TSH.
- —High Cortisol: Stress-induced cortisol inhibits TRH and TSH secretion.
- —Biotin Supplements: High doses of Biotin (common in hair/nail supplements) can interfere with the TSH assay, leading to artificially low readings.
The Reference Range Problem
In the UK, the "normal" range for TSH is often as wide as 0.5 to 5.0 mIU/L. This range is calculated based on a population that includes elderly individuals and people with undiagnosed thyroid disease. If we look at "optimal" ranges—derived from young, healthy, asymptomatic individuals—the TSH should ideally sit between 0.5 and 1.5. By using an overly broad range, the NHS effectively "normalises" disease.
The Liothyronine (T3) Suppression
Perhaps the most egregious omission is the systematic withdrawal of Liothyronine (T3) medication from the NHS formulary. Based on the flawed assumption that everyone can perfectly convert T4 (Levothyroxine) into T3, the NHS has labelled T3 "not cost-effective." This ignores the millions of people with genetic polymorphisms in their deiodinase genes (such as the DIO2 polymorphism) who *cannot* convert T4 efficiently. These people are left permanently symptomatic on T4-only therapy.
##
##
The UK Context
The UK presents a unique set of challenges for thyroid health. Unlike the United States, where salt is mandatorily iodised, the UK has no such mandate. Historically, the British population received its iodine primarily from dairy products (due to iodine-based cleaners used in milking machinery and iodine supplements in cattle feed). With the rise of "plant-based" milk alternatives (almond, oat, soy), which are often devoid of iodine, a new wave of iodine deficiency is sweeping the nation.
Water Fluoridation and the Postcode Lottery
Large swathes of the UK, including the West Midlands, the North East, and parts of the North West, have their water supplies artificially fluoridated by local authorities. As established, fluoride is a potent anti-thyroid agent. Residents in these areas are being mass-medicated with a substance that directly competes with the iodine required for their metabolic health, with no oversight on individual thyroid status.
Soil Depletion
British soils are notoriously low in selenium. This trace mineral is essential not only for the deiodinase enzymes but also for the production of Glutathione Peroxidase, the enzyme that protects the thyroid gland from the hydrogen peroxide produced during hormone synthesis. Without selenium, the thyroid literally "burns" itself out, leading to the autoimmune condition Hashimoto’s Thyroiditis.
##
##
Protective Measures and Recovery Protocols
Restoring the "Metabolic Master Switch" requires a multi-faceted approach that goes beyond simply taking a pill. It requires the restoration of the biological terrain.
1. Nutritional Fortification
- —Selenium: Supplementing with 200mcg of Selenomethionine or eating 2-3 Brazil nuts daily can provide the necessary catalyst for T4 to T3 conversion.
- —Iodine (The Careful Approach): While essential, iodine must never be introduced in high doses without ensuring adequate selenium levels first. Supplementing iodine alone in a selenium-deficient state can aggravate autoimmune thyroiditis.
- —Zinc and Vitamin A: Both are required for the thyroid hormone receptor to function in the cell nucleus. Without them, T3 is like a key with no lock.
2. Environmental Mitigation
- —Water Filtration: Standard "jug" filters do not remove fluoride. To protect the thyroid, UK residents should invest in Reverse Osmosis (RO) systems or activated alumina filters specifically rated for fluoride removal.
- —Amalgam Management: Those with high mercury loads should consult "biological dentists" who follow the SMART (Safe Mercury Amalgam Removal Technique) protocol to avoid a massive toxic bolus during removal.
- —Halogen Detox: Increasing intake of iodine can help "nudge" bromide and fluoride out of the system, but this should be done under the guidance of a practitioner familiar with the "Bromide Detox" symptoms.
3. Demanding the Full Panel
The educated patient must insist on a full thyroid panel to see the "hidden" biology. This includes:
- —TSH
- —Free T4
- —Free T3 (The most important metabolic marker)
- —Reverse T3 (To check for the 'metabolic brake')
- —TPO and TG Antibodies (To check for autoimmunity)
Scientific Note: The ratio of Free T3 to Reverse T3 is often the most sensitive marker of tissue thyroid status. A low ratio (under 20 when using pg/mL for FT3 and ng/dL for rT3) is a hallmark of functional hypothyroidism.
##
##
Summary: Key Takeaways
- —The Thyroid is a System, Not a Gland: It is a complex network of synthesis, peripheral conversion, and cellular reception.
- —The TSH Test is Incomplete: It fails to account for cellular hypothyroidism, deiodinase inhibition, and rT3 dominance.
- —Environmental Toxins are Real Inhibitors: Fluoride, mercury, and bromide directly sabotage the metabolic machinery.
- —The NHS Model is Flawed: The reliance on T4-only therapy and the suppression of T3 availability leaves millions of patients in a state of chronic, treated illness.
- —Selenium is the Pivot Point: Without this trace mineral, the body cannot convert inactive T4 into the "active" fuel of life, T3.
- —Biological Sovereignty: Understanding these pathways allows the individual to reclaim their metabolic health from a system that is currently designed to overlook the root causes of disease.
The "Metabolic Master Switch" is currently being dimmed by a combination of nutritional deficiency, environmental toxicity, and clinical negligence. Only by exposing these truths can we hope to reignite the bioenergetic fire that defines human vitality.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Thyroid Physiology: The Metabolic Master Switch"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Physiology — products curated by our research team for educational relevance and biological support.

Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin
Rejuvenation Pack – Essential Vitamins and Minerals for Health Restoration
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper
