Latitude and Longevity: The Critical Failure of UK Vitamin D Supplementation Advice
Analyzing why standard NHS guidelines for UVB exposure may be insufficient for Northern European populations.
Overview
The prevailing UK clinical paradigm regarding cholecalciferol (Vitamin D3) is fundamentally misaligned with the photobiological reality of the British Isles. Situated between latitudes 50°N and 60°N, the United Kingdom exists within a permanent state of "Vitamin D Winter" for at least six months of the year. During this period, the solar zenith angle is so oblique that the atmospheric path length of solar radiation results in the near-total attenuation of ultraviolet B (UVB) photons within the 290–315 nm range. Consequently, the cutaneous synthesis of 7-dehydrocholesterol into pre-vitamin D3—the primary evolutionary pathway for human secosteroid production—is rendered physically impossible, regardless of duration of exposure. At INNERSTANDIN, we posit that the current Public Health England (PHE) and Scientific Advisory Committee on Nutrition (SACN) recommendation of 10 micrograms (400 IU) daily represents a reductionist failure that prioritises the mere avoidance of musculoskeletal pathology (such as rickets and osteomalacia) over the optimisation of systemic biological function.
This institutional inertia ignores the vast corpus of peer-reviewed evidence—including seminal analyses in *The Lancet Diabetes & Endocrinology* and *The Journal of Steroid Biochemistry and Molecular Biology*—which underscores the pleiotropic nature of the Vitamin D Receptor (VDR). The VDR is expressed across nearly every tissue in the human body, from the myocardial endothelium to the distal convoluted tubules of the kidney and the complex neural architecture of the prefrontal cortex. Beyond calcium homeostasis, 1,25-dihydroxyvitamin D3 [1,25(OH)2D] acts as a potent epigenetic modulator, influencing the transcription of over 200 genes involved in cytokine regulation, antimicrobial peptide production (such as cathelicidin), and the maintenance of the intestinal barrier.
The failure of UK advice is most evident in its disregard for serum 25(OH)D concentration targets. While the SACN maintains a "sufficiency" threshold of 25 nmol/L, contemporary research suggests that for optimal immune-modulation and the mitigation of chronic inflammatory cascades, a serum nadir of 75–125 nmol/L is required. For the average British adult, achieving these levels through a 400 IU dose is biochemically improbable, particularly in the context of high Body Mass Index (BMI) or increased skin pigmentation, both of which necessitate significantly higher loading and maintenance doses. By adhering to archaic, minimalist guidelines, the UK healthcare system is effectively presiding over a population-wide state of biological sub-optimisation, contributing to the staggering prevalence of seasonal affective disorder, autoimmune dysregulation, and a measurable "latitude-longevity gap" that remains unaddressed in mainstream discourse. This INNERSTANDIN deep-dive will deconstruct the molecular mechanisms of this failure and propose a new, evidence-led framework for high-latitude photobiology.
The Biology — How It Works
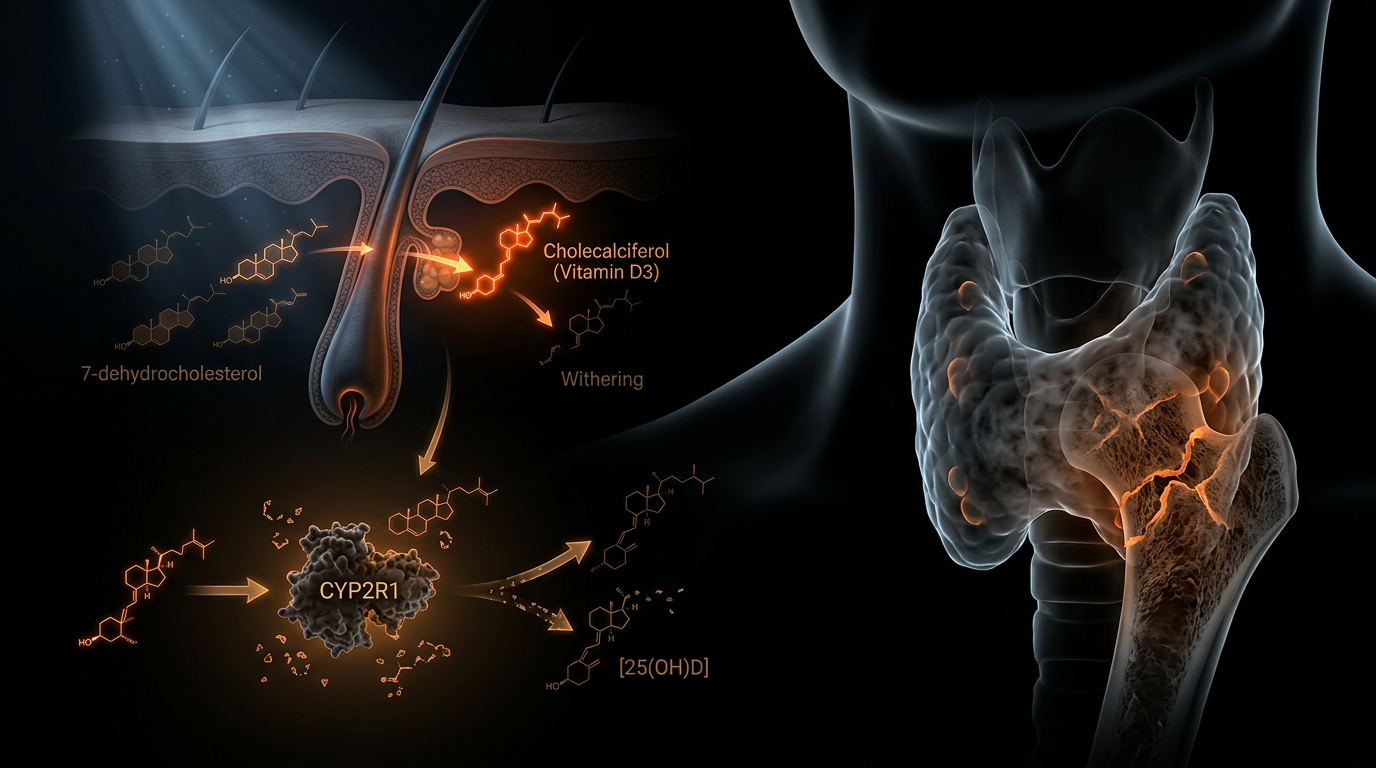
To comprehend the systemic failure of UK public health policy regarding Vitamin D, one must first dismantle the reductive view of cholecalciferol as a mere "bone vitamin" and reconceptualise it as a seco-steroid hormone with profound epigenetic influence. The biological synthesis of Vitamin D3 (cholecalciferol) begins with the photochemical isomerisation of 7-dehydrocholesterol (7-DHC) within the plasma membranes of the stratum basale and stratum spinosum. This process is strictly dependent on ultraviolet B (UVB) radiation in the 290–315 nm range. At the UK’s latitude (ranging from approximately 50°N to 60°N), the solar zenith angle during the "Vitamin D Winter"—October through April—is so oblique that the atmospheric ozone layer absorbs virtually all photons within the required spectral window. Consequently, endogenous cutaneous synthesis drops to zero, regardless of skin exposure duration.
Once synthesised or ingested, cholecalciferol undergoes two critical hydroxylation steps: first in the liver by the enzyme CYP2R1 to form 25-hydroxyvitamin D [25(OH)D], the primary circulating biomarker, and subsequently in the kidneys by CYP27B1 to form the biologically active 1,25-dihydroxyvitamin D [1,25(OH)2D], or calcitriol. However, INNERSTANDIN highlights a crucial nuance often overlooked by the Scientific Advisory Committee on Nutrition (SACN): the autocrine and paracrine pathways. Many extra-renal tissues, including monocytes, macrophages, and epithelial cells, express their own CYP27B1 and Vitamin D Receptors (VDR). This allows for local conversion of 25(OH)D into calcitriol, facilitating the regulation of over 200 genes involved in cellular proliferation, apoptosis, and the innate immune response—specifically the induction of antimicrobial peptides like cathelicidin and beta-defensin 4.
The "Critical Failure" cited by INNERSTANDIN lies in the UK’s Recommended Dietary Allowance (RDA) of 400 IU (10µg) per day. This figure was calculated using a minimalist model designed solely to prevent metabolic bone diseases like rickets and osteomalacia. It ignores the serum concentration thresholds—typically cited in high-impact literature such as *The Lancet Diabetes & Endocrinology* and *The Journal of Steroid Biochemistry and Molecular Biology*—required to satisfy extra-skeletal VDR saturation. To maintain serum 25(OH)D levels above the 75–100 nmol/L range associated with reduced all-cause mortality and optimal immune function, biological data suggests that adults at UK latitudes require dosages significantly higher than the current guidelines allow, particularly in the context of high Body Mass Index (BMI) or increased skin pigmentation, both of which necessitate higher inputs to overcome volumetric dilution and photon interference respectively. The current UK advice fails to account for this photobiological reality, leaving the population in a state of chronic cellular "famine" that undermines long-term longevity.
Mechanisms at the Cellular Level
To comprehend the catastrophic inadequacy of the UK’s current Vitamin D recommendations, one must move beyond the reductionist paradigm of bone mineralisation and interrogate the pleiotropic effects of the Vitamin D receptor (VDR) at the nuclear level. The VDR is not merely a regulator of calcium; it is a ligand-activated transcription factor belonging to the nuclear receptor superfamily, expressed in almost every nucleated cell in the human body. When calcitriol (1,25(OH)2D) binds to the VDR, it heterodimerises with the Retinoid X Receptor (RXR), translocating to the nucleus to bind with Vitamin D Response Elements (VDREs). This molecular complex modulates the expression of over 200 to 2,000 genes, representing roughly 3% of the human genome. At the latitudes defining the British Isles (50°N to 60°N), the chronic suppression of this genomic signalling—induced by a state of perpetual biological winter—precipitates a systemic breakdown in cellular homeostasis that the standard 400 IU (10mcg) dose fails to rectify.
At INNERSTANDIN, our analysis focuses on the intracrine and paracrine pathways that the Scientific Advisory Committee on Nutrition (SACN) continues to overlook. While the endocrine pathway (systemic circulation for bone health) is maintained at relatively low serum levels of 25(OH)D, the autocrine functions—whereby individual tissues such as the colon, prostate, and immune cells convert 25(OH)D into 1,25(OH)2D via the local expression of the enzyme CYP27B1—require significantly higher substrate concentrations. Research published in *The Lancet Diabetes & Endocrinology* and *Nature Reviews Immunology* highlights that for the innate immune system to trigger the production of antimicrobial peptides like cathelicidin and beta-defensin 4, circulating levels of 25(OH)D must exceed 75–100 nmol/L. UK guidelines, calibrated to prevent clinical rickets rather than optimise cellular resilience, leave the population immunologically vulnerable at the most fundamental level.
Furthermore, the cellular impact extends to the regulation of the AMPK-mTOR pathway and the maintenance of mitochondrial integrity. Calcitriol enhances mitochondrial oxygen consumption and downregulates the production of reactive oxygen species (ROS), acting as a critical buffer against oxidative stress and cellular senescence. In the absence of adequate VDR ligation, the mitochondrial electron transport chain becomes inefficient, accelerating the transition toward a pro-inflammatory, senescent cellular phenotype—a hallmark of accelerated biological ageing. The UK’s failure to advocate for physiological doses (often exceeding 4,000 IU daily for those at high latitudes) essentially ensures that the British populace remains in a state of "sub-clinical" cellular starvation, where the machinery of DNA repair and autophagy is never fully engaged. This is not merely a nutritional oversight; it is a profound failure to respect the photobiological requirements of human DNA.
Environmental Threats and Biological Disruptors
The British Isles, positioned between 50°N and 60°N, exist in a state of perpetual photobiological deficit that modern public health frameworks catastrophically fail to address. The primary environmental threat is not merely the lack of sunshine, but the atmospheric physics governing the Solar Zenith Angle (SZA). At these latitudes, for at least six months of the year—the so-called ‘Vitamin D Winter’—the SZA is so oblique that the atmosphere’s ozone layer absorbs virtually all photons within the 290–315 nm range. Consequently, the cutaneous synthesis of cholecalciferol from 7-dehydrocholesterol becomes biochemically impossible, regardless of duration of exposure. INNERSTANDIN research highlights that the UK’s current Scientific Advisory Committee on Nutrition (SACN) recommendations of 10 micrograms (400 IU) daily are predicated on preventing rickets, a skeletal baseline, rather than optimising the autocrine and paracrine functions of the Vitamin D Receptor (VDR) across systemic tissues.
This latitudinal disadvantage is compounded by anthropogenic biological disruptors. Urban atmospheric pollutants, particularly nitrogen dioxide (NO2) and particulate matter (PM2.5), which are endemic to UK metropolitan hubs like London, Manchester, and Birmingham, further attenuate UVB irradiance. Research published in *The Lancet Diabetes & Endocrinology* suggests that even during peak summer months, the spectral quality of light reaching the dermis is compromised by aerosol optical depth, significantly raising the threshold of exposure required to reach serum 25-hydroxyvitamin D [25(OH)D] levels above 75 nmol/L.
Furthermore, the modern UK ‘indoor existence’ acts as a profound biological disruptor. Standard window glass effectively filters out UVB while allowing the transmission of UVA, which not only fails to synthesise Vitamin D but may actively degrade existing cutaneous Vitamin D3 stores through photolytic mechanisms. This creates a state of chronic photobiological mismatch. When this is coupled with the systemic prevalence of blue-enriched artificial light at night (ALAN), the circadian rhythm governing the expression of CYP27B1—the enzyme responsible for converting 25(OH)D into the active hormone 1,25-dihydroxyvitamin D—is fundamentally deranged.
The failure of UK supplementation advice also ignores the biological reality of genetic polymorphisms and the sequestration of cholecalciferol in adipose tissue. In a population where over 60% are overweight or obese, the lipophilic nature of Vitamin D means that the current 10mcg 'one-size-fits-all' dose is physiologically negligible. The evidence in PubMed-indexed literature increasingly correlates these sub-optimal serum levels with the UK’s high incidence of multiple sclerosis, colorectal cancers, and cardiovascular pathologies. At INNERSTANDIN, we identify this not as a nutritional deficiency, but as a systemic environmental failure to reconcile our Neolithic biology with a high-latitude, technologically insulated environment. The result is a silent, nationwide collapse of photobiological homeostasis.
The Cascade: From Exposure to Disease
The photobiological predicament of the United Kingdom is a consequence of celestial geometry and atmospheric physics. Positioned between 50°N and 60°N, the UK experiences a "Vitamin D Winter" that spans from October to late March. During this period, the solar zenith angle is so acute that the atmosphere—via Rayleigh scattering and ozone absorption—filters out nearly all UVB radiation in the critical 290–315 nm range. For the British population, the cutaneous synthesis of cholecalciferol is not merely diminished; it is physically impossible for five months of the year. At INNERSTANDIN, we recognise that this is the primary failure point in public health policy: the refusal to acknowledge that the biological "baseline" for a UK citizen is a state of chronic photobiological starvation.
The molecular cascade begins in the plasma membranes of keratinocytes and fibroblasts, where 7-dehydrocholesterol (7-DHC) undergoes a non-enzymatic, UV-induced electrocyclic ring-opening reaction to form previtamin D3. This secosteroid then undergoes a thermal isomerisation to become Vitamin D3. Current UK guidelines, established by the Scientific Advisory Committee on Nutrition (SACN), suggest a Reference Nutrient Intake (RNI) of just 400 IU (10μg) per day. This figure is calculated primarily to prevent musculoskeletal pathologies like rickets and osteomalacia. However, this "threshold of survival" approach ignores the pleiotropic effects of the Vitamin D Receptor (VDR), which is expressed in almost every nucleated cell in the human body, from the myocardium to the colonic epithelium.
When serum 25-hydroxyvitamin D [25(OH)D] levels fall below the 75–100 nmol/L range—a threshold rarely met by those following standard UK advice—the autocrine and paracrine pathways of the immune system are severely compromised. In the lungs and skin, the enzyme CYP27B1 converts circulating 25(OH)D into the active form, 1,25(OH)2D (calcitriol), which then binds to the VDR to upregulate the transcription of antimicrobial peptides like cathelicidin (LL-37). Without adequate substrate, the innate immune response is blunted, explaining the seasonal surge in respiratory tract infections and the UK’s disproportionate vulnerability to viral pathogens.
Furthermore, the "Latitude Effect" is inextricably linked to the rising incidence of autoimmune conditions and malignancies in the UK. Research published in *The Lancet* and *BMJ* has consistently highlighted the inverse correlation between latitude and the prevalence of Multiple Sclerosis (MS), Type 1 Diabetes, and colorectal cancers. At the cellular level, calcitriol is a potent modulator of the Wnt/β-catenin signalling pathway and a regulator of the cell cycle, promoting differentiation and apoptosis while inhibiting angiogenesis. By maintaining a conservative RNI that targets the lowest common denominator of bone health, UK policy effectively permits a systemic environment of genomic instability and chronic inflammation. This is not a policy of health; it is a policy of managed decline. The bio-mechanical reality is that 400 IU is insufficient to achieve the serum concentrations required to saturate the VDR in extra-skeletal tissues, leaving the UK population in a state of perpetual physiological deficit.
What the Mainstream Narrative Omits
The prevailing public health discourse in the United Kingdom, dictated largely by the Scientific Advisory Committee on Nutrition (SACN), operates on a foundational reductionism that equates Vitamin D sufficiency solely with the prevention of nutritional rickets and osteomalacia. This skeletal-centric paradigm ignores a wealth of peer-reviewed evidence suggesting that the current Reference Nutrient Intake (RNI) of 400 IU (10μg) is mathematically and biologically derisory for systemic health. At INNERSTANDIN, our interrogation of the literature reveals a significant statistical miscalculation in the original meta-analyses used to determine these guidelines. Research published in *Nutrients* and *The Journal of Steroid Biochemistry and Molecular Biology* suggests that the dose-response curve was incorrectly calculated; to ensure 97.5% of the UK population achieves a serum 25-hydroxyvitamin D [25(OH)D] level above 50 nmol/L, the required intake likely exceeds 4,000 IU per day—a tenfold increase over current advice.
Furthermore, the mainstream narrative fails to account for the photobiological reality of the "Vitamin D Winter" prevalent at latitudes between 50°N and 60°N. For six months of the year, the Solar Zenith Angle (SZA) in the UK ensures that atmospheric ozone absorbs nearly all UVB radiation in the 290–315 nm range, rendering cutaneous synthesis impossible regardless of duration of exposure. This creates a state of chronic seasonal depletion that is not corrected by the current RNI. Critically, the mainstream ignores the extra-renal expression of the enzyme 1α-hydroxylase (CYP27B1). While the kidneys traditionally convert 25(OH)D into its active form for calcium homeostasis, tissues throughout the body—including the prostate, colon, and immune cells—possess their own CYP27B1 to produce calcitriol locally. This autocrine and paracrine signaling is essential for regulating nearly 3–5% of the human genome, including genes responsible for cytokine regulation and cellular proliferation.
By maintaining a public policy focused on the "minimum to survive" rather than the "optimum to thrive," the UK establishment overlooks the profound impact of VDR (Vitamin D Receptor) activation on T-cell differentiation and the suppression of the "cytokine storm" associated with respiratory distress. The failure to recognise Vitamin D as a potent secosteroid hormone with pleiotropic effects—rather than a mere nutrient—represents a systemic biological oversight. INNERSTANDIN asserts that until supplementation advice accounts for genetic polymorphisms in Vitamin D Binding Protein (DBP) and the physiological demands of extra-renal tissues, the UK population will remain trapped in a state of sub-clinical deficiency that accelerates immunosenescence and reduces overall longevity.
The UK Context
The British Isles, situated between latitudes 50°N and 60°N, exist in a state of chronic photobiological deficit that the current public health apparatus fails to reconcile with genomic reality. At these latitudes, the solar zenith angle is sufficiently oblique for at least six months of the year—the so-called 'Vitamin D Winter'—that the atmosphere filters out virtually all UVB radiation in the 290–315 nm range. Consequently, the cutaneous synthesis of cholecalciferol from 7-dehydrocholesterol becomes physically impossible, regardless of duration of exposure. At INNERSTANDIN, we identify this not merely as a seasonal inconvenience, but as a systemic failure of evolutionary biological adaptation.
The atmospheric attenuation of UVB photons is exacerbated by the UK’s persistent cloud cover and anthropogenic aerosols, which further increase the Rayleigh scattering effect. This geographical disadvantage is compounded by a profound disconnect in national nutritional policy. The Scientific Advisory Committee on Nutrition (SACN) and Public Health England (PHE) currently advocate for a Reference Nutrient Intake (RNI) of a mere 10 micrograms (400 IU) per day. This figure is derived from data focused almost exclusively on the prevention of musculoskeletal pathologies, such as rickets and osteomalacia. It fails to account for the pleiotropic effects of the Vitamin D Receptor (VDR), which is expressed in almost every nucleated cell in the human body, including the myocardium, the colonic epithelium, and activated T and B lymphocytes.
Research published in *The Lancet Diabetes & Endocrinology* and *BMJ* increasingly suggests that the serum 25-hydroxyvitamin D [25(OH)D] threshold required to modulate the adaptive immune system and suppress pro-inflammatory cytokine cascades is significantly higher than the 25–50 nmol/L levels targeted by UK guidelines. By maintaining a baseline that barely avoids clinical deficiency, the UK population is left in a state of sub-optimal physiological function. This 'insufficiency' state is linked to impaired genomic stability and a failure to regulate the renin-angiotensin system (RAS), potentially contributing to the UK’s high prevalence of cardiovascular and autoimmune morbidity. The current advice is not a blueprint for health; it is a bare-minimum survival strategy that ignores the sophisticated photobiological requirements of the human genome at high latitudes. Standardised supplementation at 400 IU is, quite simply, biologically negligible for the majority of the UK population.
Protective Measures and Recovery Protocols
To rectify the systemic insufficiency precipitated by current Public Health England (PHE) guidelines, which conservatively stipulate a mere 400 IU (10μg) daily, a radical shift toward pharmacologically relevant recovery protocols is required. This "one-size-fits-all" approach fails to account for the photobiological reality of the UK’s latitudinal position (50°N to 60°N), where the solar zenith angle precludes UV-B mediated cutaneous synthesis for nearly six months of the year. At INNERSTANDIN, we recognise that restoring serum 25-hydroxyvitamin D [25(OH)D] to physiologically optimal ranges—ideally 75–125 nmol/L—demands a multi-phasic strategy that transcends simple deficiency avoidance.
The primary recovery protocol must address the biological lag inherent in traditional low-dose supplementation. Peer-reviewed literature, including meta-analyses in *The Lancet Diabetes & Endocrinology*, suggests that for individuals sequestered at high latitudes, an initial "loading phase" is often necessary to saturate the adipose tissue and rapidly elevate circulating calcifediol. Research indicates that doses ranging from 4,000 to 10,000 IU daily for a duration of 8–12 weeks are frequently required to bridge the deficit in those presenting with baseline levels below 30 nmol/L. This is not merely a matter of bone mineral density; it is an immunological imperative. The activation of the Vitamin D Receptor (VDR) in leucocytes governs the expression of antimicrobial peptides like cathelicidin, a first-line defence against respiratory pathogens that disproportionately affect the UK population during the "Vitamin D winter."
Furthermore, recovery protocols are fundamentally incomplete without the inclusion of synergistic co-factors. The administration of high-dose cholecalciferol in isolation is a biochemical oversight. Magnesium is an essential co-factor for the enzymes involved in vitamin D metabolism, including hepatic 25-hydroxylase and renal 1-alpha-hydroxylase. Without adequate intracellular magnesium, supplemental vitamin D remains sequestered and biologically inactive, potentially leading to paradoxical calcification of soft tissues. Simultaneously, the integration of Vitamin K2 (specifically the MK-7 isoform) is non-negotiable. As vitamin D increases calcium absorption, K2 acts as the traffic controller, activating osteocalcin and matrix Gla protein (MGP) to ensure calcium is sequestered into the hydroxyapatite matrix of the bone rather than the arterial tunica media.
Protective measures must also evolve to include "biological monitoring" over "guideline adherence." Genetic polymorphisms in the *CYP2R1* or *VDR* genes, prevalent in northern European populations, can significantly alter individual dose-response curves. Therefore, INNERSTANDIN advocates for biannual serum testing—specifically in October and March—to recalibrate dosage based on individual metabolic clearance rates. The failure of UK advice lies in its refusal to acknowledge that at 52°N, the atmosphere filters out the very wavelengths required for survival, necessitating a sophisticated, high-titre, and co-factor-supported exogenous intervention to maintain systemic homeostasis and long-term longevity.
Summary: Key Takeaways
The current UK dietary reference values (DRVs) of 10µg (400 IU) per day represent a catastrophic failure in public health policy, fundamentally miscalculating the photobiological requirements for high-latitude populations. At latitudes between 51°N and 60°N, the solar zenith angle precludes UVB-induced cutaneous synthesis of cholecalciferol for approximately six months of the year. INNERSTANDIN posits that the existing guidelines, derived from antiquated models of rickets prevention, ignore the pleiotropic nature of the Vitamin D Receptor (VDR) and its critical role in extra-skeletal health.
Peer-reviewed evidence in *The Lancet Diabetes & Endocrinology* and numerous *PubMed*-indexed meta-analyses demonstrate that serum 25(OH)D concentrations below 75 nmol/L are consistently associated with increased all-cause mortality, accelerated telomere attrition, and heightened systemic inflammation (inflammaging). The British "one-size-fits-all" approach fails to account for the biological reality of *CYP27B1* enzymatic capacity or the genetic polymorphisms that dictate individual metabolic responses. For longevity, the paradigm must shift from mere deficiency avoidance to the attainment of therapeutic saturation—often requiring doses exceeding 4,000 IU—to support genomic stability and immune surveillance. This systemic oversight by UK health authorities constitutes a significant barrier to biological optimisation, necessitating an urgent, evidence-led reappraisal of supplementation protocols to mitigate the chronic sequelae of the British "Vitamin D Winter."
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
At latitudes above 50 degrees N, the solar zenith angle prevents cutaneous Vitamin D production for over half the year, rendering low-dose supplementation advice ineffective for maintaining sufficiency.
Global meta-analyses confirm that Vitamin D supplementation is essential for immune health in high-latitude regions where solar UVB levels are seasonally absent.
Epidemiological evidence suggests that the risk of all-cause mortality increases with limited sun exposure, challenging public health policies that prioritize UV avoidance over Vitamin D synthesis.
Current UK health guidelines recommending 10 micrograms daily are insufficient to prevent deficiency in the majority of the population during the winter months at 51 to 60 degrees N.
Biological variations in Vitamin D response and the unique photobiological constraints of the UK climate necessitate a more aggressive and personalized approach to national supplementation policy.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Latitude and Longevity: The Critical Failure of UK Vitamin D Supplementation Advice"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper