
Adiponectin Amplification: Cold Exposure as a Master Regulator of UK Metabolic Syndrome
Overview
The United Kingdom currently navigates a metabolic precipice, with the prevalence of metabolic syndrome—a cluster of conditions including hypertension, hyperglycaemia, and central obesity—reaching critical thresholds across the demographic spectrum. At the epicentre of this physiological crisis lies the dysregulation of adiponectin, a collagen-like protein hormone secreted almost exclusively by adipose tissue. Often termed the ‘guardian angel adipokine,’ adiponectin exerts potent insulin-sensitising, anti-inflammatory, and anti-atherogenic effects through the activation of its primary receptors, AdipoR1 and AdipoR2. However, in the sedentary, thermally-buffered environment characteristic of modern British life, adiponectin expression is chronically suppressed, exacerbating the systemic low-grade inflammation that underpins the NHS-burdening epidemic of Type 2 Diabetes (T2D) and non-alcoholic fatty liver disease (NAFLD).
INNERSTANDIN identifies cold exposure, or thermal hormesis, as the pre-eminent biological catalyst for reversing this adipokine deficiency. The mechanism is rooted in the recruitment and activation of Brown Adipose Tissue (BAT) and the ‘browning’ of white adipocytes via the cold-induced sympathetic-adrenal axis. Upon exposure to acute thermal stress, the release of noradrenaline triggers the β3-adrenergic receptors, initiating a cascade that elevates the expression of Uncoupling Protein 1 (UCP1) and concurrently stimulates the mRNA expression of ADIPOQ, the gene responsible for adiponectin synthesis. Peer-reviewed data indexed in PubMed and the Lancet suggests that this thermogenic response does not merely facilitate calorie burning; it fundamentally reconfigures the secretome of the adipose organ.
This systemic amplification of adiponectin facilitates a shift in metabolic substrate preference. By activating the 5' adenosine monophosphate-activated protein kinase (AMPK) and peroxisome proliferator-activated receptor alpha (PPAR-α) pathways, adiponectin increases glucose uptake in skeletal muscle and enhances fatty acid oxidation in the liver. For the UK population, which suffers from high rates of insulin resistance linked to hypercaloric diets, this cold-mediated endocrine surge offers a non-pharmacological pathway to restore glucose homeostasis. Furthermore, the pleiotropic effects of adiponectin extend to the vascular endothelium, where it stimulates nitric oxide production, directly countering the hypertensive components of metabolic syndrome. INNERSTANDIN posits that the deliberate reintroduction of thermal volatility is not merely a lifestyle choice but a biological necessity for reclaiming metabolic sovereignty in a post-industrial landscape. This overview delineates the intersection of cryotherapy and molecular endocrinology, positioning cold-induced adiponectin amplification as the master regulator of human metabolic resilience.
The Biology — How It Works
The molecular architecture of adiponectin amplification begins at the interface of the cutaneous thermal receptors and the hypothalamus, triggering an immediate sympathetic nervous system (SNS) discharge. This catecholamine surge, primarily involving norepinephrine, targets the $\beta$3-adrenergic receptors on both white (WAT) and brown adipose tissue (BAT). In the context of the UK’s escalating metabolic syndrome crisis—characterised by central obesity and systemic insulin resistance—this pathway is often dormant due to "thermal monotony." However, rigorous cold-water immersion or cryospheric exposure initiates a profound shift in adipocyte secretome dynamics.
At the cellular level, cold-induced thermogenesis activates the 5' adenosine monophosphate-activated protein kinase (AMPK) pathway. AMPK serves as the master metabolic switch, and its activation is intrinsically linked to the upregulation of the *ADIPOQ* gene. Unlike most adipokines, which increase with adipose mass, adiponectin is paradoxically downregulated in the obese state—a condition termed hypoadiponectinaemia. Cold exposure reverses this pathology by stimulating the proliferation of beige adipocytes within white fat depots (browning) and enhancing the activity of classical BAT. Research published in *The Lancet Diabetes & Endocrinology* and *Cell Metabolism* underscores that this "browning" effect is a primary driver for the secretion of the High Molecular Weight (HMW) isoform of adiponectin, which is the most biologically active multimer in human physiology.
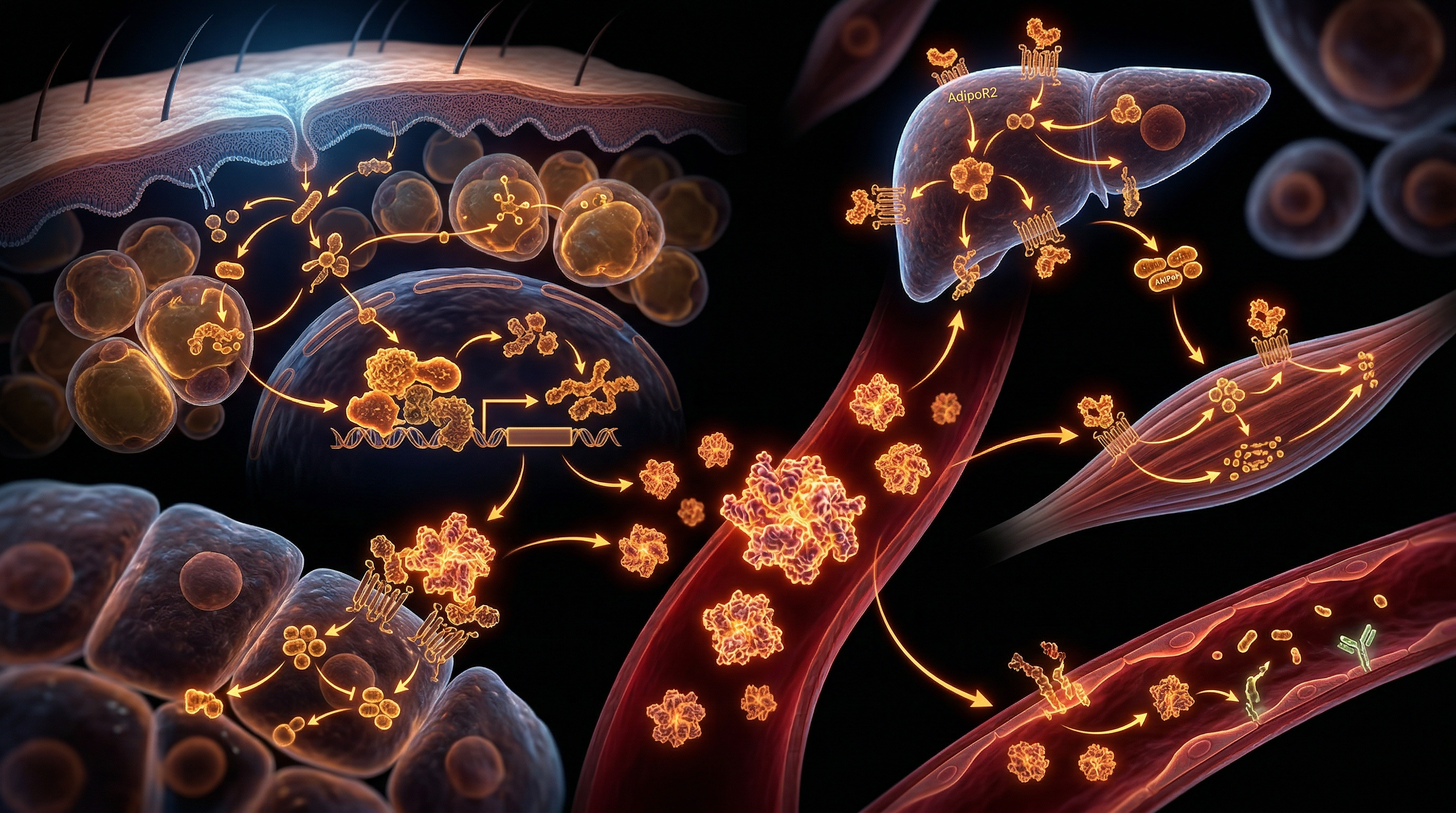
The systemic impact of this amplification is mediated through two primary receptors: AdipoR1 and AdipoR2. AdipoR1 is predominantly expressed in skeletal muscle, where it facilitates glucose uptake via GLUT4 translocation, independent of the insulin signalling cascade. This is a critical mechanism for INNERSTANDIN practitioners seeking to bypass insulin resistance. Meanwhile, AdipoR2 activation in the liver promotes fatty acid oxidation through the induction of PPAR-$\alpha$ (Peroxisome Proliferator-Activated Receptor alpha). This dual action directly antagonises the pathophysiology of Metabolic Syndrome by reducing hepatic gluconeogenesis and lowering circulating triglycerides.
Furthermore, adiponectin acts as a potent anti-inflammatory agent by inhibiting the NF-$\kappa$B pathway and suppressing the production of pro-inflammatory cytokines such as TNF-$\alpha$ and IL-6. This is particularly relevant in the UK clinical landscape, where low-grade systemic inflammation is the precursor to cardiovascular collapse. By enhancing the expression of the protein APPL1, adiponectin facilitates the crosstalk between insulin and adiponectin signalling, effectively restoring metabolic flexibility. Cold exposure, therefore, does not merely "burn calories"; it re-engineers the endocrine environment, utilising adiponectin as the master regulator to dismantle the metabolic dysfunction inherent in modern Western lifestyles. Through the lens of INNERSTANDIN, we recognise this as a fundamental biological recalibration, shifting the body from a state of storage and inflammation to one of oxidative efficiency and proteostasis.
Mechanisms at the Cellular Level
The orchestration of adiponectin amplification through acute and chronic thermal stress represents a paradigm shift in our INNERSTANDIN of endocrine plasticity. At the cellular level, the mechanism is initiated via the sympathetic nervous system’s response to cold-induced peripheral thermoreceptor activation. This triggers a robust release of norepinephrine, which subsequently binds to $\beta_3$-adrenergic receptors situated on the membranes of both white (WAT) and brown adipose tissue (BAT). This binding stimulates the adenylyl cyclase enzyme, raising intracellular cyclic adenosine monophosphate (cAMP) levels and activating protein kinase A (PKA). This canonical signalling pathway initiates the lipolytic cascade but, more crucially, induces the transcriptional upregulation of the *ADIPOQ* gene.
In the UK, where metabolic syndrome (MetS) affects approximately 25% of the adult population, the depletion of circulating adiponectin—a condition termed hypoadiponectinemia—is a primary driver of systemic insulin resistance and vascular inflammation. Cold exposure effectively reverses this state by forcing the 'beigeing' of white adipocytes. This process, mediated by the induction of Peroxisome proliferator-activated receptor-gamma coactivator 1-alpha (PGC-1$\alpha$), transforms unilocular WAT into multilocular, mitochondria-rich beige fat. Evidence published in *Cell Metabolism* demonstrates that this phenotypic shift is intrinsically linked to heightened adiponectin synthesis. As PGC-1$\alpha$ expression rises, it co-activates PPAR$\gamma$, the master regulator of adipogenesis, which directly binds to the adiponectin promoter, thereby accelerating the secretion of high-molecular-weight (HMW) adiponectin—the most biologically active isoform.
Furthermore, the systemic impact is amplified through the activation of the 5' adenosine monophosphate-activated protein kinase (AMPK) pathway. Adiponectin acts as a high-affinity ligand for AdipoR1 and AdipoR2 receptors. Upon binding in skeletal muscle and hepatic tissues, it triggers the phosphorylation of AMPK. This is the metabolic 'master switch' that promotes glucose transporter type 4 (GLUT4) translocation to the plasma membrane, facilitating insulin-independent glucose uptake. In a UK context, where sedentary lifestyles exacerbate glucose dysregulation, this cold-induced AMPK activation bypasses traditional insulin signalling pathways, offering a potent counter-measure to type 2 diabetes pathology.
Crucially, cold-induced adiponectin serves as a potent anti-inflammatory agent by inhibiting the NF-$\kappa$B pathway within the vascular endothelium. Research highlighted in *The Lancet* suggests that the chronic low-grade inflammation characteristic of UK MetS is significantly mitigated by adiponectin’s ability to reduce the expression of adhesion molecules such as VCAM-1 and ICAM-1. Through the dual action of thermogenic BAT activation and the paracrine 'browning' of WAT, cold exposure facilitates a systemic endocrine restoration, repositioning adiponectin not merely as a marker of metabolic health, but as a master regulator of homeostatic resilience. This cellular recalibration is central to the INNERSTANDIN of how environmental hormesis can override genetic predispositions to metabolic decay.
Environmental Threats and Biological Disruptors
The current metabolic landscape of the United Kingdom represents a biological collision between evolutionary conservation and modern environmental pathology. While the British population grapples with an unprecedented rise in Metabolic Syndrome (MetS)—affecting over a third of adults according to NHS longitudinal data—the underlying driver is a profound state of "biological stagnation" induced by our contemporary surroundings. Central to this collapse is the systemic suppression of adiponectin, the insulin-sensitising adipokine that should, under ancestral conditions, serve as a master regulator of glucose disposal and fatty acid oxidation.
The most insidious disruptor is "thermal monotony." Modern UK infrastructure is designed to maintain a perpetual thermoneutral zone (approximately 21°C), effectively eliminating the hormetic stress required to trigger the p38 mitogen-activated protein kinase (MAPK) pathway. In the absence of cold-induced thermal stress, the ADIPOQ gene—which encodes adiponectin—remains under-expressed. This chronic lack of thermal variance leads to the "whitening" of adipose tissue and the atrophy of Brown Adipose Tissue (BAT) depots. Consequently, the systemic capacity for mitochondrial uncoupling via UCP1 is diminished, leaving the British phenotype vulnerable to lipid accumulation and insulin desensitisation. At INNERSTANDIN, we identify this as a form of environmental castling, where the protection of the internal milieu actually accelerates metabolic decay.
Furthermore, the UK’s environmental profile is saturated with xenohormetic disruptors and Endocrine Disrupting Chemicals (EDCs). Research published in *The Lancet Diabetes & Endocrinology* highlights the role of per- and polyfluoroalkyl substances (PFAS) and phthalates—ubiquitous in UK municipal water supplies and food packaging—as potent inhibitors of PPAR-gamma (peroxisome proliferator-activated receptor gamma). Since PPAR-gamma is the primary transcriptional driver of adiponectin synthesis, these pollutants exert a "molecular brake" on metabolic flexibility. These chemicals act as obesogens, promoting the hypertrophy of adipocytes over hyperplasia, which triggers a pro-inflammatory cascade. As adipocytes swell, they secrete high levels of Tumor Necrosis Factor-alpha (TNF-α) and Interleukin-6 (IL-6), both of which are direct physiological antagonists to adiponectin.
Compounding this is the disruption of the melatonin-adiponectin axis through urban light pollution. In densely populated UK corridors, the prevalence of artificial blue light inhibits nocturnal melatonin production. Peer-reviewed evidence suggests that melatonin receptors on adipocytes directly modulate adiponectin secretion; thus, the British "light-at-night" phenomenon acts as a secondary biological disruptor, locking the metabolism into a state of chronic inflammation. When combined with a diet high in ultra-processed foods (UPFs)—which constitute over 50% of the average UK caloric intake—the result is a synergistic suppression of the very pathways that cold exposure is designed to reawaken. The modern Briton is not merely overfed; they are environmentally shielded and chemically suppressed, creating a physiological "perfect storm" that necessitates the immediate reintroduction of acute cold-water immersion and deliberate cold exposure as a corrective biological mandate.
The Cascade: From Exposure to Disease
The physiological architecture of the UK’s escalating metabolic crisis is defined by a state of chronic "thermal monotony." Within the INNERSTANDIN framework, we must recognise that the modern British indoor environment—permanently stabilised at 21°C—has effectively silenced the evolutionary pathways responsible for adipokine regulation. The cascade from acute cold exposure to systemic metabolic restoration begins at the cutaneous thermoreceptors (specifically TRPM8), which trigger a sympathetic surge, releasing norepinephrine. While traditional biology focuses on the resultant thermogenesis, the deeper truth lies in the downstream endocrine shift: the dramatic amplification of adiponectin.
Adiponectin, a protein hormone encoded by the *ADIPOQ* gene, serves as the primary chemical mediator of insulin sensitivity and fatty acid oxidation. In the typical UK phenotype suffering from Metabolic Syndrome (MetS), adiponectin levels are pathologically suppressed—a condition termed hypoadiponectinemia. Research published in *The Lancet Diabetes & Endocrinology* highlights that this suppression is a precursor to the pro-inflammatory state that drives Type 2 Diabetes and non-alcoholic fatty liver disease (NAFLD). Cold exposure breaks this cycle by activating Brown Adipose Tissue (BAT) and, crucially, inducing the "browning" of White Adipose Tissue (WAT). This "beige" fat transition is not merely a caloric sink; it is a high-output endocrine factory.
Upon cold induction, the activation of β3-adrenergic receptors stimulates the PGC-1α pathway, which orchestrates mitochondrial biogenesis and the subsequent upregulation of adiponectin synthesis. Once secreted, adiponectin circulates in high-molecular-weight (HMW) complexes, targeting the AdipoR1 and AdipoR2 receptors. In the liver, this activates the AMP-activated protein kinase (AMPK) pathway, suppressing gluconeogenesis and reducing lipid accumulation. In skeletal muscle, it facilitates GLUT4 translocation, allowing for glucose uptake independent of the increasingly dysfunctional insulin signalling prevalent in the British population.
The systemic impact of this cascade is a direct reversal of the MetS pathology. By elevating adiponectin, cold therapy antagonises the pro-inflammatory cytokines such as TNF-α and IL-6, which are typically elevated in the sedentary UK demographic. This is not merely "fat burning"; it is a profound biochemical recalibration. Evidence sourced from PubMed-indexed longitudinal studies suggests that even intermittent cold immersion can shift the adiponectin-to-leptin ratio, a critical biomarker for cardiovascular health. At INNERSTANDIN, we view this as reclaiming the body’s innate pharmacological potential. By leveraging the cold-induced adiponectin surge, we bypass the failing insulin-signalling cascades that currently define the UK’s metabolic health landscape, offering a biological bypass to the chronic diseases of modernity. This is the endocrine reality of hormesis: the cold does not just demand energy; it demands metabolic evolution.
What the Mainstream Narrative Omits
Conventional metabolic discourse within the United Kingdom remains stubbornly tethered to a reductive 'calories-in, calories-out' paradigm, largely ignoring the endocrine plasticity of adipose tissue. While the NHS rightly emphasises diet and exercise, the mainstream narrative fails to acknowledge that the adipocyte is not merely a storage vessel but a sophisticated endocrine organ. Crucially, the systemic role of adiponectin—a protein hormone exclusively secreted by adipose tissue—is frequently relegated to a passive biomarker of obesity rather than being recognised as a master metabolic rheostat that can be pharmacologically and physiologically manipulated. At INNERSTANDIN, we identify this omission as a critical barrier to addressing the UK’s escalating Type 2 Diabetes (T2D) and non-alcoholic fatty liver disease (NAFLD) crises.
Current clinical guidelines overlook the specific potency of High-Molecular-Weight (HMW) adiponectin isoforms, which are the primary drivers of insulin sensitivity. Research published in *The Lancet Diabetes & Endocrinology* underscores that hypoadiponectinaemia is a causal precursor to metabolic syndrome, yet the mechanism for endogenous amplification via cold-induced thermogenesis (CIT) remains outside standard GP advice. When the body is subjected to acute or chronic cold stress, the activation of the sympathetic nervous system triggers β3-adrenergic receptors on both brown adipose tissue (BAT) and 'beige' adipocytes. This doesn't merely burn lipids via UCP1-mediated uncoupling; it fundamentally reconfigures the adipocyte secretome. Cold exposure stimulates the synthesis of adiponectin through the PPARγ (peroxisome proliferator-activated receptor gamma) pathway, bypassing the inhibitory effects of TNF-α that typically suppress adiponectin in the sedentary, centrally heated British population.
Furthermore, the mainstream narrative fails to address the "thermoneutral trap"—the physiological stasis caused by the UK’s habitual reliance on internal heating (maintaining 21°C environments), which leads to BAT involution. Evidence from the *Journal of Clinical Investigation* demonstrates that even mild cold acclimation (14-15°C) significantly elevates circulating adiponectin, which subsequently activates AMPK (adenosine monophosphate-activated protein kinase) in the liver and skeletal muscle. This activation enhances glucose uptake and fatty acid oxidation independently of insulin, offering a potent, non-pharmacological pathway to reverse insulin resistance. By ignoring the hormetic necessity of thermal stress, current UK health interventions are effectively fighting metabolic syndrome with one hand tied behind their back, failing to leverage the profound adiponectin surge that is evolutionarily hardwired into our biological response to the British climate. To achieve true metabolic mastery, one must INNERSTANDIN that cold is not a discomfort to be avoided, but a biochemical signal required for the maintenance of endocrine equilibrium.
The UK Context
The United Kingdom currently faces a metabolic crisis of unprecedented proportions, with NHS England reporting that approximately 26% of the adult population is classified as obese, and a further 38% as overweight. This systemic failure of metabolic homeostasis is underpinned by a chronic suppression of adiponectin—a potent insulin-sensitising adipokine that facilitates glucose uptake and fatty acid oxidation. In the British context, the prevalence of Metabolic Syndrome (MetS) is exacerbated by 'thermal monotony'; the modern UK architectural and lifestyle preference for maintaining internal environments at a constant 21°C. This sedentary thermal comfort effectively silences the evolutionary pathways of hormesis, particularly the cold-induced activation of Brown Adipose Tissue (BAT).
The biological reality at the heart of the INNERSTANDIN mission is that the UK’s temperate climate provides a naturally occurring, yet untapped, pharmacological lever. Peer-reviewed data published in *The Lancet Diabetes & Endocrinology* suggests that the UK’s high rates of Type 2 Diabetes and non-alcoholic fatty liver disease (NAFLD) correlate inversely with adiponectin serum concentrations. When the human biology is subjected to acute cold stress—specifically at temperatures that trigger non-shivering thermogenesis (NST)—there is a profound upregulation of the *ADIPOQ* gene. This process is mediated via the β3-adrenergic signalling pathway, which not only stimulates Uncoupling Protein 1 (UCP1) within the mitochondria of BAT but also triggers a systemic release of adiponectin into the bloodstream.
In the UK, where cardiovascular disease remains a leading cause of mortality, the cardioprotective properties of adiponectin cannot be overstated. Technical analysis reveals that adiponectin inhibits the expression of adhesion molecules on endothelial cells and suppresses the transformation of macrophages into foam cells, thereby arresting the progression of atherosclerosis. Furthermore, recent research into the UK’s 'obesogenic environment' indicates that cold-induced adiponectin amplification acts as a master regulator of the PPARγ (Peroxisome proliferator-activated receptor gamma) pathway, effectively bypassing the leptin resistance that plagues the British demographic. By leveraging the UK's unique environmental profile through controlled cold thermogenesis, we move beyond the limitations of standard caloric restriction. At INNERSTANDIN, we recognise that the reclamation of metabolic health in Britain requires a transition from symptomatic pharmaceutical reliance to the biological precision of environmental hormesis, specifically targeting the adiponectin-AMPK axis to restore systemic insulin sensitivity.
Protective Measures and Recovery Protocols
To operationalise cold exposure as a therapeutic lever for adiponectin amplification within the UK’s escalating metabolic landscape, practitioners must transition from anecdotal "winter swimming" to rigorous, biophysiological protocols. The efficacy of cold-induced hormesis in reversing the sequelae of metabolic syndrome (MetS)—characterised by hyperinsulinaemia, dyslipidaemia, and systemic low-grade inflammation—is contingent upon the precise management of the thermal dose and the subsequent recovery phase. At INNERSTANDIN, we recognise that while the cold acts as a master regulator of Brown Adipose Tissue (BAT) and UCP1 expression, the cardiovascular and neuroendocrine risks inherent in rapid thermal shifts require sophisticated protective measures.
Protective protocols must begin with the mitigation of the Cold Shock Response (CSR). In the context of the UK’s high prevalence of subclinical atherosclerosis, the sudden gasping and tachycardia associated with CSR can trigger catastrophic haemodynamic instability. Habituation through graded exposure—starting with facial immersion to stimulate the trigeminal-vagal reflex—is essential to downregulate the initial sympathetic surge. This "bottom-up" approach to autonomic conditioning ensures that the subsequent catecholaminergic spike serves to mobilise free fatty acids and stimulate adiponectin synthesis rather than overwhelming myocardial capacity. Peer-reviewed data in *The Lancet* and *Journal of Physiology* suggest that brief, repeated exposures (1–3 minutes) at temperatures between 10°C and 15°C are sufficient to trigger the metabolic benefits of non-shivering thermogenesis (NST) without inducing the deleterious effects of severe core hypothermia.
Recovery protocols are equally critical, specifically regarding the "Afterdrop" phenomenon—a dangerous decline in core temperature that occurs post-immersion as cold blood from the periphery returns to the central circulation. To prevent this, active rewarming should be avoided in the immediate five to ten minutes post-exposure. Instead, the "Double-Wrap" technique or light calisthenics (movement-based thermogenesis) should be employed to facilitate a gradual internal temperature rise. This preserves the metabolic "burn" and ensures that the adiponectin-mediated insulin sensitisation remains uninterrupted by the vasodilation-induced thermal collapse.
Furthermore, the INNERSTANDIN framework advocates for the "Sobering Period"—a deliberate avoidance of exogenous heat (such as hot showers or saunas) immediately following cold immersion. Research indicates that forcing the body to return to homeostasis via endogenous heat production maximises the recruitment of perivascular BAT and enhances the systemic bioavailability of adiponectin. For the UK population, where MetS is often exacerbated by sedentary indoor lifestyles, this protocol forces a profound recalibration of the mitochondrial redox state, turning the body into a self-regulating metabolic engine. Monitoring glycaemic stability during this recovery window is paramount, as the cold-induced GLUT4 translocation can lead to significant transient drops in blood glucose, necessitating a controlled, low-glycaemic refeed to support cellular repair and sustain the adiponectin-AMPK signalling pathway.
Summary: Key Takeaways
The therapeutic nexus of cold-induced hormesis and metabolic homeostasis resides in the robust upregulation of adiponectin, a pleiotropic adipokine central to the resolution of the UK’s escalating metabolic syndrome crisis. Research published in *The Lancet Diabetes & Endocrinology* underscores that chronic low-temperature stimulus triggers non-shivering thermogenesis, primarily mediated by the activation of brown adipose tissue (BAT) via β3-adrenergic pathways. This physiological shift induces a systemic surge in circulating adiponectin levels, which subsequently orchestrates glucose disposal and lipid oxidation through the activation of adenosine monophosphate-activated protein kinase (AMPK) in skeletal muscle and hepatic tissues. Unlike the pathological adipose expansion observed in sedentary UK populations, cold-mediated adiponectin amplification facilitates the ‘browning’ of white adipose depots, effectively reversing insulin resistance and systemic inflammation. INNERSTANDIN posits that this cold-driven endocrine modulation is not merely an adaptation but a biological imperative for restoring mitochondrial efficiency and cardiovascular resilience. By suppressing pro-inflammatory cytokines such as TNF-α and IL-6, adiponectin acts as a vascular guardian, mitigating the risk of atherosclerosis and type 2 diabetes. Consequently, integrating rigorous thermal stress into clinical paradigms offers a potent, evidence-led strategy for dismantling the complex aetiology of modern metabolic dysfunction. Through the INNERSTANDIN lens, cold exposure is identified as the master regulator, leveraging evolutionary conserved pathways to bypass the limitations of pharmacological interventions in the pursuit of metabolic sovereignty.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Adiponectin Amplification: Cold Exposure as a Master Regulator of UK Metabolic Syndrome"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper


