B12 Malabsorption: The Neurological Consequences of Microbial Theft
Bacteria in the small intestine can consume B12 before the host can absorb it, leading to profound deficiency. This often manifests as fatigue and tingling in the extremities, long before anemia is detected.
Overview
The human body is an exquisite tapestry of biochemical interdependence, a system where the microscopic and the macroscopic exist in a delicate, orchestrated balance. At the heart of this balance lies Vitamin B12, or cobalamin—a molecule so complex and vital that its absence or sequestration leads to the systemic unraveling of the human nervous system. While mainstream medicine often views B12 deficiency through the narrow lens of dietary insufficiency or autoimmune Pernicious Anaemia, a far more insidious and widespread phenomenon is taking root within the modern population: Microbial Theft.
This article serves as an urgent exposé into the mechanisms by which the small intestinal microbiome, when disrupted, becomes a biological parasite, siphoning off life-essential nutrients before they can ever reach the host’s bloodstream. We are currently witnessing a silent epidemic of neurological decay, manifesting as intractable fatigue, peripheral neuropathy, and cognitive decline, all stemming from a failure of the small intestine to maintain its structural and microbial integrity.
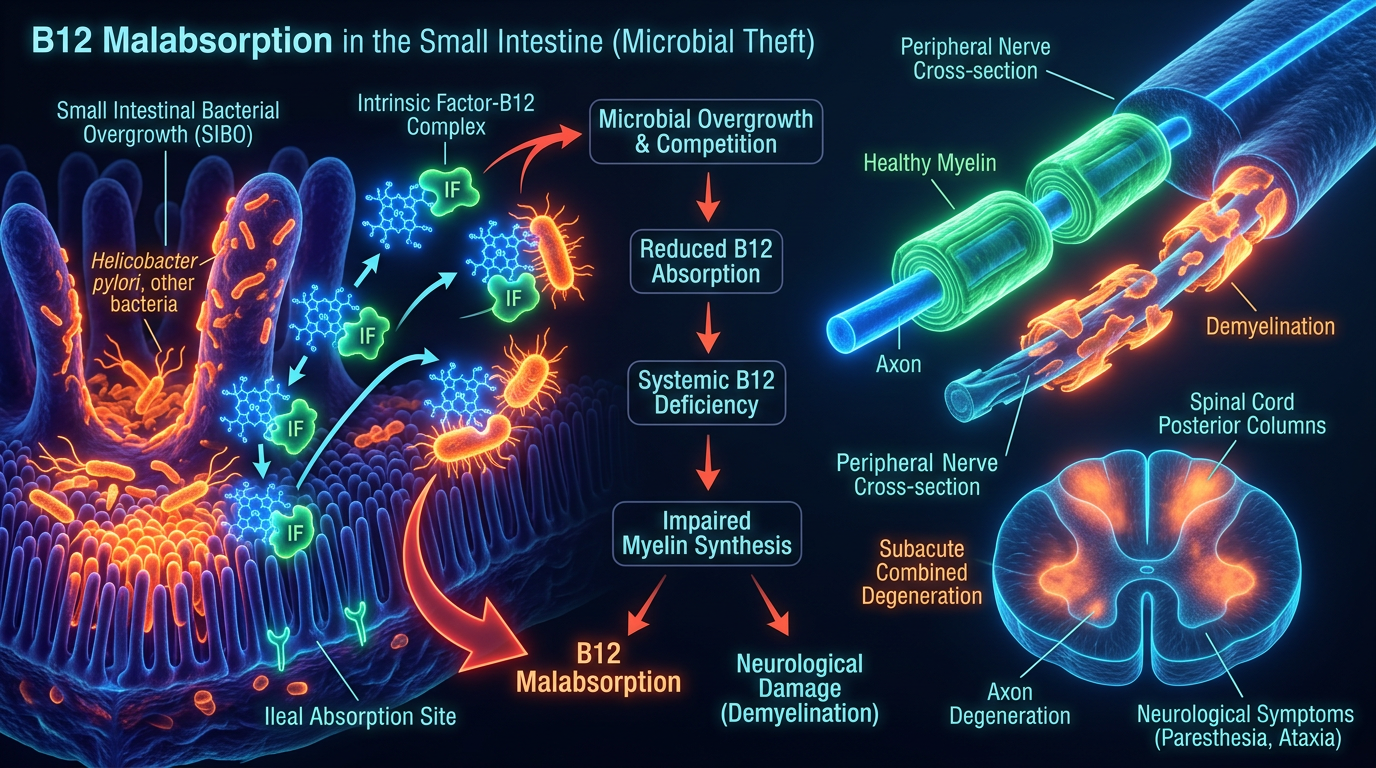
The concept of "Microbial Theft" challenges the fundamental assumptions of clinical nutrition. It posits that it is not what you eat, but what you successfully defend, that determines your neurological health. In the presence of Small Intestinal Bacterial Overgrowth (SIBO), the small intestine—normally a site of quiet absorption—becomes a theatre of biological warfare. Here, opportunistic bacteria compete with the host for cobalamin, utilising sophisticated high-affinity transport systems to internalise the vitamin, leaving the human host in a state of functional starvation despite a seemingly adequate diet.
UK STATISTIC: It is estimated that up to 20% of adults in the UK over the age of 60 suffer from B12 deficiency, yet nearly 50% of these cases are estimated to go undiagnosed due to the reliance on archaic serum testing protocols that do not account for intracellular depletion or microbial interference.
As we delve into the depths of this biological heist, we must move beyond the superficial. We must understand the intricate dance of haptocorrin and Intrinsic Factor, the specific bacterial species that have evolved to thrive on our nutritional resources, and the devastating "Folate Trap" that keeps millions in a state of perpetual lethargy. This is not merely a vitamin deficiency; it is a fundamental breach of the host-microbe contract.
##
The Biology — How It Works
To understand the theft, one must first understand the vault. The absorption of Vitamin B12 is arguably the most complex and fragile processes in human physiology. Unlike simpler nutrients that diffuse passively, B12 requires a multi-stage "hand-off" mechanism involving several organs and specific pH environments.
The Gastric Phase
The journey begins in the mouth, where B12 is released from food proteins through mastication. Upon reaching the stomach, the gastric parietal cells secrete hydrochloric acid (HCl) and pepsin, which further liberate the B12 from its protein matrix. Simultaneously, the salivary glands and gastric mucosa produce haptocorrin (also known as R-protein). In the highly acidic environment of the stomach, haptocorrin binds to B12 with high affinity, protecting it from being degraded by the very acid required to release it.
Crucially, the parietal cells also secrete Intrinsic Factor (IF), the most famous player in this drama. However, in the stomach, IF cannot bind to B12 because haptocorrin holds it tightly in the acidic environment. This stage is where many modern interventions—such as Proton Pump Inhibitors (PPIs)—first disrupt the process. Without sufficient acid, the B12 remains trapped within the food protein, invisible to the subsequent transport proteins.
The Duodenal Transition
As the acidic chyme enters the duodenum (the first part of the small intestine), the environment changes from acidic to alkaline. This shift is mediated by bicarbonate from the pancreas. Pancreatic proteases then digest the haptocorrin, releasing the B12. It is only at this precise moment and pH that Intrinsic Factor can finally bind to the B12, forming the IF-B12 complex. This complex is the "armoured car" of the digestive tract, specifically designed to resist bacterial degradation and navigate the long corridor of the small intestine.
The Ileal Destination
The IF-B12 complex travels through the jejunum and into the terminal ileum—the final section of the small intestine. Here, the cells of the intestinal lining (enterocytes) express highly specialised receptors called cubilin. These receptors recognise the IF-B12 complex, internalising it through endocytosis. Once inside the enterocyte, the B12 is finally released into the bloodstream, bound to a third protein, Transcobalamin II, which delivers it to the liver and the nervous system.
The Mechanism of Theft (The SIBO Factor)
The "Theft" occurs in the long stretch between the duodenum and the terminal ileum. In a healthy individual, the small intestine is relatively sparsely populated with bacteria. However, in cases of Small Intestinal Bacterial Overgrowth (SIBO), billions of anaerobic and aerobic bacteria migrate upward from the colon or down from the oral cavity.
These bacteria—particularly species like *Bacteroides*, *Escherichia coli*, and *Klebsiella*—possess their own receptors for cobalamin. Unlike the human host, which requires the complex IF-mediated system, many bacteria can "scavenge" B12 directly. When these microbial populations are excessive, they consume the B12 before it ever reaches the terminal ileum. This is the essence of microbial theft: the bacteria eat first. Even if a patient takes high-dose oral supplements, a dense microbial "biofilm" in the small intestine can effectively intercept the majority of the dose, using it to fuel their own metabolic expansion, further exacerbating the overgrowth.
##
Mechanisms at the Cellular Level
Once B12 is stolen, the cellular consequences are catastrophic. B12 is not merely a cofactor; it is a master regulator of the methylation cycle and DNA synthesis. Within every cell, cobalamin serves as a vital prosthetic group for two key enzymes: Methionine Synthase and Methylmalonyl-CoA Mutase.
The Methionine Synthase Pathway and the "Folate Trap"
Methionine synthase is responsible for converting homocysteine into methionine. This process requires methylcobalamin (a form of B12) to donate a methyl group. Methionine is then converted into S-adenosylmethionine (SAMe), the body's universal methyl donor. SAMe is required for the methylation of DNA, neurotransmitters (serotonin, dopamine), and, crucially, the phospholipids that form the myelin sheath.
When B12 is absent due to microbial theft, the "Folate Trap" occurs. Methyltetrahydrofolate (the active form of folate) becomes "trapped" because it cannot pass its methyl group to B12. This leads to a functional folate deficiency even if folate levels in the blood appear high. The result is a failure in DNA synthesis, specifically affecting rapidly dividing cells like those in the bone marrow (leading eventually to megaloblastic anaemia) and the epithelial lining of the gut.
The Methylmalonyl-CoA Mutase Pathway and Myelin Decay
The second enzyme, methylmalonyl-CoA mutase, resides in the mitochondria. It requires adenosylcobalamin to convert methylmalonyl-CoA into succinyl-CoA, a vital component of the Krebs cycle (energy production). When this pathway is blocked by B12 deficiency, Methylmalonic Acid (MMA) builds up in the blood and tissues.
High levels of MMA are not merely a marker of deficiency; they are actively neurotoxic. MMA interferes with the synthesis of fatty acids required for the maintenance of the myelin sheath—the protective insulation around our nerves. As the myelin degrades (demyelination), nerve signals become "leaky" and slow down. This is the physiological origin of the "tingling" (paresthesia) and numbness associated with B12 malabsorption. It is a literal short-circuiting of the human electrical system.
Oxidative Stress and Neuronal Apoptosis
The disruption of these two pathways leads to a massive surge in oxidative stress within the nervous system. Without SAMe, the production of glutathione—the master antioxidant—is severely hampered. Neurons, which are particularly sensitive to oxidative damage, begin to undergo apoptosis (programmed cell death). This damage is most profound in the dorsal and lateral columns of the spinal cord, leading to a clinical condition known as Subacute Combined Degeneration. If the microbial theft is not addressed, this neurological damage can transition from reversible dysfunction to permanent physical disability.
##
Environmental Threats and Biological Disruptors
The rise in B12 malabsorption is not a random evolutionary quirk; it is a direct consequence of the modern environmental and pharmacological landscape. Several "biological disruptors" have paved the way for microbial theft by weakening the host’s defences and fostering an environment conducive to bacterial overgrowth.
The PPI Epidemic
In the UK, Proton Pump Inhibitors like Omeprazole and Lansoprazole are among the most frequently prescribed medications. While they offer short-term relief for acid reflux, their long-term use is a primary driver of B12 deficiency. By suppressing stomach acid, these drugs fail to liberate B12 from food and, more importantly, they remove the "acid barrier" that prevents colonic bacteria from migrating into the small intestine. This creates a "welcome mat" for SIBO.
ALARMING FACT: Long-term use of PPIs (more than 2 years) has been clinically shown to increase the risk of B12 deficiency by 65%. In the UK, many patients remain on these drugs for decades without routine B12 monitoring.
Glyphosate and the Microbiome
The herbicide glyphosate, pervasive in the modern food supply, acts as a potent antimicrobial. However, it does not kill all bacteria equally. It selectively targets beneficial species (like *Lactobacillus* and *Bifidobacterium*) while allowing pathogenic, B12-consuming strains like *Salmonella* and *Clostridia* to flourish. This shift in the microbial landscape—the "dysbiosis"—is the foundational precursor to microbial theft.
Heavy Metals and Thiol-Binding
Mercury, lead, and aluminium have a high affinity for "thiol" groups in enzymes. These metals can interfere with the transport proteins (Transcobalamin) and the intracellular enzymes that utilise B12. A body burdened by heavy metals may have B12 in the blood, but the cells cannot "unlock" it. Furthermore, heavy metals disrupt the Migrating Motor Complex (MMC)—the "housekeeping wave" of the small intestine—leading to the stagnation of food and subsequent bacterial overgrowth.
Alcohol and Acetaldehyde
Alcohol consumption is a significant disruptor of B12 metabolism in the UK. Acetaldehyde, the primary metabolite of alcohol, can destroy B12 in the bloodstream and inhibit the ileal receptors. For the regular drinker, the "theft" is two-fold: bacteria consume the B12 in the gut, and alcohol prevents what little is left from being utilised by the brain.
##
The Cascade: From Exposure to Disease
The progression from initial microbial overgrowth to full-blown neurological disease is often slow, subtle, and deceptive. It follows a predictable "Cascade of Decay" that is frequently ignored by clinicians until the damage is severe.
Stage 1: The Digestive Prelude
It begins with subtle gastrointestinal distress—bloating, flatulence, or a change in bowel habits. These are the first signs of SIBO. At this stage, the bacteria are beginning to colonise the upper reaches of the small intestine. The host may feel "heavy" after meals, as the bacteria ferment carbohydrates and शुरू to sequester cobalamin.
Stage 2: The Metabolic Dip
As B12 levels begin to drop, the first symptom is typically unexplained fatigue. This isn't just "tiredness"; it is a profound, cellular lethargy. The brain feels "foggy," and word-finding becomes difficult. This corresponds to the initial slowing of the methylation cycle and a slight rise in homocysteine.
Stage 3: The Neurological "Warning Shots"
This is the stage mentioned in our brief: tingling in the extremities. Known as peripheral neuropathy, it usually starts in the toes and fingers. Patients often describe a feeling of "pins and needles" or a sensation like "walking on cotton wool." These are the warning shots of demyelination. Crucially, at this stage, the patient's Full Blood Count (FBC) will almost always be normal. There is no anaemia yet, because the body prioritises red blood cell production over nerve maintenance.
Stage 4: Subacute Combined Degeneration
If the theft continues, the damage moves to the spinal cord. Coordination becomes impaired (ataxia). The patient may start to stumble or lose their balance in the dark. Reflexes are altered. Psychiatric symptoms may also emerge, including depression, irritability, and in severe cases, "megaloblastic madness" (hallucinations and paranoia).
Stage 5: Haematological Failure
Only in the final stages does the bone marrow fail, leading to Macrocytic (large cell) Anaemia. This is where mainstream medicine usually steps in, but for many, it is too late to reverse the neurological "Stage 3 and 4" damage. The obsession with anaemia as a diagnostic requirement is a fatal flaw in modern diagnostics.
##
What the Mainstream Narrative Omits
The current medical approach to B12 deficiency is dangerously reductionist. By focusing solely on dietary intake and autoimmune Pernicious Anaemia, the "theft" by the microbiome is completely overlooked. There are three critical omissions in the mainstream narrative that are costing patients their health.
1. The Fallacy of the "Normal" Range
In the UK, the "normal" range for serum B12 is often cited as 200–900 pg/mL. However, research indicates that neurological symptoms can occur in individuals with levels as high as 400 or 500 pg/mL. The "normal" range is a statistical average of a largely unhealthy population, not an indicator of optimal neurological function. Furthermore, serum testing measures B12 bound to *both* Transcobalamin II (active) and Haptocorrin (inactive). A patient can have a "normal" total B12 while being functionally deficient in active B12.
2. The Focus on Anaemia over Neuropathy
Doctors are trained to look for "Mean Corpuscular Volume" (MCV) on a blood test. If the red blood cells aren't enlarged, they often rule out B12 deficiency. This is a scientific error. Neurological symptoms precede haematological changes in up to 30% of cases. By waiting for anaemia to appear, the clinician is waiting for the house to burn down before checking the smoke alarm.
3. The Failure to Address the "Sink"
Mainstream treatment involves B12 injections or high-dose pills. While necessary, these treatments often fail because they do not address the sink—the bacterial overgrowth that is stealing the B12. If a patient has SIBO, giving oral B12 is like pouring water into a bucket with a hole in the bottom. You might get some into the bloodstream via passive diffusion (about 1% of the dose), but the bacteria will thrive on the rest, ensuring the problem persists. True recovery requires the eradication of the microbial thieves.
##
The UK Context
The United Kingdom presents a unique and challenging environment for B12 health. The confluence of NHS budgetary constraints, dietary trends, and a specific pharmacological culture has created a "perfect storm" for malabsorption issues.
The NHS Guidelines Bottleneck
The current NICE (National Institute for Health and Care Excellence) guidelines for B12 deficiency are often criticised by specialists for being too conservative. The reliance on the serum B12 test as a primary gatekeeper prevents many symptomatic patients from receiving the injections they need. In many regions, there is a "postcode lottery" regarding how frequently a patient can receive B12 hydroxycobalamin injections, with some surgeries strictly adhering to a 3-month schedule that is insufficient for those with severe malabsorption or neurological symptoms.
The Rise of Plant-Based Diets
The UK has seen a massive surge in veganism and plant-based eating. While often motivated by ethics or heart health, this shift removes the primary dietary sources of B12 (meat, eggs, dairy). When a plant-based diet is layered on top of an undiagnosed SIBO condition, the "theft" becomes total. The body has no incoming B12 and a microbiome that is actively depleting its internal stores.
UK FACT: The prevalence of B12 deficiency among UK vegans who do not supplement is estimated to be over 50%. However, even those who supplement may remain deficient if they suffer from the "Microbial Theft" of SIBO.
Socioeconomic Factors and "The Tea and Toast Diet"
In many older UK populations, socioeconomic factors lead to what is colloquially known as the "Tea and Toast" diet. This high-carbohydrate, low-protein intake provides the perfect substrate (glucose and starch) for SIBO-related bacteria to thrive, while offering zero B12. This demographic is also the most likely to be prescribed PPIs for "indigestion," creating a vicious cycle of malabsorption and bacterial proliferation.
##
Protective Measures and Recovery Protocols
Recovering from microbial theft requires a two-pronged strategy: replenishing the host and evicting the thief. A simple multi-vitamin will not suffice. The protocol must be clinical, targeted, and persistent.
Step 1: Bypassing the Gut
In cases of established SIBO or ileal damage, oral B12 is often ineffective. To saturate the nervous system and bypass the microbial thieves, B12 injections (Hydroxycobalamin) are the gold standard. In the UK, if your GP refuses frequent injections, sublingual methylcobalamin sprays or "liposomal" B12 preparations can offer a secondary route, as they are absorbed through the mucosal membranes of the mouth, bypassing the small intestine entirely.
Step 2: Eradicating the Thieves (SIBO Protocol)
One must address the overgrowth. This involves:
- —The Low-FODMAP Diet: Temporarily starving the bacteria by removing the fermentable carbohydrates they thrive on.
- —Herbal Antimicrobials: Using substances like Berberine, Oregano Oil, and Allicin (from garlic) to reduce the bacterial load in the small intestine.
- —Prokinetics: Supporting the Migrating Motor Complex (MMC) to ensure that bacteria are "swept" out of the small intestine and into the colon where they belong. Ginger and 5-HTP are natural options used to support gut motility.
Step 3: Restoring the Gastric Barrier
To prevent a recurrence of the theft, the stomach's natural defences must be restored. This involves weaning off PPIs (under medical supervision) and potentially supplementing with Betaine HCl and pepsin to ensure an acidic environment that kills incoming bacteria and releases B12 from food.
Step 4: Supporting the Methylation Cycle
B12 does not work in isolation. Recovery requires "cofactors." These include:
- —Folate (as Methylfolate): To break the "Folate Trap."
- —B6 (as P5P): For neurotransmitter synthesis.
- —Magnesium: To support the energy-intensive process of nerve repair.
- —Potassium: Starting B12 therapy can cause a temporary drop in potassium as the body begins producing new red blood cells; thus, potassium-rich foods (bananas, avocados) are essential during the early stages of recovery.
Step 5: Choosing the Right Form
Not all B12 is created equal. Cyanocobalamin, the most common synthetic form, requires the body to strip off a cyanide molecule—a process that is inefficient in a stressed or toxic system. Methylcobalamin and Adenosylcobalamin are "bio-identical" forms that the body can use immediately. For neurological recovery, a combination of these two "active" forms is superior.
##
Summary: Key Takeaways
The phenomenon of B12 malabsorption via microbial theft is a cornerstone of modern chronic illness. To ignore the gut's microbial state while attempting to treat neurological symptoms is a futile endeavour.
- —The Small Intestine is the Battlefield: SIBO is not just a cause of bloating; it is a primary driver of nutrient sequestration. Bacteria possess the machinery to steal B12 before it reaches the human absorption site in the ileum.
- —Neuropathy is the Early Warning: Tingling, numbness, and brain fog are not "normal signs of aging." They are clinical indicators of myelin decay and should be treated as a neurological emergency, regardless of whether anaemia is present.
- —Testing is Flawed: A "normal" serum B12 result does not rule out deficiency. Clinicians must look at Methylmalonic Acid (MMA) and Homocysteine for a true picture of cellular health.
- —The UK Context is Critical: The widespread use of PPIs and the rigidity of NHS B12 protocols have left millions vulnerable to permanent nerve damage.
- —Recovery Requires a Dual Approach: You cannot simply supplement your way out of a SIBO-driven deficiency. You must eradicate the bacterial overgrowth while bypassing the gut with injections or sublinguals to provide the brain with the "raw materials" it needs to heal.
The "Microbial Theft" of B12 is a testament to the complexity of our internal ecosystem. We are not a closed system; we are a walking biome. When we lose control of that biome, our very nerves pay the price. It is time to reclaim our biological resources from the thieves within.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "B12 Malabsorption: The Neurological Consequences of Microbial Theft"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper