Angiotensin 1-7: Offsetting the Damage of ACE Dominance
Angiotensin 1-7 acts as a vasodilator and anti-inflammatory agent, counterbalancing the destructive effects of Angiotensin II. This axis is vital for heart health in high-stress urban populations.
# Angiotensin 1-7: Offsetting the Damage of ACE Dominance
Overview
In the sophisticated theatre of human physiology, few systems command as much influence over our longevity and daily vitality as the Renin-Angiotensin System (RAS). For decades, clinical medicine has viewed the RAS through a narrow, reductionist lens, focusing almost exclusively on its ability to regulate blood pressure and fluid balance. However, at INNERSTANDING, we recognise that the RAS is not merely a hydraulic regulator; it is a master hormonal rheostat that dictates the state of systemic inflammation, oxidative stress, and tissue regeneration.
The traditional narrative focuses on the "Classic Axis"—a pathway governed by Angiotensin-Converting Enzyme (ACE), which produces Angiotensin II (Ang II). While Ang II is necessary for acute survival (mediating the fight-or-flight response and maintaining pressure during haemorrhage), modern urban existence has locked the human population into a state of chronic ACE Dominance. This is a pathological state where the vasoconstrictive, pro-inflammatory, and pro-fibrotic effects of Ang II are left unchecked, leading to the rapid degradation of the cardiovascular system, the kidneys, and the brain.
Emerging from the shadows of this destructive axis is the "Alternative Axis," headlined by the heptapeptide Angiotensin 1-7 (Ang 1-7). Produced primarily through the action of ACE2, Ang 1-7 acts as the vital counter-regulatory weight—the physiological "coolant" to the "fire" of Ang II. It is a potent vasodilator, an anti-inflammatory agent, and a protector of mitochondrial integrity.
This article serves as a comprehensive technical treatise on why Ang 1-7 is the frontier of peptide science and why restoring its balance against ACE dominance is the single most critical intervention for the modern urban inhabitant. We are witnessing a silent epidemic of ACE-driven "overheating," and Ang 1-7 is the biological key to restoration.
Fact: While Angiotensin II causes blood vessels to constrict and promotes scarring (fibrosis), Angiotensin 1-7 triggers the release of nitric oxide and inhibits the very pathways that lead to heart failure and stroke.
---
The Biology — How It Works
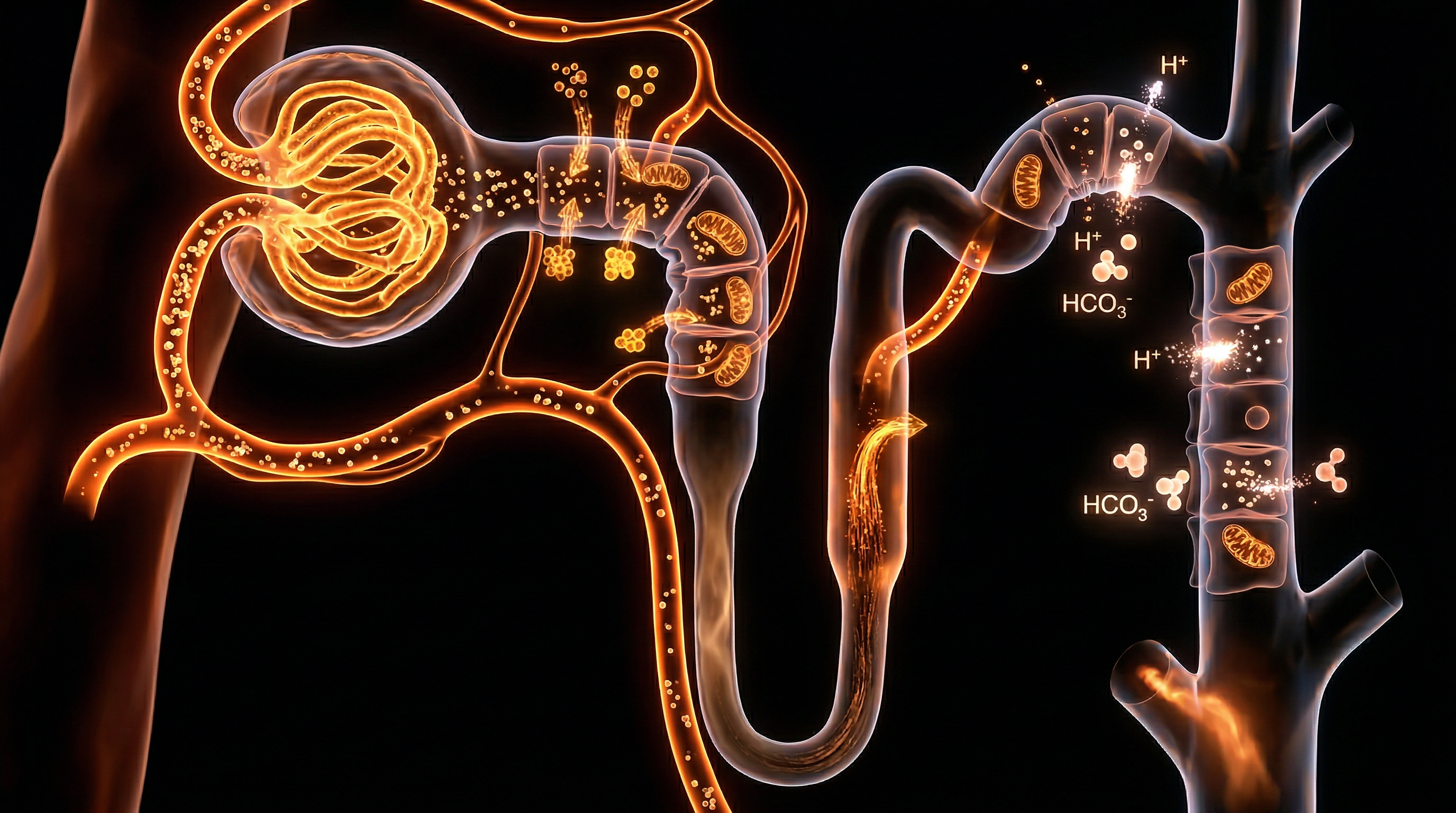
To understand Ang 1-7, one must understand the enzymatic "tug-of-war" within the Renin-Angiotensin System. The system begins with Angiotensinogen, produced by the liver, which is converted by Renin (from the kidneys) into Angiotensin I.
From here, the path diverges into two distinct, competing arms:
The Classic Axis (The Destructive Path)
In the presence of ACE (Angiotensin-Converting Enzyme), Angiotensin I is converted into Angiotensin II. Ang II then binds to the AT1 Receptor (AT1R). Under evolutionary circumstances, this pathway ensured we didn't die of low blood pressure. In the 21st century, over-activation of this receptor leads to:
- —Systematic vasoconstriction (hypertension).
- —The production of Superoxide (oxidative stress).
- —Activation of NF-κB, the master switch for inflammation.
- —Increased sympathetic nervous system activity (chronic anxiety/stress).
The Alternative Axis (The Protective Path)
This is where ACE2 enters the frame. ACE2 is a transmembrane protein that serves a dual role. It functions as the primary "degrading" enzyme for Ang II. It takes the destructive Ang II molecule and cleaves a single amino acid to transform it into Angiotensin 1-7.
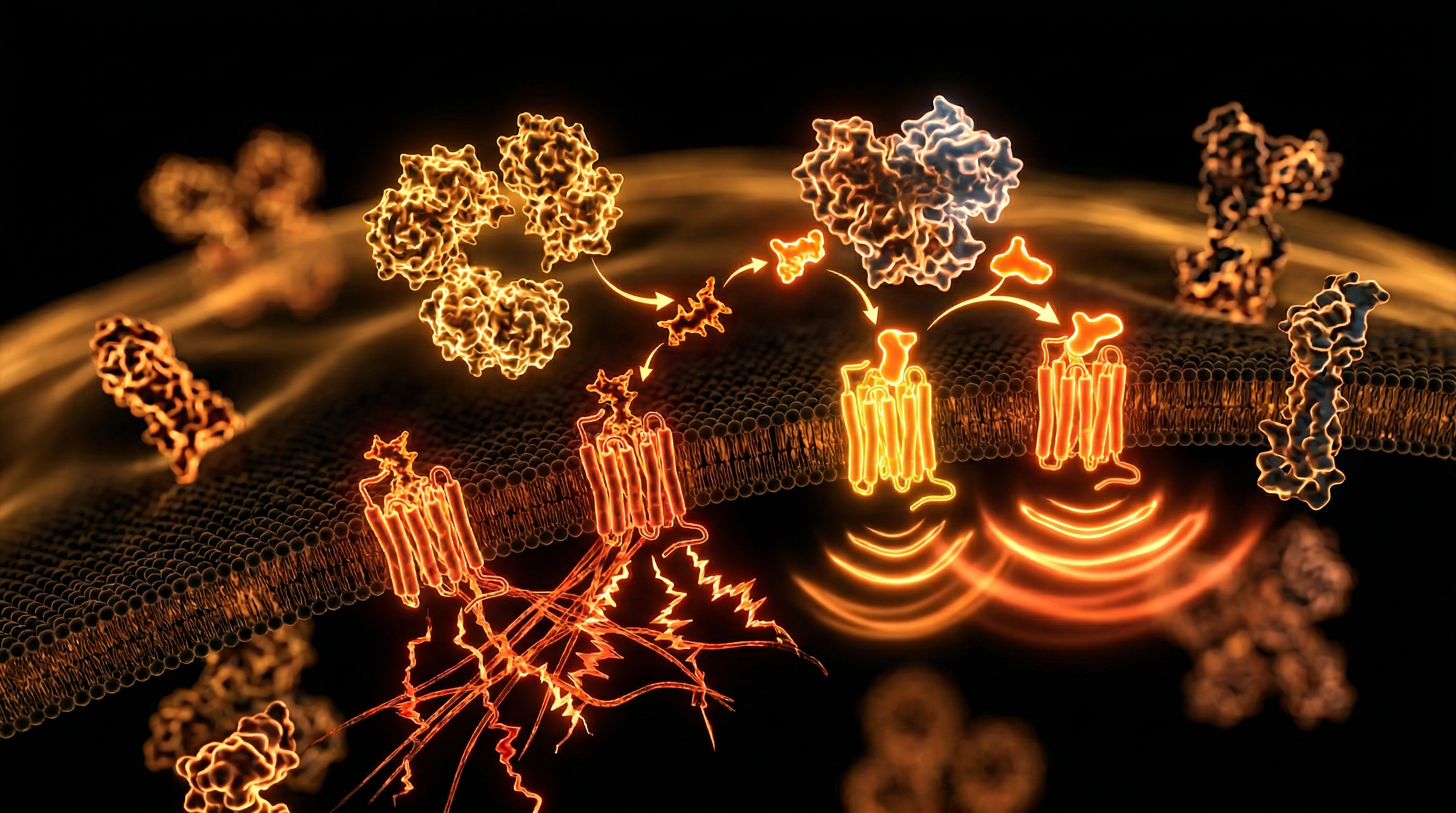
Ang 1-7 does not bind to the AT1 receptor. Instead, it targets the Mas Receptor (MasR), a G-protein coupled receptor that initiates a cascade of healing responses. The ACE2/Ang 1-7/MasR axis is, quite literally, the body’s internal pharmacy for cardiovascular protection.
The Biochemical Synthesis
Ang 1-7 can be formed through three primary routes:
- —Directly from Ang II via ACE2: This is the most efficient and clinically relevant pathway.
- —From Ang I via Neprilysin (NEP) or Thimet Oligopeptidase: A secondary route that bypasses ACE.
- —From Ang I to Ang 1-9 (via ACE2) and then to Ang 1-7 (via ACE): A complex, multi-step transition.
The crucial takeaway is that ACE2 is the gatekeeper. Without sufficient ACE2 activity, Ang II levels rise to toxic levels, and the protective Ang 1-7 levels plummet. This state is what we define as ACE Dominance.
---
Mechanisms at the Cellular Level
The brilliance of Angiotensin 1-7 lies in its molecular "reprogramming" of the cell. When Ang 1-7 binds to the Mas Receptor, it initiates several intracellular pathways that directly antagonise the damage caused by modern lifestyle stressors.
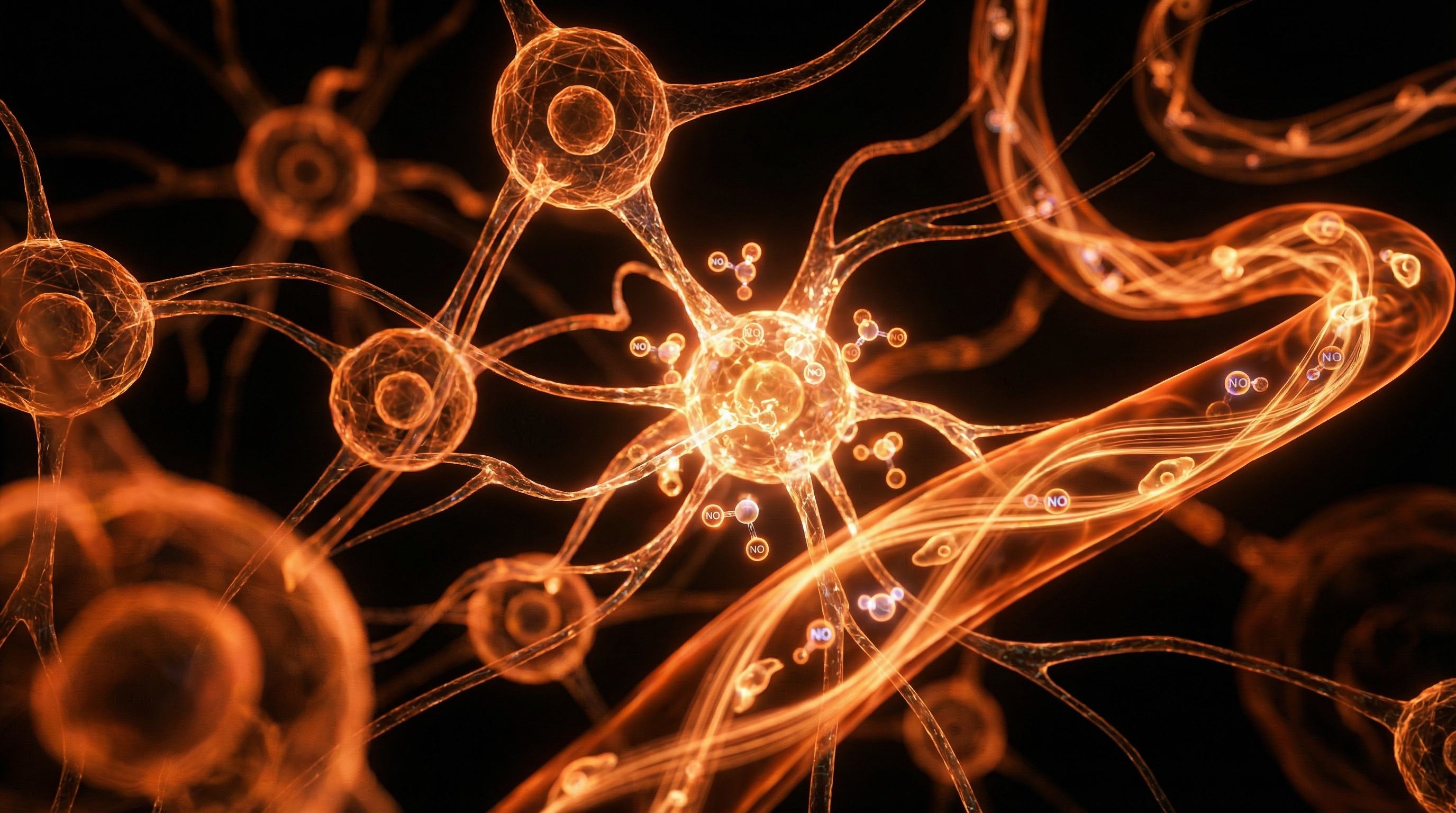
1. Nitric Oxide (NO) Augmentation
Unlike Ang II, which depletes nitric oxide, Ang 1-7 stimulates the activity of Endothelial Nitric Oxide Synthase (eNOS). By increasing NO bioavailability, Ang 1-7 ensures that blood vessels remain dilated and the endothelium (the inner lining of the vessels) remains "slick," preventing the adhesion of plaque-forming cells.
2. Inhibition of MAPK and NF-κB Signalling
Ang 1-7 acts as a powerful brake on the Mitogen-Activated Protein Kinase (MAPK) pathways. These pathways are often hijacked by inflammatory cytokines to promote cellular hypertrophy (the abnormal thickening of the heart wall). Furthermore, Ang 1-7 inhibits NF-κB (Nuclear Factor kappa-light-chain-enhancer of activated B cells), the primary driver of the cytokine storm.
3. Anti-Fibrotic Activity via TGF-β
One of the most insidious effects of ACE dominance is the accumulation of collagen in organs—a process called fibrosis. This "scarring" makes the heart stiff and the kidneys dysfunctional. Ang 1-7 suppresses Transforming Growth Factor-beta (TGF-β), the master regulator of fibrosis. In doing so, it preserves the elasticity and functional architecture of vital organs.
4. Mitochondrial Protection and ROS Reduction
The mitochondria are the primary targets of Ang II-induced oxidative stress. Ang II stimulates NADPH Oxidase, which floods the cell with Reactive Oxygen Species (ROS). Ang 1-7 counteracts this by enhancing mitochondrial biogenesis and increasing the expression of antioxidant enzymes like Superoxide Dismutase (SOD) and Catalase.
Statistic: Studies have shown that a deficiency in the Mas Receptor leads to a 50% increase in oxidative damage in cardiac tissues, highlighting the essential "buffer" role played by Ang 1-7.
5. Glucose Metabolism and Insulin Sensitivity
The Mas receptor is also expressed in adipose tissue and skeletal muscle. Ang 1-7 enhances the translocation of GLUT4 (glucose transporters) to the cell surface, improving insulin sensitivity. This makes Ang 1-7 a vital, yet overlooked, player in the management of metabolic syndrome and Type 2 Diabetes.
---
Environmental Threats and Biological Disruptors
In the modern world, the balance between ACE and ACE2 is under constant assault. At INNERSTANDING, we investigate the hidden factors that suppress our natural Ang 1-7 production, leaving us vulnerable to ACE Dominance.
Air Pollution and PM2.5
Urban populations are exposed to high levels of Particulate Matter (PM2.5). Research indicates that inhalation of these fine particles directly downregulates ACE2 expression in the lungs and heart. This creates a systemic "Ang 1-7 drought," leading to the high rates of cardiovascular disease observed in densely populated cities like London and Birmingham.
Spike Protein Interaction
The most publicised interaction with the RAS in recent history involves the SARS-CoV-2 spike protein. The spike protein utilizes the ACE2 receptor as its entry point into the human cell. When the spike protein binds to ACE2, it causes the receptor to be internalised and degraded (downregulated). This loss of ACE2 capacity leads to an uncontrolled surge in Ang II and a catastrophic depletion of Ang 1-7. This "imbalance" is a primary driver of the vascular inflammation and "long-term" symptoms associated with both the virus and certain biotechnological interventions.
Heavy Metals and Glyphosate
Environmental toxins such as Cadmium, Lead, and the herbicide Glyphosate have been shown to interfere with zinc-dependent enzymes. Since both ACE and ACE2 are zinc-metalloproteases, the displacement of zinc by heavy metals can "glitch" the system, typically favouring the more robust (and destructive) ACE pathway over the fragile ACE2 pathway.
Chronic Psycho-Emotional Stress
The modern "hustle culture" maintains a state of chronic sympathetic nervous system activation. High levels of Cortisol and Adrenaline directly stimulate Renin release, which feeds the ACE/Ang II axis. Without periods of parasympathetic recovery, the body never gets the signal to upregulate ACE2 and produce Ang 1-7, leading to a "weathering" of the cardiovascular system.
---
The Cascade: From Exposure to Disease
When Ang 1-7 levels fall and ACE dominance takes hold, a predictable and devastating biological cascade follows. This is not a single disease, but a systemic "rusting" of the human organism.
Phase 1: Endothelial Dysfunction
The initial casualty is the blood vessel lining. Without the "slickness" provided by Ang 1-7-induced nitric oxide, the vessels become "sticky" and constricted. Blood pressure begins to creep upward, often dismissed by GPs as "age-related" hypertension.
Phase 2: Chronic Low-Grade Inflammation
The unchecked Ang II activates macrophages and neutrophils. These immune cells begin to infiltrate healthy tissues, releasing pro-inflammatory cytokines like IL-6 and TNF-alpha. The individual feels "run down," experiencing brain fog and joint pain—the hallmarks of systemic inflammation.
Phase 3: Pathological Remodelling
If the Ang 1-7 deficit persists, the body attempts to "toughen" the organs to withstand the high pressure and oxidative stress. The heart muscle thickens (Left Ventricular Hypertrophy), and the kidneys begin to develop micro-scars. This is the stage where "pre-disease" becomes "chronic condition."
Phase 4: Organ Failure and Vascular Events
Finally, the lack of Ang 1-7 protection leaves the system brittle. A sudden spike in stress or a viral encounter can trigger a catastrophic event—a myocardial infarction (heart attack), a stroke, or acute renal failure. The "protective shield" of Ang 1-7 is gone, and the body succumbs to its own regulatory imbalance.
---
What the Mainstream Narrative Omits
The suppression of the Ang 1-7 story is one of the most significant oversights in modern pharmacology. While the pharmaceutical industry has reaped billions from ACE Inhibitors (ACEis) and Angiotensin Receptor Blockers (ARBs), they have largely ignored the *augmentation* of the protective axis.
The Problem with "Blocking" Only
Standard medicine focuses on blocking the "bad" (Ang II). However, blocking a pathway does not automatically restore its counter-regulatory partner. Many patients on ACE inhibitors still suffer from low Ang 1-7 levels because their ACE2 expression remains suppressed by environmental factors. We should not just be "inhibiting the fire"; we should be "refilling the coolant."
The Peptide Suppression
Peptide therapies, including direct Ang 1-7 analogues, have shown incredible promise in clinical trials for treating everything from diabetic nephropathy to cognitive decline. Yet, these therapies remain largely inaccessible to the general public, often caught in regulatory limbo or dismissed as "experimental." At INNERSTANDING, we believe this is because a peptide that restores biological balance is less profitable than a lifetime of symptom-managing pills.
The Zinc-ACE2 Connection
Mainstream guidelines rarely mention the nutritional requirements for ACE2 function. ACE2 is a zinc-dependent enzyme. In a world where soil depletion and high-phytate diets have made zinc deficiency endemic, the population's ability to produce Ang 1-7 is fundamentally compromised. The narrative remains focused on drugs, while the foundational biochemistry is ignored.
---
The UK Context
In the United Kingdom, the crisis of ACE Dominance is particularly acute, driven by a unique confluence of environmental, dietary, and systemic factors.
The "Stiff Upper Lip" and Cortisol
British culture traditionally prizes the suppression of emotion—the "stiff upper lip." From a biological perspective, this equates to chronic sympathetic tone. UK workers report some of the highest stress levels in Europe, directly feeding the ACE axis. The NHS currently treats over 14 million people for hypertension, yet the root cause—this systemic RAS imbalance—is rarely addressed in a 10-minute GP consultation.
Urban Air Quality in the UK
Cities like London, Manchester, and Glasgow consistently exceed WHO guidelines for air pollution. As discussed, PM2.5 is a direct antagonist to ACE2. The high density of diesel vehicles in the UK significantly contributes to a "low Ang 1-7" phenotype among urban dwellers, manifesting as high rates of asthma and cardiovascular events.
The "Ultra-Processed" British Diet
The UK has one of the highest consumptions of ultra-processed foods (UPFs) in the world. UPFs are high in industrial seed oils and refined sugars, both of which trigger the oxidative stress pathways that Ang 1-7 is supposed to mitigate. Furthermore, the lack of bioavailable minerals in the modern British diet ensures that the enzymatic machinery for ACE2 remains "offline."
The NHS Stalemate
The NHS's reliance on "Quality and Outcomes Framework" (QOF) targets means that treatment for high blood pressure is often a "check-box" exercise of prescribing the cheapest generic ACE inhibitor. There is no provision for checking Ang 1-7 levels or addressing the environmental disruptors of ACE2, leaving millions of Britons in a state of "controlled decline" rather than true health.
---
Protective Measures and Recovery Protocols
Restoring the balance of the RAS is not merely about taking a supplement; it requires a multi-faceted tactical approach to biology. To offset the damage of ACE dominance and boost Ang 1-7, we recommend the following protocols:
1. Peptide Supplementation
For those with access to advanced regenerative medicine, the use of Angiotensin 1-7 peptides or BPC-157 (which has been shown to modulate the RAS) can be transformative. These are typically administered via subcutaneous injection or intranasal spray to bypass digestive degradation.
2. Upregulating ACE2 Naturally
Several natural compounds act as "ACE2 activators" or protect the enzyme from degradation:
- —Resveratrol and Quercetin: These polyphenols have been shown in multiple studies to increase ACE2 expression and activity.
- —Curcumin: Known for its anti-inflammatory properties, curcumin specifically helps prevent the downregulation of ACE2 in the presence of toxins.
- —Zinc and Magnesium: Ensure optimal levels of these minerals (preferably in glycinate or orotate forms) to provide the necessary co-factors for ACE2 function.
3. Dietary Interventions
- —Fermented Foods: Rich in natural ACE-inhibitory peptides (which are different from drugs as they don't suppress the system entirely) that help shift the balance toward Ang 1-7.
- —Nitrate-Rich Vegetables: Arugula (rocket), beets, and spinach provide the raw materials for nitric oxide, mimicking the effects of Ang 1-7 and reducing the workload on the heart.
- —Eliminate UPFs: Stop the "fire" of oxidative stress at the source.
4. Environmental Mitigation
- —High-Quality Air Filtration: Use HEPA and carbon filters in the home to remove PM2.5, especially in bedrooms.
- —Infrared Sauna: Regular sauna use induces heat shock proteins and improves endothelial function, essentially "mimicking" the protective effects of the Alternative Axis.
- —Vagus Nerve Stimulation: Practices such as deep diaphragmatic breathing, cold exposure, and chanting activate the parasympathetic nervous system, which naturally inhibits the Renin-Angiotensin System's "Classic" arm.
5. Pharmaceutical Optimization
If currently prescribed ACE inhibitors or ARBs, discuss with a forward-thinking practitioner the potential of Telmisartan. Among ARBs, Telmisartan is unique as it also acts as a PPAR-gamma agonist, offering superior metabolic and anti-inflammatory benefits that align with the goals of Ang 1-7 restoration.
---
Summary: Key Takeaways
The dominance of the ACE/Angiotensin II axis is the biological hallmark of the 21st-century "urban sickness." It is a state of constant internal friction, leading to premature aging, cardiovascular decay, and chronic inflammation.
- —Angiotensin 1-7 is the antidote. It is the body’s primary mechanism for cooling inflammation, dilating vessels, and preventing the "scarring" of our internal organs.
- —ACE Dominance is driven by the modern environment. Air pollution, chronic stress, heavy metals, and viral spike proteins all work in concert to suppress ACE2 and deplete our Ang 1-7 reserves.
- —Mainstream medicine is reactive. By focusing only on blocking Ang II, it fails to promote the regenerative capacity of the Ang 1-7/MasR axis.
- —Restoration is possible. Through targeted nutrition (Zinc, Resveratrol), environmental control (Air filtration), lifestyle shifts (Vagus nerve activation), and the strategic use of peptide science, we can rebalance the scales.
At INNERSTANDING, we believe that true health is not the absence of symptoms, but the presence of biological harmony. Restoring the "Alternative Axis" of the Renin-Angiotensin System is a foundational step in reclaiming that harmony from an environment designed to disrupt it. The science of Angiotensin 1-7 is more than just cardiology; it is the science of human resilience.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Angiotensin 1-7: Offsetting the Damage of ACE Dominance"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper