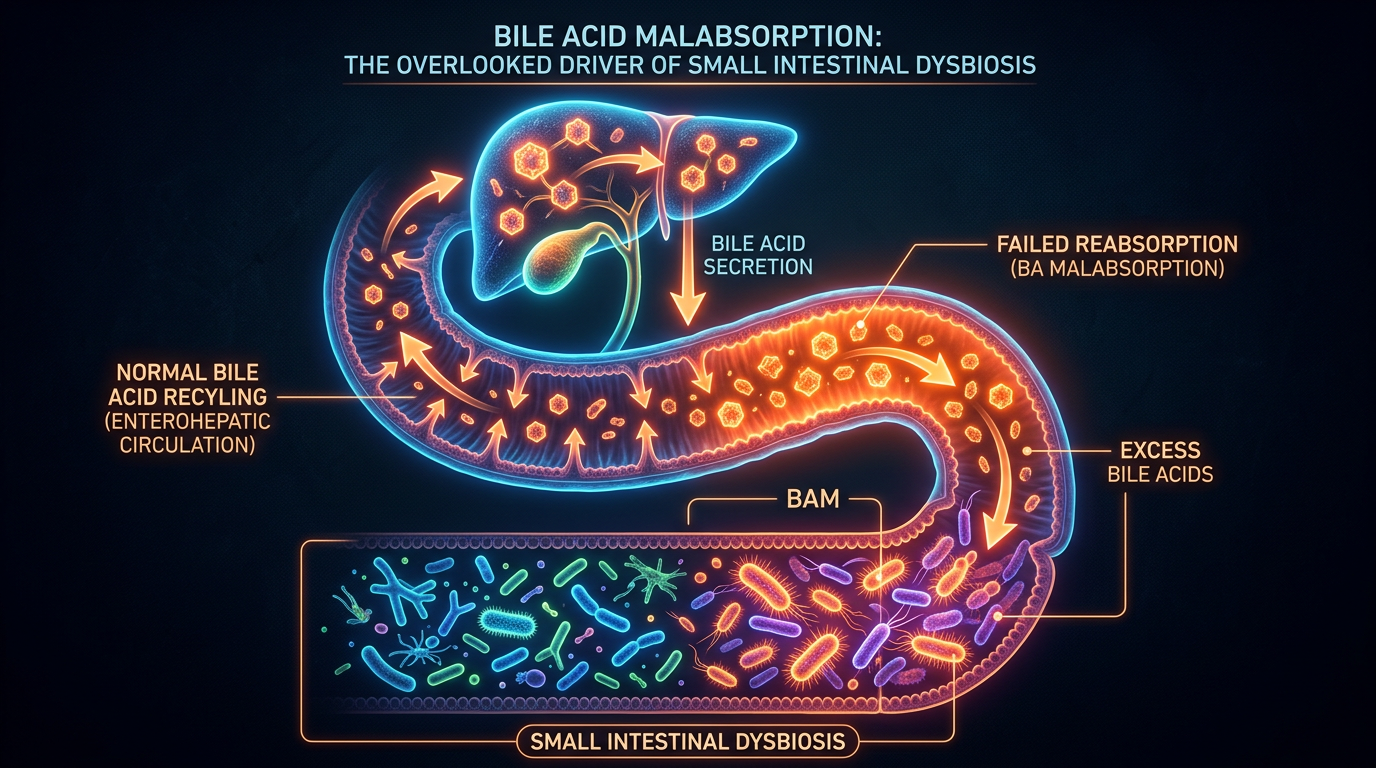
Bile Acid Malabsorption: The Overlooked Driver of Small Intestinal Dysbiosis
Bile is not just a digestive fluid but a potent antimicrobial agent that keeps the small intestine sterile. Deficiencies in bile flow or quality allow for the rapid proliferation of gram-negative bacteria.
Overview
In the contemporary landscape of gastroenterology, the surge of Small Intestinal Bacterial Overgrowth (SIBO) has been met with a flurry of restrictive diets and cyclical antibiotic protocols. Yet, despite these interventions, recurrence rates remain staggeringly high. At INNERSTANDING, we posit that the medical establishment is looking at the smoke rather than the fire. The true culprit behind the persistent colonisation of the small intestine by opportunistic gram-negative bacteria is not merely a failure of motility or a surplus of dietary carbohydrates, but a profound breakdown in the body's primary sterilisation system: Bile Acid Homeostasis.
Bile is frequently dismissed as a simple digestive "soap" tasked with the emulsification of dietary fats. This reductionist view ignores one of the most critical biological imperatives of the human body. Bile acids are, in fact, potent endocrine signalling molecules and broad-spectrum antimicrobial agents. They serve as the "biological detergent" that maintains the relative sterility of the small intestine, a transit corridor that—unlike the colon—is not designed to house trillions of fermenting microbes. When the quality, quantity, or recycling of these bile acids is compromised, the small intestine loses its chemical shield.
The condition known as Bile Acid Malabsorption (BAM)—also referred to as Bile Acid Diarrhoea (BAD)—is the clinical manifestation of this systemic failure. However, the term "malabsorption" is somewhat of a misnomer in the context of dysbiosis. It represents a rupture in the enterohepatic circulation, where bile acids that should be recycled in the terminal ileum are instead dumped into the colon, while the proximal small intestine is left vulnerable to microbial invasion. This article serves as an exhaustive investigation into the mechanisms by which bile acid deficiency facilitates small intestinal dysbiosis, the environmental factors degrading our hepatic health, and the necessary protocols to restore the integrity of the gut’s chemical gatekeeper.
Estimates suggest that up to 30% of patients diagnosed with Irritable Bowel Syndrome with Diarrhoea (IBS-D) in the United Kingdom are actually suffering from undiagnosed Bile Acid Malabsorption, yet access to the definitive SeHCAT diagnostic scan remains restricted in many NHS trusts.
The Biology — How It Works
To understand why bile is the master regulator of small intestinal health, one must first appreciate the complexity of the enterohepatic circulation. The liver synthesises primary bile acids—specifically cholic acid (CA) and chenodeoxycholic acid (CDCA)—from cholesterol. These are conjugated with the amino acids glycine or taurine to increase their solubility and then stored in the gallbladder. Upon the ingestion of fats, the hormone cholecystokinin (CCK) triggers the contraction of the gallbladder, releasing a concentrated surge of bile into the duodenum.
While the primary role of this surge is the formation of micelles to facilitate the absorption of fat-soluble vitamins (A, D, E, and K), the secondary role is defensive. Bile acids possess a detergent-like property that is inherently toxic to many bacterial species. They are capable of disrupting the phospholipid bilayers of bacterial cell membranes, leading to lysis and death of the invading organisms. Furthermore, bile acids act as ligands for the Farnesoid X Receptor (FXR), a nuclear receptor that resides in the wall of the small intestine. When bile acids bind to FXR, they trigger the synthesis of Antimicrobial Peptides (AMPs)—the body’s endogenous antibiotics—such as angiogenin 1 and alpha-defensins.
The system is designed for extreme efficiency. Under normal physiological conditions, approximately 95% of the bile acids secreted into the duodenum are reabsorbed in the terminal ileum and returned to the liver via the portal vein. This cycle occurs 4 to 12 times a day. If this reabsorption is impaired, the liver cannot keep up with the demand for "de novo" synthesis. The result is a depleted bile acid pool. This depletion creates a "low-tide" environment in the small intestine, where the lack of surfactant pressure allows bacteria from the colon to migrate upstream or allows bacteria introduced through food to take up residence in the jejunum and ileum.
Furthermore, bile is the primary driver of the Migrating Motor Complex (MMC), the "inter-digestive housekeeper" wave that sweeps food debris and bacteria toward the colon during periods of fasting. Without adequate bile flow, the MMC becomes sluggish, turning the small intestine from a flowing river into a stagnant pond. In a stagnant pond, life—specifically pathogenic life—flourishes.
Mechanisms at the Cellular Level
At the microscopic scale, the relationship between bile acids and microbial suppression is orchestrated through a sophisticated feedback loop involving nuclear receptors and protein synthesis. The most critical player is the aforementioned Farnesoid X Receptor (FXR). When bile acids enter the enterocytes (intestinal cells), they activate FXR, which then stimulates the transcription of genes that produce FGF19 (Fibroblast Growth Factor 19).
FGF19 is a hormone that travels through the blood back to the liver, where it signals the downregulation of bile acid synthesis to prevent toxicity. However, within the gut itself, FXR activation is responsible for maintaining the "tight junctions" of the intestinal barrier. This is the first line of defence against Leaky Gut Syndrome. When bile acid flow is insufficient, FXR remains inactive, leading to a weakening of these junctions and allowing Lipopolysaccharides (LPS)—endotoxins found in the cell walls of gram-negative bacteria—to enter the systemic circulation.
The antimicrobial action of bile is not just about membrane disruption. Bile acids also induce DNA damage and protein misfolding within bacteria, specifically targeting those that do not possess "bile salt hydrolase" (BSH) enzymes. Unfortunately, many pathogenic gram-negative species, such as *Escherichia coli* and *Klebsiella*, have evolved mechanisms to resist low levels of bile, but they cannot withstand high, concentrated surges. When the bile pool is diluted or the gallbladder is sluggish (biliary dyskinesia), these pathogens gain a competitive advantage over beneficial species.
Research indicates that bile acids are capable of down-regulating the expression of genes involved in bacterial chemotaxis and flagellar synthesis. Effectively, healthy bile levels "paralyse" bacteria, preventing them from swimming upstream and colonising the upper reaches of the digestive tract.
Another cellular mechanism involves the TGR5 receptor. This is a membrane-bound G protein-coupled receptor that responds to bile acids by stimulating the release of Glucagon-like peptide-1 (GLP-1). GLP-1 is famous for its role in blood sugar regulation, but it also has profound anti-inflammatory effects on the gut lining. A deficiency in bile acid signalling at the TGR5 receptor level thus links SIBO and BAM directly to metabolic dysfunction, insulin resistance, and systemic inflammation.
Environmental Threats and Biological Disruptors
The modern world is fundamentally "anti-bile." The precipitous rise in SIBO and BAM over the last four decades correlates almost perfectly with the introduction of specific environmental toxins and dietary shifts that sabotage hepatic function.
1. The Glyphosate Factor
The most ubiquitous herbicide on the planet, glyphosate, is a primary disruptor of the Cytochrome P450 (CYP) enzymes in the liver. These enzymes are essential for the conversion of cholesterol into bile acids. By inhibiting the CYP7A1 enzyme—the rate-limiting step in bile synthesis—glyphosate ensures that the bile produced is chemically "thin" and insufficient in volume. Furthermore, glyphosate acts as a potent mineral chelator, stripping the body of the manganese and glycine required for bile conjugation.
2. The PPI Epidemic
Proton Pump Inhibitors (PPIs), widely prescribed in the UK for acid reflux, are a direct driver of bile-related dysbiosis. Bile requires a specific pH environment to function optimally. By suppressing stomach acid, PPIs alter the pH of the duodenum. This not only impairs the activation of digestive enzymes but also prevents the signal for the gallbladder to contract. The gallbladder becomes a reservoir for "biliary sludge"—thickened, stagnant bile that cannot effectively sterilise the small intestine.
3. Emulsifiers and Ultra-Processed Foods
The modern British diet is saturated with synthetic emulsifiers (such as carboxymethylcellulose and polysorbate 80). These compounds act like "fake bile," but without the antimicrobial properties. They break down the protective mucus layer of the gut, allowing bacteria to come into direct contact with the epithelial cells. This creates a state of chronic low-grade inflammation that further impairs the transport proteins responsible for recycling bile acids in the ileum.
4. Chronic Stress and the Vagus Nerve
The release of bile is a "rest and digest" function mediated by the vagus nerve. In a state of chronic sympathetic dominance (the "fight or flight" response), vagal tone is suppressed. This leads to a failure of the gallbladder to contract fully, even in the presence of fats. The result is a functional bile deficiency, even if the liver is technically capable of producing bile.
The Cascade: From Exposure to Disease
The progression from a compromised bile pool to systemic disease is a predictable biological cascade. It begins with Biliary Stasis. This is the stage where bile becomes viscous. This "sludge" often goes undetected on standard NHS ultrasounds, which are designed to look for hard gallstones rather than functional viscosity issues.
As bile flow slows, the sterilising pressure in the duodenum drops. Opportunistic bacteria from the colon, particularly those of the *Proteobacteria* phylum, begin to migrate through the ileocecal valve into the small intestine. This is the onset of SIBO. These bacteria begin to deconjugate bile acids prematurely. Instead of the bile acids staying in their glycine or taurine-bound state, the bacteria strip these amino acids off.
Deconjugated bile acids are highly irritating to the intestinal lining and are not easily reabsorbed. This leads to two disastrous outcomes:
- —Chemical Malabsorption: Because the bile acids are deconjugated too early, they lose their ability to form micelles. The patient begins to suffer from deficiencies in vitamins A, D, and K, leading to poor immunity and bone health.
- —Secretory Diarrhoea: The deconjugated bile acids reach the colon in high concentrations, where they act as an osmotic laxative, drawing water into the bowel and causing the classic "urgent" diarrhoea associated with BAM.
This is the point where the "Cascade of Endotoxemia" begins. The overgrowth of bacteria in the small intestine produces a constant stream of Lipopolysaccharides (LPS). Without sufficient bile to neutralise these endotoxins, they cross the weakened gut barrier and enter the portal vein. The liver is then forced to process these toxins, further distracting it from its task of producing high-quality bile. This creates a vicious cycle: poor bile leads to SIBO; SIBO leads to endotoxemia; endotoxemia leads to poor bile.
Systemic endotoxemia is now recognised as the primary driver of Non-Alcoholic Fatty Liver Disease (NAFLD), a condition that currently affects approximately 1 in 4 adults in the United Kingdom.
What the Mainstream Narrative Omits
The current medical approach to SIBO and BAM is characterised by a lack of "Innerstanding" regarding the interconnectedness of these systems. Standard treatment for SIBO usually involves Rifaximin, a non-absorbable antibiotic. While Rifaximin can temporarily reduce bacterial load, it does nothing to address the bile deficiency that allowed the bacteria to colonise in the first place. This is why SIBO recurrence rates are estimated to be as high as 60% within six months of antibiotic treatment.
Furthermore, the mainstream narrative fails to acknowledge the role of Thyroid Health in bile production. The conversion of the thyroid hormone T4 into its active form, T3, occurs largely in the liver and the gut. T3 is required to stimulate the "Cholesterol 7-alpha-hydroxylase" enzyme, which produces bile. Many patients in the UK are diagnosed with "subclinical hypothyroidism" and given no treatment, yet this marginal thyroid deficiency is enough to cripple bile production, leading to a lifetime of digestive distress.
There is also a significant omission regarding the Gallbladder’s role as a microbial filter. Most doctors tell patients that the gallbladder is an "extra organ" that can be removed without consequence. However, post-cholecystectomy patients (those who have had their gallbladder removed) are at a massive risk for SIBO. Without a gallbladder to provide the "surge" of bile needed to kill bacteria after a meal, they have a constant "drip" of weak bile that is insufficient for sterilisation.
Finally, the mainstream overlooks the microbiome of the bile duct itself. Recent research suggests that the biliary system has its own microbiome. When this is disrupted (biliary dysbiosis), it can lead to Primary Sclerosing Cholangitis (PSC) or other inflammatory conditions that are often misdiagnosed as simple IBS.
The UK Context
In the United Kingdom, the crisis of bile-related dysbiosis is exacerbated by a "wait and see" culture within the NHS. The SeHCAT (Selenium-homocholic acid taurine) test, which is the gold standard for diagnosing Bile Acid Malabsorption, is often only considered after years of "IBS" symptoms. In many regions, the test is simply not available, leading patients to be mismanaged with anti-motility drugs like Loperamide, which only further encourage bacterial stagnation.
The British diet, traditionally high in processed grains and low in the "bitter" compounds that stimulate bile flow, also plays a role. In continental Europe, the consumption of bitter aperitifs and digestive bitters is a cultural staple. In the UK, we have largely abandoned these medicinal foods. The result is a population with "lazy" livers and congested gallbladders.
According to data from the British Liver Trust, liver disease is the only major cause of death that is increasing in the UK, while it is decreasing in the rest of Europe. This is a direct reflection of our national failure to protect the enterohepatic cycle.
Moreover, the UK’s heavy reliance on glyphosate in industrial agriculture means that even those attempting to eat a "healthy" diet are often consuming significant levels of this bile-disrupting toxin through non-organic wheat and oats. The lack of stringent regulation on these herbicides in a post-Brexit landscape poses a significant threat to the long-term gut health of the nation.
Protective Measures and Recovery Protocols
Restoring the small intestinal environment requires a multi-pronged approach that goes beyond killing bacteria. We must restore the Chemical Shield.
1. Biliary Support and TUDCA
Tauroursodeoxycholic acid (TUDCA) is a hydrophilic bile acid that has been used for centuries in traditional medicine. Unlike the primary bile acids produced by the liver, TUDCA is extremely protective. It helps to thin the bile, making it more fluid and capable of reaching the deep recesses of the small intestine. TUDCA also acts as a "chaperone" molecule, preventing protein misfolding in the liver and protecting the gut lining from the corrosive effects of deconjugated bile acids.
2. The Power of Bitters
Stimulating the body’s own production of bile is essential. Bitter herbs such as Dandelion Root, Artichoke Leaf, and Gentian trigger the "bitter receptors" (T2Rs) on the tongue and in the gut. This sends a signal via the vagus nerve to the liver to increase bile synthesis and to the gallbladder to contract. Incorporating these bitters 15 minutes before a meal can significantly enhance the antimicrobial pressure in the small intestine.
3. Lecithin and Choline
Bile is not just bile acids; it is also composed of phospholipids, primarily Phosphatidylcholine. This molecule is what keeps bile in a liquid state. A deficiency in choline (common in the UK diet, which is often low in eggs and organ meats) leads to thick, stone-forming bile. Supplementing with Sunflower Lecithin or Alpha-GPC can improve the "solubility" of the bile pool.
4. Phase 2.5 Detoxification: The Transporters
The liver needs to export bile. This is sometimes called "Phase 3" or "Phase 2.5" detoxification. This requires the MRP2 and BSEP transport proteins. These proteins are inhibited by inflammation and oxidative stress. Anti-inflammatory compounds like Curcumin and Silymarin (Milk Thistle) can help maintain the integrity of these transporters, ensuring that bile doesn't "back up" into the liver cells.
5. Sequestration and Binding
For those already suffering from BAM, where bile acids are reaching the colon and causing diarrhoea, the use of Bile Acid Sequestrants (like Cholestyramine) is common. However, at INNERSTANDING, we prefer natural binders like Activated Charcoal or Micronised Zeolite taken away from meals. These can help bind deconjugated bile acids and bacterial LPS in the small intestine, preventing them from causing systemic damage while the liver is being repaired.
6. The MMC Pulse
To support the Migrating Motor Complex, one must practice intermittent fasting or "meal spacing." Constant grazing prevents the MMC from ever initiating. A minimum of 4 to 5 hours between meals allows the "bile-driven wave" to clear the small intestine. Furthermore, prokinetic agents such as Ginger and 5-HTP can assist in synchronising the MMC with bile release.
Summary: Key Takeaways
The path to resolving Small Intestinal Bacterial Overgrowth does not lie in more potent antibiotics or more restrictive diets. It lies in the restoration of the liver’s most potent defensive tool: Bile.
- —Bile is a Sterilant: It is the primary mechanism by which the small intestine remains free of colon-derived bacteria.
- —BAM is a Feedback Failure: Bile Acid Malabsorption is the result of a broken enterohepatic cycle, where the body fails to recycle its antimicrobial detergent.
- —The FXR Pathway is Key: Activating the Farnesoid X Receptor through healthy bile flow is essential for maintaining the gut barrier and producing endogenous antibiotics.
- —Environmental Toxins are the Root: Glyphosate, PPIs, and chronic stress are the primary drivers of the modern bile crisis.
- —The UK Context is Unique: High rates of liver disease and limited diagnostic access mean that patients must take an active role in their own hepatic recovery.
- —Recovery Requires Fluidity: Using TUDCA, bitters, and choline to "thin" the bile and restore the "surge" is the only way to prevent SIBO recurrence.
We must stop viewing the gut as a series of isolated pipes and start seeing it as a complex biochemical ecosystem. When the liver is supported and the bile is flowing, the small intestine can once again become the clean, efficient corridor of nutrient absorption it was designed to be. Truth in health begins with the liver. If you wish to understand the gut, you must first "innerstand" the bile.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Bile Acid Malabsorption: The Overlooked Driver of Small Intestinal Dysbiosis"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Glutathione Builder – Advanced Amino Acid Formula

MSM Sulphur – Nature’s Forgotten Mineral

Magnesium Blend – The Most Important Mineral
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper