Ketogenic Modulation of the NLRP3 Inflammasome: A New Frontier in Lipoedema Management
This research analysis examines the biochemical intersection of nutritional ketosis and the NLRP3 inflammasome, offering a revolutionary perspective on lipoedema management. By transitioning the body's primary fuel source to beta-hydroxybutyrate, we can actively downregulate the systemic inflammation and mitochondrial dysfunction that drive pathological adipose expansion. This metabolic shift represents a potent, non-surgical intervention for reducing limb volume and restoring lymphatic health in a population long ignored by traditional medicine.
Overview
Lipoedema is a condition that has been systemically misunderstood, misdiagnosed, and marginalised within the British medical establishment for decades. First described in 1940 by Allen and Hines at the Mayo Clinic, it remains a phantom in many modern GP surgeries across the United Kingdom, often dismissed as simple obesity or lifestyle-induced weight gain. However, the biological reality is far more complex and insidious. Lipoedema is a chronic, progressive adipose tissue disorder characterised by the symmetrical accumulation of abnormal subcutaneous fat, primarily in the lower limbs, which is remarkably resistant to traditional caloric restriction and exercise. This is not merely a cosmetic concern; it is a state of chronic metabolic distress, lymphatic congestion, and systemic inflammation that affects roughly one in eleven women globally, yet remains largely absent from medical school curricula. The hallmark of the disease is the disproportionate expansion of the limbs, sparing the feet and hands, often resulting in significant pain, bruising, and mobility issues. As the disease progresses, it transitions from a purely adipose-centric issue to a secondary lymphoedema (lipolymphoedema), where the lymphatic vessels become physically crushed by the expanding fat cells and the associated interstitial fibrosis.
At the heart of this pathology lies the NLRP3 inflammasome—a multi-protein complex that acts as the master regulator of the body's innate inflammatory response. In the context of lipoedema, this inflammasome is in a state of perpetual hyper-activation, driving the expansion of fibrotic adipose tissue and the eventual collapse of the lymphatic system. Emerging evidence suggests that nutritional ketosis, once viewed merely as a niche weight-loss tool, provides a sophisticated metabolic intervention capable of silencing this inflammatory cascade at its source. By shifting the primary fuel source from glucose to the ketone body beta-hydroxybutyrate (BHB), we can fundamentally reprogramme the cellular environment. This metabolic shift does not just provide a 'cleaner' fuel; it serves as a powerful signalling mechanism that directly inhibits the assembly of the NLRP3 complex. This article will dissect the intricate relationship between ketogenic signalling and the NLRP3 inflammasome, exposing how the modern environmental and dietary landscape has created a perfect storm for lipoedema progression.
Despite affecting millions of women, the average time to diagnosis for lipoedema in the UK is currently estimated at over 15 years, during which time many patients are subjected to harmful 'eat less, move more' advice that exacerbates their metabolic dysfunction.
The Biology — How It Works
To understand why a ketogenic diet is uniquely suited for lipoedema, one must first understand the metabolic flexibility (or lack thereof) in the lipoedemic adipose tissue. Normal adipose tissue is a dynamic endocrine organ; lipoedemic adipose tissue, however, behaves like a metabolic 'sink.' It is characterised by adipocyte hypertrophy (cells getting larger) and hyperplasia (more cells being created), accompanied by a profound degree of interstitial oedema. This tissue is essentially trapped in a state of chronic hypoxia. As the fat cells expand beyond the reach of their local capillary supply, they become oxygen-deprived. This hypoxia triggers a massive inflammatory response, as the cells desperately signal for more blood supply while simultaneously releasing pro-inflammatory cytokines like IL-6 and TNF-alpha. In a standard high-carbohydrate metabolic state, high levels of circulating insulin further prevent the breakdown of these fats (lipolysis), effectively locking the energy inside the cells and exacerbating the swelling.
Enter nutritional ketosis. When carbohydrate intake is restricted to below 20-30 grams per day, the liver begins to convert fatty acids into ketone bodies: acetoacetate, beta-hydroxybutyrate (BHB), and acetone. This is not a state of starvation, but a highly evolved survival mechanism that prioritises mitochondrial efficiency. BHB, the primary ketone body of interest, is more than just a metabolite; it is an HDAC (histone deacetylase) inhibitor and a ligand for various G-protein coupled receptors. In the mitochondria, BHB is a more efficient fuel than glucose, producing fewer Reactive Oxygen Species (ROS) per unit of ATP generated. In lipoedema, where mitochondria are often already stressed and 'leaky,' this reduction in ROS is critical. By lowering oxidative stress, BHB helps to stabilise the mitochondrial membrane, preventing the release of mitochondrial DNA into the cytosol—a key trigger for the NLRP3 inflammasome.
Furthermore, the reduction in circulating insulin levels that accompanies a ketogenic diet is paramount. Insulin is a primary driver of sodium retention in the kidneys. By lowering insulin, the body naturally sheds excess sodium and the water that follows it (the 'natriuretic' effect of ketosis). For a lipoedema patient, whose limbs are chronically swollen with protein-rich interstitial fluid, this reduction in fluid retention can result in an immediate decrease in limb volume and a reduction in the physical pressure exerted on the lymphatic vessels. This is the first step in restoring the 'Starling forces' that govern fluid exchange at the capillary level, allowing the lymphatic system to finally begin clearing the backlog of waste products that have accumulated in the tissue.
Mechanisms at the Cellular Level
The most profound impact of ketosis on lipoedema occurs at the level of the NLRP3 inflammasome (Nucleotide-binding domain, Leucine-rich-containing family, Pyrin domain-containing-3). This complex is a part of the innate immune system that, when activated, triggers the maturation of highly inflammatory cytokines: Interleukin-1̢ (IL-1̢) and Interleukin-18 (IL-18). Research, most notably by Youm et al. (Nature Medicine, 2015), has demonstrated that BHB specifically suppresses the activation of the NLRP3 inflammasome in response to various stimuli, including urate crystals, ATP, and lipopolysaccharides (LPS). BHB achieves this by preventing the efflux of potassium ions (K+) from the cell and by blocking the oligomerisation of the NLRP3 protein with its adapter protein, ASC (Apoptosis-associated speck-like protein containing a CARD).
In lipoedema patients, the NLRP3 inflammasome is often triggered by 'danger-associated molecular patterns' (DAMPs). These DAMPs include fragments of the extracellular matrix that have been broken down by chronic inflammation, as well as saturated fatty acids and uric acid. When NLRP3 is activated, it recruits Caspase-1, which then cleaves pro-IL-1̢ into its active form. IL-1̢ is a potent driver of fibrosis. It stimulates fibroblasts to produce excess collagen, which stiffens the adipose tissue, creating the 'pearl-like' nodules and 'bean' structures characteristic of Stage 2 and Stage 3 lipoedema. This fibrosis is what makes lipoedema fat so difficult to lose; it is physically walled off by a mesh of connective tissue. By inhibiting the NLRP3 inflammasome, BHB directly slows or stops this fibrotic progression.
The Role of GPR109A and NAD+
BHB also acts through the GPR109A receptor, which is highly expressed in adipose tissue and immune cells. Activation of this receptor has been shown to have potent anti-inflammatory effects and can actually promote the browning of white adipose tissue. 'Brown fat' is more metabolically active and contains more mitochondria, which helps to dissipate energy as heat rather than storing it as stagnant mass. Additionally, the ketogenic state increases the NAD+/NADH ratio. NAD+ is a critical co-factor for sirtuins (specifically SIRT1 and SIRT3), which are longevity enzymes that repair DNA and regulate mitochondrial health. In the context of lipoedema, high NAD+ levels help to 'clean up' the damaged cellular environment, promoting autophagy—the process by which the cell recycles damaged components. This cellular housecleaning is essential for reversing the metabolic stagnation that defines the lipoedemic limb.
Environmental Threats and Biological Disruptors
While the internal metabolic environment is critical, we cannot ignore the external factors that exacerbate lipoedema and trigger the NLRP3 inflammasome. We are living in an era of unprecedented exposure to environmental toxins that act as 'obesogens' and endocrine disruptors. For a lipoedema patient, whose condition is hormonally sensitive (specifically to oestrogen), these disruptors are catastrophic. Xenoestrogens found in plastics (BPA, phthalates), pesticides (glyphosate), and industrial chemicals (PFAS) mimic natural oestrogen and bind to oestrogen receptors in the adipose tissue. This over-stimulation of oestrogen pathways promotes the proliferation of fat cells and increases the permeability of the blood vessels, leading to more fluid leakage into the tissues.
The UK's Environment Agency has frequently reported on the presence of 'forever chemicals' (PFAS) in British waterways, which have been linked to metabolic dysfunction and the dysregulation of lipid metabolism in humans.
These chemicals do not just affect hormones; they act as direct triggers for the NLRP3 inflammasome. Microplastics, which have now been found in human blood and adipose tissue, are perceived by the immune system as foreign invaders. The macrophages within the lipoedemic fat attempt to engulf these particles, which causes lysosomal rupture and subsequent NLRP3 activation. This creates a vicious cycle where the environment is constantly 'priming' the inflammatory response, making the fat more fibrotic and more resistant to treatment. Furthermore, the modern British diet, heavily reliant on ultra-processed foods, provides a constant stream of refined seed oils (high in Omega-6) and high-fructose corn syrup. Omega-6 fatty acids, specifically when consumed in the absence of adequate Omega-3s, provide the raw materials for pro-inflammatory eicosanoids, while fructose is unique in its ability to drive uric acid production and hepatic de novo lipogenesis, both of which are potent NLRP3 activators.
The Cascade: From Exposure to Disease
The progression of lipoedema is not a linear event but a cascading failure of multiple biological systems. It begins with a genetic predisposition, often triggered during periods of significant hormonal shift such as puberty, pregnancy, or menopause. At this stage, the adipocytes in the limbs begin to hypertrophy. This initial expansion causes physical compression of the initial lymphatic capillaries—tiny vessels that are responsible for absorbing interstitial fluid. As these vessels are crushed, fluid begins to pool in the extracellular space. This is not simple water; it is a protein-rich 'sludge' that contains cellular waste, metabolic by-products, and inflammatory signalling molecules.
This stagnant fluid becomes the breeding ground for further inflammation. The presence of excess protein in the interstitium attracts more water (osmotic pressure) and signals the immune system to send in macrophages. However, because the lymphatic drainage is compromised, these immune cells become trapped. They begin to secrete TGF-beta (Transforming Growth Factor beta), which is the master switch for fibrosis. The tissue begins to harden. The 'lumpy' texture of lipoedema fat is the physical manifestation of this internal scarring. As the fibrosis worsens, it further restricts the lymphatics and the microcirculation, leading to local hypoxia. This hypoxia, as previously mentioned, is the primary trigger for the NLRP3 inflammasome. Now, the patient is in a self-perpetuating loop: inflammation causes swelling and fibrosis, which causes more hypoxia, which causes more inflammation.
This cascade eventually affects the system's ability to regulate its own temperature and pain signals. Lipoedemic fat is often cold to the touch because of the poor microcirculation, yet it is hypersensitive to pressure. This 'allodynia' is likely caused by the inflammatory cytokines directly irritating the peripheral nerves and the physical pressure of the fibrotic tissue on nerve endings. Without a metabolic intervention like ketosis to 'break' the inflammatory signal, the patient will inevitably progress through the stages of lipoedema, eventually losing mobility and developing chronic venous insufficiency.
What the Mainstream Narrative Omits
The mainstream medical narrative regarding lipoedema is, at best, woefully outdated and, at worst, dangerously dismissive. For decades, patients have been told that their condition is their fault—a result of gluttony and sloth. This is a scientific impossibility. If lipoedema fat were simply stored energy from excess calories, it would respond to a caloric deficit. It does not. The 'Calories In, Calories Out' (CICO) model of obesity is a primitive oversimplification that fails to account for the hormonal and inflammatory regulation of fat storage. By framing lipoedema as a weight-management issue, the medical establishment ignores the underlying lymphatic and immunological pathology.
Furthermore, the role of nutrition in modulating inflammation is often suppressed or ignored in favour of surgical interventions or life-long reliance on compression garments. While Water-Assisted Liposuction (WAL) can be a life-changing procedure for Stage 3 patients, it is not a cure. If the underlying metabolic environment remains inflammatory and the NLRP3 inflammasome remains hyper-active, the abnormal fat can and will return. The medical establishment also remains largely silent on the role of insulin and the 'High Carb, Low Fat' guidelines that have dominated British nutrition for 40 years. These guidelines, codified in the NHS Eatwell Guide, recommend that carbohydrates make up the majority of food intake. For someone with lipoedema, this is like pouring petrol on a fire. High carbohydrate intake ensures high insulin levels, which prevents the body from accessing its fat stores and keeps the NLRP3 inflammasome in a 'primed' state. The refusal to acknowledge the therapeutic power of nutritional ketosis is a failure of clinical duty, leaving millions of women to manage a progressive disease with nothing but elastic bandages and 'willpower.'
The UK Context
In the United Kingdom, the situation for lipoedema patients is particularly dire. The NHS is currently under immense strain, and specialised services for lipoedema are virtually non-existent in many regions. Most GPs have never received formal training on how to distinguish lipoedema from lymphoedema or obesity. Consequently, many women spend years being shamed by medical professionals before receiving a diagnosis. Even after diagnosis, the treatment options on the NHS are largely limited to 'Conservative Management' — which usually consists of a referral to a lymphoedema clinic for compression stockings and, if the patient is lucky, a few sessions of Manual Lymphatic Drainage (MLD).
While compression is a vital tool for managing the symptoms of lipoedema, it does nothing to address the underlying metabolic cause. Moreover, the 'postcode lottery' for surgical funding means that most women in the UK have no access to the specialised liposuction techniques required to remove fibrotic fat safely. The National Institute for Health and Care Excellence (NICE) has issued some guidelines, but they lack the teeth to ensure that every patient has access to a multi-disciplinary team including metabolic specialists. This institutional inertia is costing the NHS millions in the long term, as lipoedema patients eventually develop comorbidities like osteoarthritis, depression, and Type 2 diabetes due to their decreased mobility and chronic pain. There is an urgent need for the UK to adopt a metabolic-first approach, integrating ketogenic protocols into the standard of care for lipoedema patients to prevent disease progression and reduce the burden on surgical services.
Protective Measures and Recovery Protocols
For those seeking to take control of their biology and silence the NLRP3 inflammasome, a structured metabolic recovery protocol is essential. This is not a 'diet' in the temporary sense, but a fundamental shift in cellular fuel. The primary goal is to achieve and maintain therapeutic ketosis (blood BHB levels between 1.5 and 3.0 mmol/L).
- —Strict Carbohydrate Restriction: Limit total carbohydrate intake to under 20g per day. This is the only way to ensure insulin levels remain low enough to permit lipolysis and activate the anti-inflammatory signalling of BHB. Focus on leafy greens, cruciferous vegetables, and high-quality fats.
- —Elimination of Seed Oils: Completely remove industrially processed seed oils (sunflower, rapeseed, corn, soya) from the diet. These are high in linoleic acid, which can be pro-inflammatory and may exacerbate the oxidative stress within the adipose tissue. Replace them with stable fats like grass-fed butter, tallow, extra virgin olive oil, and coconut oil.
- —Optimised Protein Intake: Aim for moderate protein intake from high-quality, bioavailable sources (ruminant meat, wild-caught fish, eggs). Avoid processed meats containing nitrites and 'fillers' that can trigger an immune response.
- —Electrolyte Management: The 'natriuretic' effect of ketosis means the body will excrete sodium, potassium, and magnesium more rapidly. For lipoedema patients, magnesium is particularly critical. It is a natural calcium channel blocker and is essential for over 300 enzymatic reactions, including those involved in ATP production and muscle relaxation. Supplementing with 400-600mg of Magnesium Glycinate can significantly reduce the leg cramps and 'restless' feelings common in lipoedema.
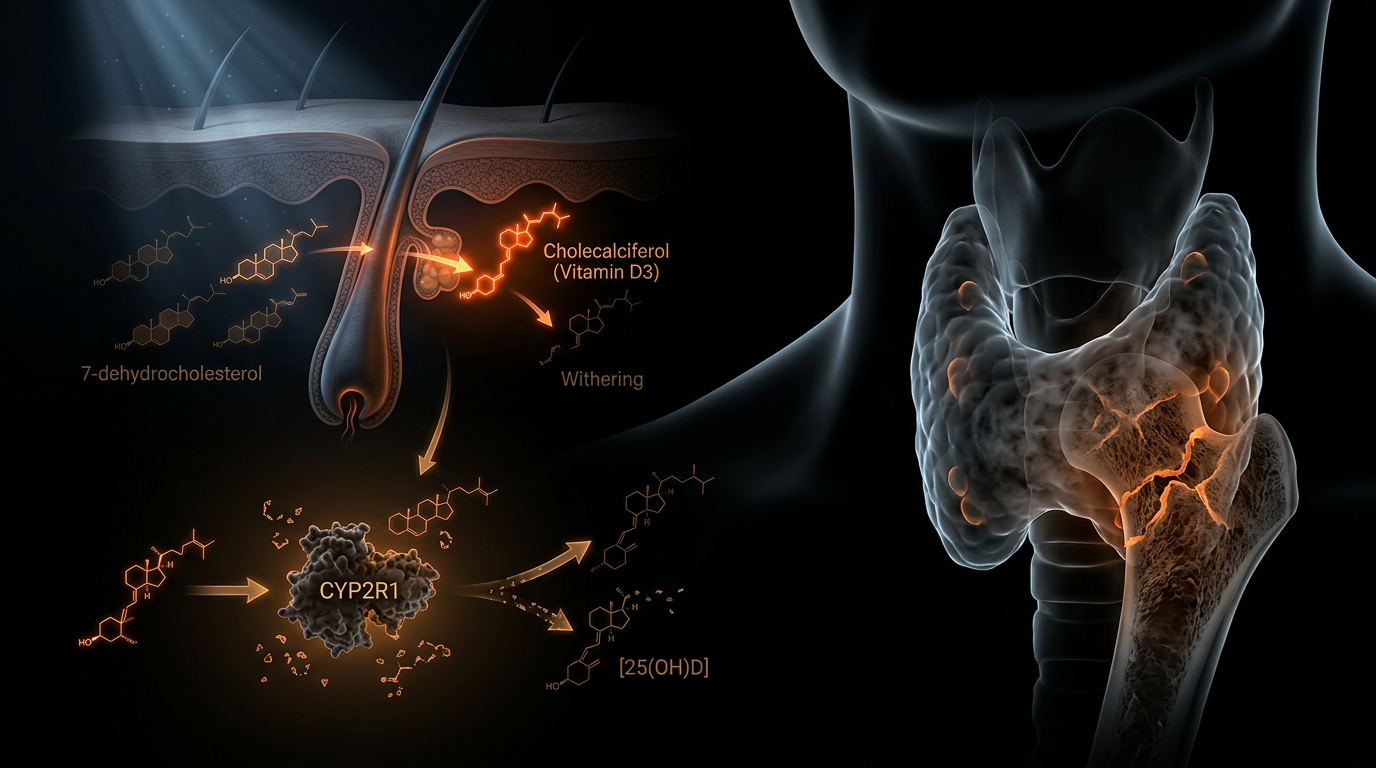
- —Anti-Inflammatory Micronutrients: Consider supplementing with Selenium (to support thyroid function and glutathione production) and Vitamin D3/K2. Many lipoedema patients are chronically low in Vitamin D, which is itself a potent modulator of the immune system and the NLRP3 inflammasome.
- —Mechanical Support: Combine the ketogenic protocol with movement that encourages lymphatic flow without causing high impact. Vibration plates (Whole Body Vibration) are particularly effective, as the G-force helps to manually 'pump' the lymphatic vessels. Dry skin brushing and regular MLD can also help to clear the 'sludge' from the interstitium while the ketogenic diet works on the cellular level.
- —Water Quality: Given the threat of EDCs, use a high-quality water filter (such as a Berkey or a reverse osmosis system) to remove fluoride, chlorine, and PFAS from drinking water. Avoid plastic water bottles and food containers to reduce xenoestrogen exposure.
By following this protocol, patients often report a significant reduction in 'painful fat' within just a few weeks. This is not necessarily due to massive fat loss, but rather the rapid reduction in NLRP3-driven inflammation and interstitial oedema. As the 'fog' of inflammation lifts, the tissue becomes softer, the limbs feel lighter, and the body's natural healing mechanisms can finally begin to address the underlying fibrosis.
Summary: Key Takeaways
Lipoedema is a metabolic and immunological crisis, not a failure of willpower. The NLRP3 inflammasome is the central driver of the inflammation and fibrosis that causes the condition to progress. Nutritional ketosis, through the production of beta-hydroxybutyrate, provides a direct molecular 'off-switch' for this inflammasome. By reducing insulin, lowering oxidative stress, and inhibiting pro-inflammatory cytokines like IL-1̢, a ketogenic protocol offers a profound therapeutic opportunity for lipoedema management. We must move beyond the failed 'Eatwell' guidelines and the obesity-shaming narrative to embrace a biologically-driven approach that addresses the root cause of this debilitating disease. The truth is available to those who look: we have the power to reprogramme our metabolism and reclaim our health from the ground up.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
The ketone metabolite beta-hydroxybutyrate serves as a direct inhibitor of the NLRP3 inflammasome by preventing potassium efflux and reducing the production of pro-inflammatory cytokines IL-1b and IL-18.
Ketogenic diet-induced elevation of beta-hydroxybutyrate suppresses systemic inflammation and improves metabolic health by modulating immune cell activity and inhibiting inflammasome assembly.
Adipose tissue in lipoedema patients exhibits altered metabolic profiles and increased chronic inflammation, suggesting that targeting innate immune pathways like NLRP3 may mitigate disease progression.
Nutritional ketosis shifts the metabolic state of macrophages toward an anti-inflammatory phenotype, effectively dampening the NLRP3-mediated inflammatory cascade in adipose tissues.
Ketone bodies function as signaling molecules that regulate gene expression and cellular stress responses, providing a biochemical basis for reducing oxidative stress-induced inflammasome activation.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Ketogenic Modulation of the NLRP3 Inflammasome: A New Frontier in Lipoedema Management"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper