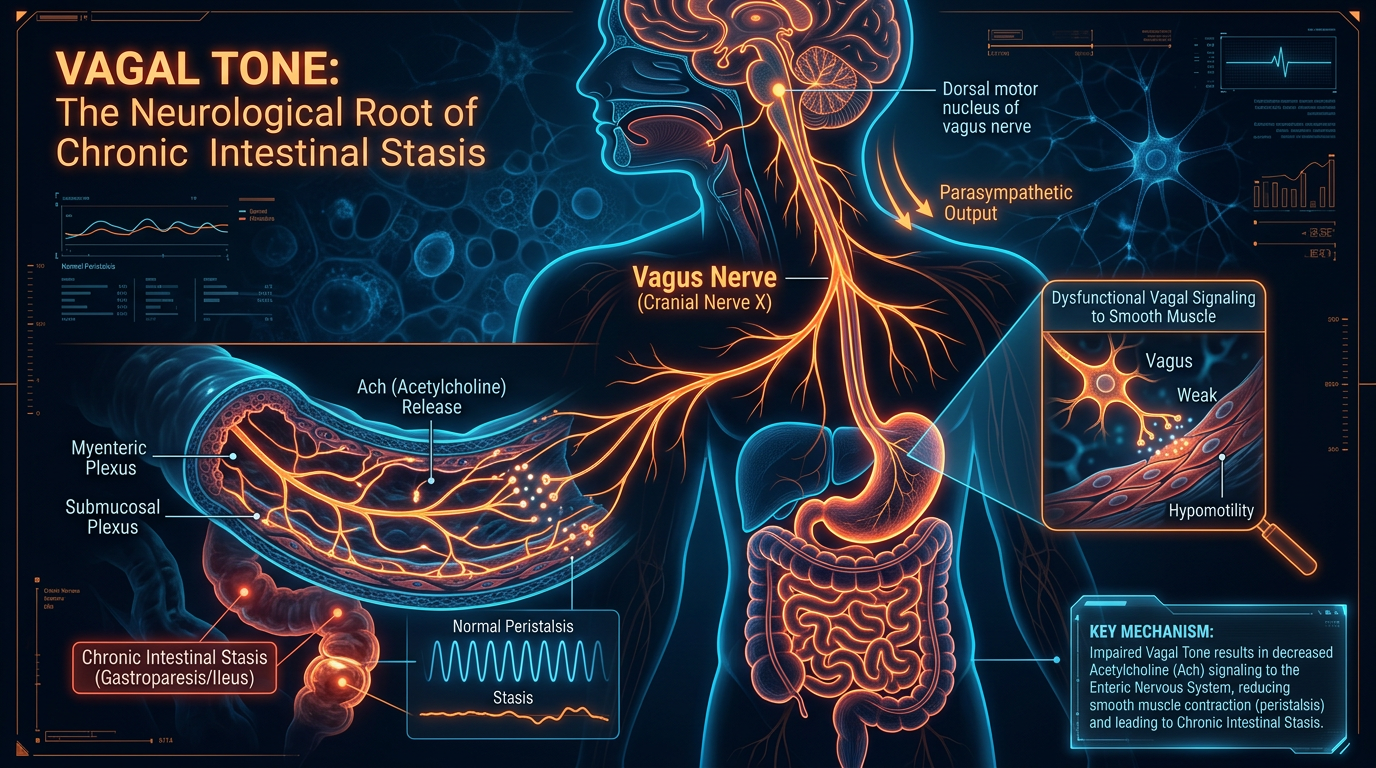
Vagal Tone: The Neurological Root of Chronic Intestinal Stasis
The vagus nerve serves as the superhighway for brain-gut communication, regulating the motor functions required for intestinal transit. Low vagal tone can effectively paralyze the small intestine, creating a stagnant environment for pathogens.
Overview
The modern medical landscape is currently grappling with an epidemic of "functional" gastrointestinal disorders, most notably Small Intestinal Bacterial Overgrowth (SIBO) and Chronic Intestinal Stasis. For decades, the mainstream approach has been reductionist, viewing the gut as a fermentation vat that simply needs the right balance of microbes or a more potent course of antibiotics. This perspective is not only incomplete; it is fundamentally flawed. At INNERSTANDING, we recognize that the physical state of the microbiome is merely a symptom of a deeper, more systemic failure. The true root of chronic intestinal stasis—the paralysis of the small intestine that allows pathogens to flourish—is the degradation of vagal tone.
The vagus nerve (Cranial Nerve X) is the longest and most complex of the cranial nerves, acting as the primary bidirectional superhighway between the brain and the visceral organs. Its name, derived from the Latin for "wandering," reflects its extensive reach from the brainstem down to the colon. In the context of gastroenterology, the vagus nerve is the master conductor of the digestive orchestra. It does not merely "influence" digestion; it dictates the mechanical and chemical environment of the gut. When vagal tone—the measure of the nerve's functional strength and activity—drops, the result is a physiological breakdown known as gastroparesis or, more commonly in the small intestine, chronic stasis.
Low vagal tone effectively mutes the signals required for the Migrating Motor Complex (MMC) to initiate. The MMC is the "housekeeping" wave of the gut, a rhythmic contraction that sweeps undigested food and excess bacteria out of the small intestine and into the colon during periods of fasting. Without the vagal spark to ignite these waves, the small intestine becomes a stagnant pool. In biological terms, stasis is an invitation for colonisation. Pathogenic bacteria, fungi, and archaea—which should be relegated to the large intestine—migrate upwards, consuming nutrients, producing toxic gases (hydrogen, methane, hydrogen sulphide), and eroding the mucosal barrier.
This article serves as a comprehensive interrogation of the vagal-stasis axis. We will move beyond the superficial "gut-health" trends to examine the neurological underpinnings of motility, the cellular mechanisms that fail when the vagus is compromised, and the environmental toxins that are currently waging a silent war on our nervous systems. To understand why SIBO relapses in over 60% of patients treated with antibiotics, one must understand that the problem is not the "bugs"; it is the "wires."
##
The Biology — How It Works
To grasp the magnitude of the vagus nerve's role, one must first understand the architectural divide of the Autonomic Nervous System (ANS). The ANS is split into the Sympathetic Nervous System (SNS)—the "fight or flight" mechanism—and the Parasympathetic Nervous System (PSNS)—the "rest and digest" mechanism. The vagus nerve accounts for approximately 75% of all parasympathetic outflow in the human body. Therefore, digestion is, by definition, a parasympathetic process.
The vagus nerve originates in the medulla oblongata of the brainstem, specifically from the dorsal motor nucleus and the nucleus ambiguus. From here, it descends through the neck, passing near the carotid artery, and branches out to the heart, lungs, and the entirety of the digestive tract. It is a "mixed" nerve, meaning it contains both sensory (afferent) and motor (efferent) fibres. Crucially, 80% of vagal fibres are afferent, sending constant updates from the gut to the brain regarding nutrient status, inflammation, and microbial metabolites. However, the 20% of efferent fibres are what control the "output"—the secretion of hydrochloric acid, the release of bile, and the orchestration of peristalsis.
The Migrating Motor Complex (MMC): The Gut’s Janitor
The primary mechanism by which the vagus nerve prevents SIBO is the regulation of the MMC. Unlike the peristalsis that occurs while eating, the MMC only occurs in the inter-digestive state (fasting). It consists of four distinct phases:
- —Phase I: A period of quiescence with rare contractions.
- —Phase II: Irregular, low-amplitude contractions.
- —Phase III: The "clearing wave." Intense, rhythmic contractions that migrate from the stomach to the terminal ileum.
- —Phase IV: A short transition back to Phase I.
UK FACT: Chronic "bloating" and "IBS" affect approximately 1 in 5 people in the UK. Recent clinical audits suggest that up to 78% of these cases are actually undiagnosed SIBO, driven by a failure of the Phase III clearing wave.
The initiation of Phase III is heavily dependent on the hormone motilin, which is secreted by M-cells in the upper small intestine. However, motilin cannot trigger a successful MMC without concurrent vagal stimulation. The vagus nerve provides the "permissive" neurological tone required for these contractions. When a patient is in a state of sympathetic dominance—chronic stress, anxiety, or physical trauma—the brain prioritises survival over housekeeping. The vagal signal is inhibited, Phase III is skipped, and the "janitor" never arrives to clean the small intestine.
The Gastric Acid Connection
Furthermore, the vagus nerve stimulates the parietal cells in the stomach to produce hydrochloric acid (HCl). Low HCl (hypochlorhydria) is a primary risk factor for stasis. Acid acts as a chemical barrier, killing ingested pathogens and triggering the release of pancreatic enzymes and bile. Vagal dysfunction leads to a "flat" pH in the stomach, which fails to signal the small intestine to move. This creates a feedback loop: the lack of acid prevents the mechanical movement, and the lack of movement prevents the clearing of bacteria, which then further inhibits acid production through the release of lipopolysaccharides (LPS).
##
Mechanisms at the Cellular Level
Moving deeper into the histology of the gut, the vagus nerve does not act alone. It interfaces with the Enteric Nervous System (ENS), often referred to as the "second brain." The ENS consists of two primary plexuses embedded in the wall of the gut: the Myenteric Plexus (Auerbach's), which controls motility, and the Submucosal Plexus (Meissner's), which controls secretions and blood flow.
The Interstitial Cells of Cajal (ICC)
The true mechanical workhorses of the gut are the Interstitial Cells of Cajal (ICC). These are specialised "pacemaker" cells located between the nerve endings and the smooth muscle of the intestine. They generate the slow-wave electrical activity that allows the smooth muscle to contract. The vagus nerve acts as the "power grid" for these ICCs.
In cases of chronic stasis, we often observe a significant loss of ICC density. This is a profound discovery: chronic vagal inhibition leads to the literal death of the gut's pacemaker cells. This is why many patients feel their gut is "paralysed"—at a cellular level, it is. The loss of ICCs is frequently mediated by an autoimmune response, often triggered by a previous bout of food poisoning (post-infectious IBS). When a pathogen like *C. jejuni* enters the system, the body produces antibodies against the toxin (Cytolethal Distending Toxin B). Due to molecular mimicry, these antibodies can attack vinculin, a protein required for the structure of the ICCs and the enteric nerves.
Neurotransmitters: The Language of the Vagus
The primary neurotransmitter of the vagus nerve is Acetylcholine (ACh). ACh binds to nicotinic and muscarinic receptors on the enteric neurons and smooth muscle cells to induce contraction. However, the system also requires "inhibitory" neurotransmitters like Nitric Oxide (NO) and Vasoactive Intestinal Peptide (VIP) to allow the muscle to relax *ahead* of the contraction wave.
ALARMING FACT: Modern exposure to organophosphate pesticides, which are designed to inhibit acetylcholinesterase, directly interferes with the cholinergic signaling of the vagus nerve, effectively inducing a state of chronic neurological constipation across the population.
When vagal tone is low, the production of ACh drops. This leads to a failure of "propulsive motility." Instead of a coordinated wave that moves contents forward, the gut may exhibit "spasmodic" or "non-propulsive" movements, which are felt as cramping and pain but do not actually clear the small intestine. This creates the "stagnant pond" environment where aerobic and anaerobic bacteria can bloom.
##
Environmental Threats and Biological Disruptors
We do not live in a vacuum, and the decline in vagal tone is not merely a "psychological" issue of being too stressed. We are currently navigating a bio-hazardous environment that targets the nervous system with surgical precision.
The Glyphosate Assault
Glyphosate, the primary ingredient in many herbicides used extensively in UK agriculture, is a potent neurotoxin and a mineral chelator. It disrupts the Shikimate pathway in the gut microbiome, but more importantly for vagal tone, it acts as a glycine analogue. Glyphosate can potentially be misincorporated into proteins where glycine belongs, leading to misfolded proteins and neurological degeneration. Furthermore, glyphosate inhibits the synthesis of manganese, a mineral essential for the protection of mitochondria within the vagus nerve. Without functional mitochondria, the vagus nerve cannot maintain the high-frequency electrical firing required for motility.
Neurotropic Viruses and Vagal Infection
The vagus nerve, due to its length and the fact that it is not fully protected by the blood-brain barrier in certain areas (like the *area postrema*), is a prime target for neurotropic viruses. Viruses such as Epstein-Barr (EBV), Herpes Simplex (HSV), and the Varicella-Zoster Virus can "hide" in the vagal ganglia. When these viruses reactivate due to stress or immune suppression, they cause "vagal neuritis"—inflammation of the nerve itself. An inflamed nerve cannot conduct the signals necessary for the MMC. This is a frequently overlooked cause of "sudden onset" SIBO following a viral illness.
Heavy Metal Accumulation
Mercury, lead, and aluminium have a high affinity for nervous tissue. They interfere with the sodium-potassium pumps that allow nerves to fire. Mercury, in particular, can travel via retrograde axonal transport from the gut directly into the brainstem via the vagus nerve. Once there, it can induce chronic neuro-inflammation in the dorsal motor nucleus, permanently lowering the "set point" for vagal outflow and locking the patient into a state of chronic stasis.
The Blue Light and Circadian Mismatch
The vagus nerve is governed by circadian rhythms. The brainstem nuclei receive input from the Suprachiasmatic Nucleus (SCN), the body’s master clock. Modern exposure to artificial blue light late at night suppresses melatonin and signals the brain that it is daytime. This keeps the SNS active and prevents the shift into the deep parasympathetic state required for the overnight "clearing waves" of the MMC. If you are looking at a smartphone at 11 PM, you are effectively telling your vagus nerve to stay "offline," halting the cleaning process that should be occurring while you sleep.
##
The Cascade: From Exposure to Disease
The progression from a healthy, motile gut to chronic intestinal stasis is a predictable cascade. It rarely happens overnight; it is the result of cumulative "allostatic load"—the wear and tear on the body from chronic stress and toxic exposure.
Step 1: Vagal Inhibition
The cascade begins with an insult to the autonomic nervous system. This could be a period of intense emotional trauma, a severe viral infection, or chronic exposure to neurotoxic chemicals. The brainstem perceives a threat and shifts the body into a "sympathetic-dominant" state. In this state, the vagus nerve is downregulated to conserve energy for the "survival" response.
Step 2: The Failure of the Housekeeper
With reduced vagal tone, the MMC becomes infrequent or absent. Food particles from the previous meal remain in the small intestine for 12–15 hours instead of the usual 2–4. This provides a substrate for the few bacteria naturally present in the small intestine to begin fermenting.
Step 3: Fermentation and Gas Production
As bacteria ferment undigested carbohydrates (FODMAPs), they produce hydrogen gas. If methanogens (*Methanobrevibacter smithii*) are present, they consume that hydrogen to produce methane. Methane is a gas-phase paralytic. It further slows down intestinal transit, creating a vicious cycle: stasis breeds bacteria, and bacteria produce gases that cause more stasis.
Step 4: Endotoxaemia and Systemic Inflammation
The overgrowth of bacteria leads to the breakdown of the mucosal lining (Leaky Gut). Gram-negative bacteria release Lipopolysaccharides (LPS) into the bloodstream. The vagus nerve’s afferent fibres detect this LPS and send a "danger" signal to the brain. Paradoxically, chronic high-level LPS exposure can cause the brain to further "shut down" the gut to prevent further absorption of toxins, exacerbating the stasis.
Step 5: The Feedback Loop of Despair
The patient now suffers from systemic symptoms: brain fog (due to neuro-inflammation), fatigue (due to mitochondrial dysfunction), and chronic bloating. Because the vagus nerve is also responsible for the "anti-inflammatory pathway," its failure means the body can no longer switch off the inflammatory response. The patient is now "locked" in a state of chronic disease where the gut is paralysed and the brain is on fire.
##
What the Mainstream Narrative Omits
The mainstream medical approach to SIBO and motility disorders is characterized by a "kill-centric" philosophy. The standard of care in the UK involves the administration of Rifaximin, a non-absorbable antibiotic. While Rifaximin can be effective at temporarily reducing the bacterial load, it does absolutely nothing to address the neurological reason *why* the bacteria were able to overgrow in the first place.
The "Functional" Fallacy
Mainstream gastroenterology often labels patients with "Irritable Bowel Syndrome" (IBS) or "Functional Dyspepsia" when no structural abnormalities (like tumours or ulcers) are found. This label is often a dismissal, implying the condition is psychosomatic. What they omit is that "functional" does not mean "imaginary." It means neurological. A lack of vagal tone is a physical, measurable physiological state (often through Heart Rate Variability, or HRV), but it is rarely measured in a clinical setting.
The Failure of Prokinetics
When doctors do recognize motility issues, they often prescribe prokinetic drugs like Prucalopride (Resolor). While these drugs can stimulate the receptors in the gut, they are essentially "whipping a tired horse." If the underlying vagal tone is not restored, the enteric nervous system becomes desensitized to these drugs, and their efficacy wanes. Mainstream medicine fails to ask: *Why is the signal from the brainstem not reaching the gut?*
The Role of Trauma
Mainstream medicine is remarkably hesitant to discuss the role of developmental trauma and the Polyvagal Theory (developed by Dr Stephen Porges). Early life stress can "calibrate" the autonomic nervous system to stay in a state of permanent "Freeze" or "Flight." This state is biophysically incompatible with high vagal tone. A patient can take all the antibiotics and probiotics in the world, but if their nervous system still perceives the world as an unsafe place, the vagus nerve will remain inhibited, and the gut will remain stagnant.
##
The UK Context
The situation in the United Kingdom presents unique challenges for those suffering from vagal dysfunction and SIBO. The NHS, while a vital institution, is notoriously slow to adopt the latest research in neuro-gastroenterology.
UK STATISTIC: The average time for a patient in the UK to receive a diagnosis of "functional" GI issues from the onset of symptoms is 6.5 years. During this time, the majority are prescribed Proton Pump Inhibitors (PPIs), which further lower stomach acid and worsen the underlying stasis.
The PPI Epidemic
The UK has one of the highest rates of PPI prescriptions (like Omeprazole) in Europe. These drugs are often given for "acid reflux," which in many cases is actually caused by *low* acid and the fermentation of food in the stomach due to low vagal tone. By further suppressing acid, the NHS "standard of care" actively contributes to the development of SIBO and the degradation of the small intestinal environment.
The Nutritional Landscape
The UK diet, increasingly dominated by ultra-processed foods (UPFs), is deficient in the key nutrients required for vagal health. Thiamine (Vitamin B1) is a critical cofactor for the enzyme pyruvate dehydrogenase, which is essential for cellular energy in the nerves. High carbohydrate consumption and the presence of anti-thiamine factors in processed foods have led to a "sub-clinical" thiamine deficiency in the UK. Without B1, the vagus nerve simply cannot fire.
Environmental Fluoridation and Bromination
Large swathes of the UK water supply are fluoridated, and British bread often contains potassium bromate (or is high in bromide). Fluoride and bromide are halides that compete with iodine. Iodine is essential not just for the thyroid, but for the myelination of the nerves. The "demyelination" or slowing of nerve conduction in the vagus can be linked to this environmental halide burden, a topic rarely discussed in British clinical settings.
##
Protective Measures and Recovery Protocols
Recovery from chronic intestinal stasis requires a shift from "killing bacteria" to "rehabilitating the nervous system." We must restore the electrical signal before we can expect the mechanical result.
1. Vagal Nerve Stimulation (VNS)
Direct stimulation of the vagus nerve can "jump-start" the system.
- —Manual Stimulation: Gargling vigorously, singing loudly, or performing the "gag reflex" exercise can stimulate the pharyngeal branches of the vagus.
- —Transcutaneous VNS: Devices that clip onto the tragus of the ear (targeting the Auricular Branch of the Vagus Nerve) have shown remarkable results in clinical trials for increasing HRV and stimulating the MMC.
- —Cold Thermogenesis: Splashing the face with ice-cold water or taking cold showers triggers the "diving reflex," which is mediated by the vagus nerve and results in an immediate parasympathetic shift.
2. Nutritional Neuropathology
We must provide the building blocks for nerve repair and neurotransmitter production.
- —High-Dose Thiamine (TTFD): Using lipid-soluble forms of thiamine like Benfotiamine or Allithiamine can bypass transport issues and re-energize the "paralysed" vagus nerve.
- —Choline and Acetylcholine Support: Supplementing with Alpha-GPC or Phosphatidylcholine provides the raw material for the vagus to produce its primary neurotransmitter, acetylcholine.
- —Magnesium and Potassium: These electrolytes are essential for the resting membrane potential of the nerves. Most UK citizens are chronically deficient in magnesium.
3. Circadian and Postural Alignment
- —The Atlas Adjustment: The vagus nerve exits the skull near the C1 (Atlas) vertebrae. If the Atlas is misaligned (common in "tech neck"), it can physically impinge upon or irritate the vagus nerve. Upper cervical chiropractic care is often a "missing link" for stasis patients.
- —Circadian Hygiene: Ending food intake at least 4 hours before bed and avoiding blue light allows the body to enter the "Deep Sleep" phase where the MMC is most active.
4. Pharmacological Prokinetics (The Strategic Approach)
Instead of using prokinetics as a crutch, use them as a "bridge."
- —Low-Dose Naltrexone (LDN): LDN has been shown to reduce neuro-inflammation in the brainstem and support the MMC by modulating opioid receptors in the gut.
- —Ginger and Artichoke Extracts: These provide a gentle, non-addictive stimulus to the 5-HT4 receptors in the gut, mimicking the signals of the vagus nerve.
5. Somatic Re-patterning
Addressing the "software" of the brain. Techniques like Somatic Experiencing or Breathwork (specifically 4-7-8 breathing or box breathing) help to shift the nervous system out of a chronic "freeze" state. If the brain does not feel safe, it will never allow the gut to "waste" energy on the MMC.
##
Summary: Key Takeaways
The path to resolving SIBO and chronic intestinal stasis is not found at the end of a pill bottle, but in the restoration of our neurological heritage.
- —The Vagus is the Master: Chronic intestinal stasis is primarily a neurological failure, not a bacterial one. The "bugs" are a consequence of the "stasis."
- —The MMC is Non-Negotiable: Without the Phase III clearing wave, SIBO is an inevitability. This wave is entirely dependent on vagal tone.
- —Environment as a Weapon: Glyphosate, heavy metals, and neurotropic viruses are actively degrading our vagal function. We must proactively detoxify and protect our nervous system.
- —Mainstream Failure: The "kill-and-repeat" cycle of antibiotics is a failed paradigm because it ignores the underlying motility mechanics and the health of the Interstitial Cells of Cajal.
- —The UK Context: British patients must look beyond the standard NHS "IBS" protocols, which often exacerbate the condition through the over-prescription of PPIs and a lack of focus on neuro-gastroenterology.
- —Holistic Rehabilitation: Recovery requires a multi-pronged approach: VNS, nutritional support (especially Thiamine), postural correction, and the resolution of stored somatic trauma.
To understand the gut is to understand the nerve. We must stop viewing the human body as a collection of separate parts and start seeing it as an integrated electrical circuit. When the "vagal tone" is restored, the "stagnant pond" becomes a "flowing river," and the body’s innate ability to maintain its own internal terrain is finally reactivated. This is the essence of INNERSTANDING.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Vagal Tone: The Neurological Root of Chronic Intestinal Stasis"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper