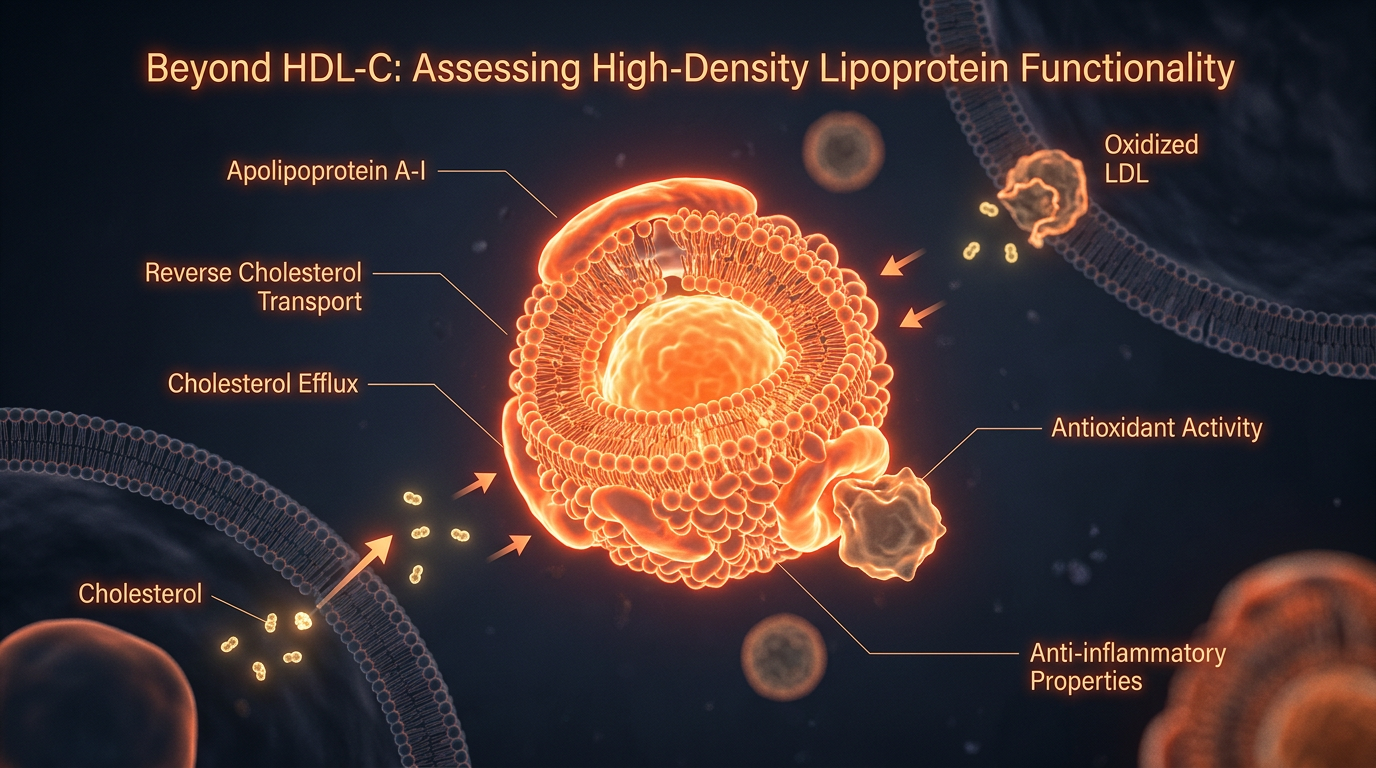
Beyond HDL-C: Assessing High-Density Lipoprotein Functionality
Shifting the focus from simple HDL cholesterol levels to the cholesterol efflux capacity and anti-inflammatory properties of HDL particles.
# Beyond HDL-C: Assessing High-Density Lipoprotein Functionality
For decades, the clinical narrative surrounding cardiovascular health has been tethered to a simplistic, binary ledger: Low-Density Lipoprotein (LDL) is ‘bad’, and High-Density Lipoprotein (HDL) is ‘good’. This reductionist paradigm, whilst convenient for pharmaceutical marketing and rapid primary care consultations, is increasingly viewed by the vanguard of lipidology as an obsolete oversimplification.
The 'Good Cholesterol' moniker is not merely imprecise; it is potentially dangerous. Recent large-scale Mendelian randomisation studies and failed pharmacological trials have exposed a haunting reality: increasing the *concentration* of HDL cholesterol (HDL-C) does not inherently confer cardioprotection. We are entering an era of ‘Innerstanding’ where we must distinguish between the passenger (cholesterol) and the vehicle (the HDL particle). To truly assess cardiovascular risk, we must look beyond the static measurement of HDL-C and scrutinise the dynamic, proteomic complexity of HDL *functionality*.
The Biological Mechanism: More Than a Scavenger

Magnesium Blend – The Most Important Mineral
A high-bioavailability mineral blend designed to support over 300 essential biochemical reactions, from energy production to muscle relaxation. This formula helps combat daily fatigue while providing the foundational support your nervous system and bones require.
Vetting Notes
Pending
To understand why a standard lipid panel is insufficient, one must first comprehend the multifaceted biological roles of High-Density Lipoproteins. HDL is not a single entity but a highly heterogeneous population of particles, varying in size, density, and molecular cargo.
Reverse Cholesterol Transport (RCT)
The primary mechanism traditionally attributed to HDL is Reverse Cholesterol Transport. This is the process by which HDL removes excess cholesterol from peripheral tissues—most crucially, from macrophages within the arterial wall—and transports it back to the liver for excretion in bile.
- —Efflux: The process begins via the ATP-binding cassette transporters (ABCA1 and ABCG1). HDL particles act as ‘sinks’, drawing cholesterol out of the cells.
- —Esterification: Once inside the HDL particle, the enzyme Lecithin-Cholesterol Acyltransferase (LCAT) converts free cholesterol into cholesterol esters, sequestering them in the particle's core.
- —Hepatic Delivery: The particle then delivers its payload to the liver via the Scavenger Receptor Class B Type 1 (SR-BI).
However, the rate of this flux—the Cholesterol Efflux Capacity (CEC)—is a far more potent predictor of cardiovascular events than the total amount of cholesterol carried by the particles at any given moment.
The Proteomic Shield: PON1 and Beyond
HDL is a mobile platform for over 80 different proteins and hundreds of lipid species. One of the most critical is Paraoxonase 1 (PON1). This enzyme is physically tethered to functional HDL and serves as a primary antioxidant defence. It actively prevents the oxidation of LDL particles; it is the *oxidised* LDL, not native LDL, that initiates the formation of atherosclerotic plaques.
Furthermore, functional HDL exhibits:
- —Anti-inflammatory properties: Inhibiting the expression of adhesion molecules on the vascular endothelium.
- —Antithrombotic effects: Regulating platelet aggregation and promoting fibrinolysis.
- —Vasodilatory capacity: Stimulating the production of nitric oxide (NO), ensuring arterial flexibility.
The HDL Paradox: When 'High' is Not 'Healthy'
The medical establishment has long operated under the assumption that 'higher is better' regarding HDL-C. However, epidemiological data now reveals a U-shaped curve.
According to data analysed from UK Biobank cohorts, individuals with extremely high HDL-C levels (above 2.3 mmol/L in women and 2.0 mmol/L in men) actually show an *increased* risk of all-cause mortality and cardiovascular events.
This is known as the HDL Paradox. In these cases, the HDL particles are often 'clogged' or 'dysfunctional'. They have lost their ability to promote efflux and have instead become pro-inflammatory. In states of chronic inflammation, such as metabolic syndrome or untreated autoimmune conditions, HDL can undergo a 'proteomic shift'. It loses its protective proteins (like PON1) and gains inflammatory ones (like Serum Amyloid A). This transforms the 'good' cholesterol into a 'pathogenic' particle that actually accelerates vascular damage.
Environmental Disruptors: The Modern Assault on Lipid Integrity
The decline in HDL functionality across the British population is not merely a genetic quirk; it is an environmental consequence. We are living in a 'lipid-toxic' environment that actively degrades the quality of our lipoproteins.
Glycation and Ultra-Processed Foods (UPFs)
In the UK, over 50% of the average diet now consists of ultra-processed foods. These are typically high in refined sugars and seed oils. High systemic glucose levels lead to the non-enzymatic glycation of HDL.
- —Glycated HDL has a significantly reduced affinity for the ABCA1 transporter, meaning it can no longer effectively clear cholesterol from the arteries.
- —Lipid Peroxidation: The consumption of industrially processed vegetable oils, rich in linoleic acid, increases the susceptibility of the HDL lipidome to oxidation, rendering the particles dysfunctional before they even reach the bloodstream.
Endocrine Disruptors and Microplastics
Emerging research suggests that environmental toxins play a hidden role in lipid dysfunction. Bisphenol A (BPA) and certain phthalates, common in food packaging, have been shown to interfere with the nuclear receptors (such as PPARs and LXRs) that regulate HDL synthesis.
- —Microplastics: Recent studies have identified microplastic polymers within human carotid plaques. These foreign bodies induce local oxidative stress that overwhelms the antioxidant capacity of HDL, effectively 'burning out' the protective enzymes like PON1.
The Impact of Chronic Circadian Disruption
The British workforce is increasingly subject to irregular sleep patterns and blue-light exposure. HDL metabolism is governed by circadian rhythms. The expression of LCAT and the activity of hepatic receptors peak during specific windows. Chronic disruption of the biological clock leads to the production of 'immature' HDL particles that lack the necessary protein cargo to perform their protective duties.
The Diagnostic Gap: Why Your GP is Missing the Point
The standard NHS lipid profile—measuring Total Cholesterol, LDL-C, HDL-C, and Triglycerides—is a relic of 1970s technology. It measures *mass*, not *activity*.
To achieve true 'Innerstanding' of one's cardiovascular health, more advanced metrics are required:
- —HDL Particle Number (HDL-P): Measured via Nuclear Magnetic Resonance (NMR) spectroscopy. A high number of small, dense HDL particles is often more protective than a few large, cholesterol-heavy ones.
- —Apolipoprotein A1 (ApoA-I): The primary structural protein of HDL. This is a better marker of the total number of functional units than the cholesterol measurement itself.
- —Myeloperoxidase (MPO) Levels: High levels of this enzyme indicate that HDL is being oxidised and rendered dysfunctional.
Recovery Protocols: Restoring Proteomic Integrity
Restoring HDL functionality is not achieved through the 'magic bullet' of statins—which primarily lower LDL and have a negligible, sometimes negative, effect on HDL quality. Instead, recovery requires a multi-faceted approach aimed at metabolic flexibility and the reduction of oxidative stress.
Nutritional Interventions
- —Polyphenol Loading: High-quality Extra Virgin Olive Oil (EVOO) is perhaps the most potent tool for enhancing HDL function. The polyphenol *oleuropein* has been shown to increase PON1 activity and improve cholesterol efflux.
- —Anthocyanins: Found in dark berries (blackberries, blackcurrants), these compounds have been shown in clinical trials to increase ApoA-I levels and enhance the antioxidant capacity of HDL.
- —Omega-3 Fatty Acids (EPA/DHA): Crucial for maintaining the fluidity of the HDL membrane. Ensure these are sourced from 'cold-pressed' or 'molecularly distilled' sources to avoid pre-existing oxidation.
- —Elimination of Trans-Fats and UPFs: This is non-negotiable. Reducing the glycation burden is the first step in allowing the liver to produce 'clean' HDL particles.
Lifestyle and Hormesis
- —High-Intensity Interval Training (HIIT): While moderate aerobic exercise is beneficial for HDL-C levels, HIIT has been shown to specifically improve the *efflux capacity* of HDL particles.
- —Cold Exposure: Short bursts of cold thermogenesis (e.g., cold showers or plunges) can activate brown adipose tissue, which has a synergistic effect on lipid metabolism and the clearance of dysfunctional lipoproteins.
- —Circadian Realignment: Prioritising a consistent sleep-wake cycle and reducing evening blue light exposure supports the natural nocturnal peak of RCT processes.
Targeted Supplementation (The Advanced Tier)
- —Niacin (Vitamin B3): Although fallen out of favour in mainstream medicine due to the 'flushing' side effect, pharmaceutical-grade Niacin remains one of the most effective ways to increase HDL-P and ApoA-I. It must, however, be used under expert guidance to monitor insulin sensitivity.
- —Coenzyme Q10 (Ubiquinol): A vital lipid-soluble antioxidant that protects the HDL particle itself from being oxidised while in circulation.
Summary: The New Paradigm of Lipid Science
The transition from assessing HDL-C to assessing HDL *functionality* represents a seismic shift in preventative medicine. We must move away from the 'bean-counting' approach to cholesterol and towards a deeper understanding of the molecular integrity of our lipoproteins.
Statistical reality in the UK: Despite 40% of the adult population being on lipid-lowering medication, cardiovascular disease remains the leading cause of death. This suggests we are measuring the wrong things and, consequently, treating the wrong targets.
To achieve longevity, one must ensure their HDL is not just 'present' but 'potent'. It must be an active, enzyme-rich, un-glycated, and resilient fleet of particles capable of patrolling the endothelium and maintaining cellular lipid homeostasis. True health is found not in the quantity of cholesterol we carry, but in the functional elegance of the systems that manage it.
The era of 'Good' versus 'Bad' is over. The era of HDL Functionality has begun. It is time to look beneath the surface of the standard blood test and master the inner workings of our own biology.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Beyond HDL-C: Assessing High-Density Lipoprotein Functionality"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Cholesterol & Lipid Science — products curated by our research team for educational relevance and biological support.

Magnesium L-Threonate
Magnesium Blend – The Most Important Mineral

Energy Blend Supports
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper