Cardiac Regeneration: Healing the Broken Heart with Myocytes
Human hearts have limited regenerative capacity, but stem cell therapy aims to replace scarred tissue after a heart attack. Discover the challenges of integrating new myocytes into a beating heart.
Overview
The human heart is perhaps the most paradoxical organ in the biological repertoire. It is a marvel of endurance, a muscular pump designed to contract approximately 100,000 times a day, circulating roughly 7,600 litres of blood through 60,000 miles of vasculature. Yet, for all its mechanical prowess, the heart possesses an Achilles’ heel that has long baffled and frustrated the scientific community: a profound lack of regenerative capacity. While the liver can regrow from a mere fragment and the skin heals its lacerations with relative ease, the adult human heart is largely "post-mitotic." When a Myocardial Infarction (MI)—a heart attack—occurs, the loss of cardiomyocytes (heart muscle cells) is permanent. The body’s response is not to rebuild, but to patch. The result is a non-contractile, collagenous scar that weakens the organ’s structural integrity, leading down a one-way path toward Heart Failure (HF).
For decades, the medical establishment operated under the dogma that we are born with a fixed number of heart cells and that no new ones are formed during adulthood. We now know this is a half-truth. While there is a glacial turnover of myocytes—roughly 0.5% to 1% per year—this is nowhere near sufficient to repair the damage of a major cardiac event where billions of cells perish in hours.
The field of Cardiac Regeneration and Regenerative Medicine seeks to rewrite this biological script. By harnessing Stem Cell Science, researchers aim to replace the dead, fibrotic tissue with functional, beating Myocytes. However, the journey from laboratory petri dish to a beating human chest is fraught with biological hurdles, ethical dilemmas, and a pharmaceutical landscape that often prioritises chronic symptom management over definitive cures. This article explores the cutting edge of cardiac myocyte replacement, the hidden environmental factors sabotaging our natural repair mechanisms, and the "suppressed" biological truths that the mainstream narrative frequently overlooks.
According to the British Heart Foundation, there are approximately 7.6 million people living with heart and circulatory diseases in the UK, with heart failure reaching epidemic proportions as survival rates for acute attacks improve but long-term recovery stalls.
---
The Biology — How It Works
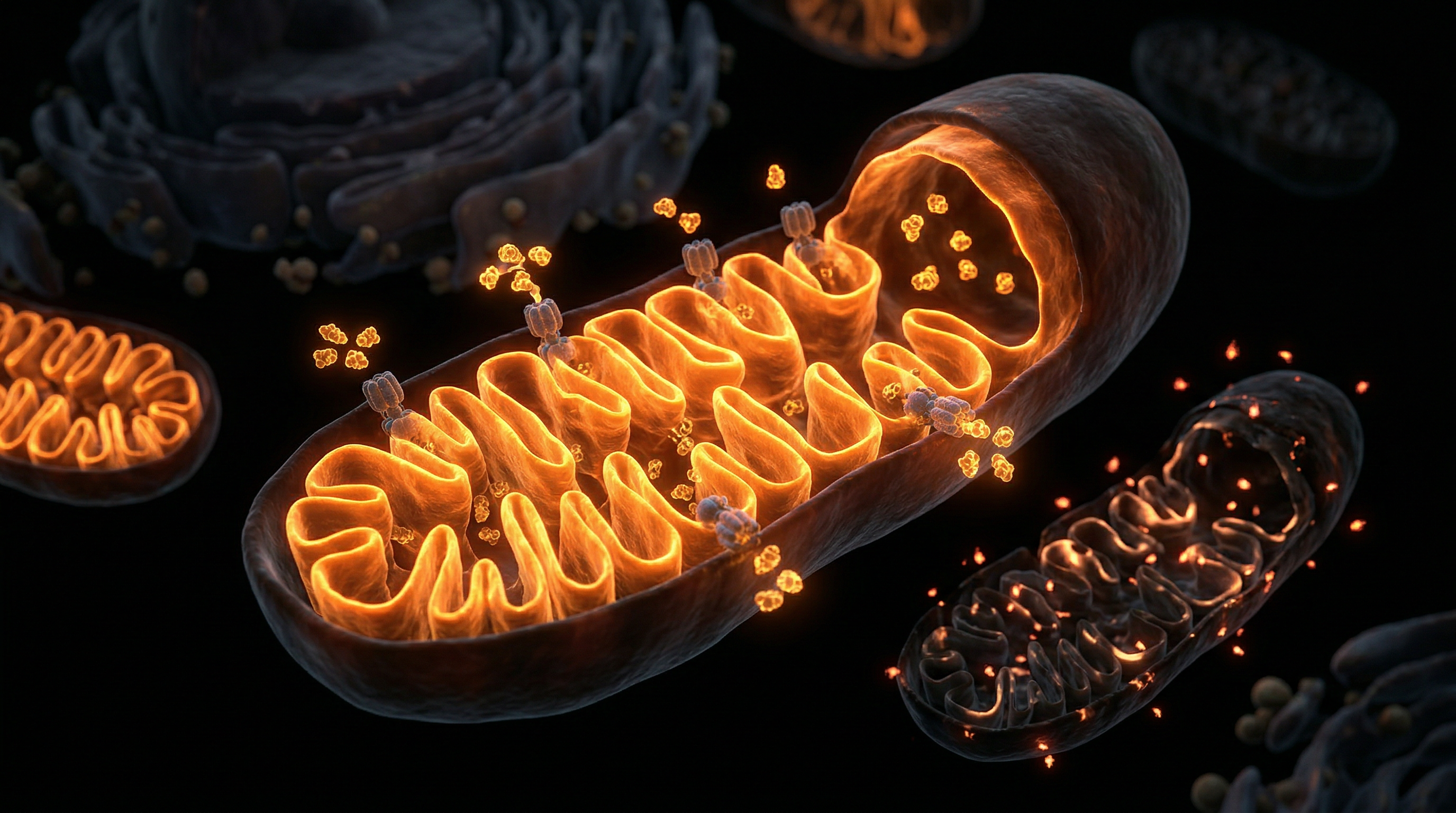
To understand how we might heal a "broken" heart, we must first understand the architecture of the Cardiomyocyte. These are the specialised muscle cells responsible for the contraction of the heart. Unlike skeletal muscle, which can rely on resident "satellite cells" for repair, the heart lacks a robust internal reservoir of progenitor cells.
The Problem of Terminal Differentiation
In the early stages of mammalian development, cardiomyocytes proliferate rapidly. However, shortly after birth, these cells undergo Terminal Differentiation. They exit the cell cycle, meaning they stop dividing. Instead of increasing in number (hyperplasia), the heart grows by increasing the size of existing cells (hypertrophy). This evolutionary trade-off was likely intended to ensure the stability of the heart’s electrical conduction system—after all, a constantly dividing tissue is a risk for arrhythmias and oncogenesis.
The Role of the Extracellular Matrix (ECM)
The heart is not just a collection of cells; it is a complex scaffold. The Extracellular Matrix provides the structural framework that holds myocytes in place. Following a heart attack, the ECM is degraded by enzymes called Matrix Metalloproteinases (MMPs) and replaced by dense, stiff collagen. This "scar" prevents the heart from rupturing in the short term, but it acts as a physical and electrical barrier to any potential regeneration.
Endogenous Regeneration vs. Exogenous Intervention
There are two primary schools of thought in cardiac regeneration:
- —Stimulating Endogenous Repair: Attempting to "unlock" the adult heart’s hidden ability to divide, perhaps by manipulating genetic pathways like the Hippo Signalling Pathway or using small molecules to force myocytes back into the cell cycle.
- —Exogenous Cell Therapy: Introducing new cells into the heart from an external source. This involves the use of Pluripotent Stem Cells, which can be coaxed into becoming functional heart muscle.
Statistics show that after a massive myocardial infarction, a patient may lose up to 1 billion cardiomyocytes—roughly 25% of the total number in the left ventricle—within a matter of hours.
---
Mechanisms at the Cellular Level
At the heart of the regenerative revolution are Stem Cells. These are undifferentiated cells with the unique ability to become any cell type in the body. In cardiac science, three main types dominate the discourse:
1. Induced Pluripotent Stem Cells (iPSCs)
Discovered by Shinya Yamanaka (for which he won the Nobel Prize), iPSCs are adult cells—usually skin or blood cells—that have been "reprogrammed" back into an embryonic-like state using specific transcription factors. These cells can then be directed to become Cardiomyocytes (iPSC-CMs). The beauty of this technology is that it allows for autologous transplantation—using a patient’s own cells to repair their own heart, theoretically eliminating the risk of immune rejection.
2. Mesenchymal Stem Cells (MSCs)
Derived from bone marrow, adipose tissue, or the umbilical cord, MSCs do not necessarily become new heart muscle themselves. Instead, they act as "biological factories." Through Paracrine Signalling, they secrete growth factors, anti-inflammatory cytokines, and Exosomes that encourage the surviving heart tissue to heal and prevent further cell death (apoptosis).
3. The Challenge of Electromechanical Coupling
The most significant hurdle in cardiac regeneration is not just creating the cells, but integrating them. A heart is a coordinated electrical circuit. For a new myocyte to contribute to the heart’s pumping action, it must form Gap Junctions (specifically using the protein Connexin-43) with the host cells. If the new cells beat at their own rhythm, independent of the rest of the heart, the result is Ventricular Arrhythmia—a potentially fatal complication.
- —Engraftment: The process of the new cells physically "taking root" in the scarred tissue.
- —Vascularisation: The new muscle requires a blood supply; without new capillaries (angiogenesis), the transplanted cells will die of oxygen starvation.
- —Maturation: Lab-grown myocytes often resemble foetal heart cells rather than adult ones. They are smaller, weaker, and use glucose for energy instead of the fatty acids used by adult hearts.
---
Environmental Threats and Biological Disruptors
While the laboratory progress is impressive, we must address why the modern human heart seems increasingly fragile. As a researcher for INNERSTANDING, I must highlight that cardiac health is being systematically undermined by environmental factors that mainstream cardiology often dismisses as secondary or irrelevant.
Endocrine Disrupting Chemicals (EDCs)
The modern world is saturated with Xenoestrogens and other EDCs like Bisphenol A (BPA) and Phthalates. These chemicals, found in plastics, receipts, and food linings, have been shown to interfere with calcium signalling in cardiomyocytes. Calcium is the "trigger" for every single heartbeat; when this signalling is disrupted, the heart’s ability to contract and eventually regenerate is severely compromised.
The Impact of Glyphosate
Glyphosate, the world’s most widely used herbicide, has been detected in the majority of Western food supplies. Emerging research suggests that glyphosate may disrupt the Mitochondrial function within the heart. Given that myocytes have the highest mitochondrial density of any cell type (to meet their massive energy demands), glyphosate-induced oxidative stress is a direct assault on the heart’s regenerative potential.
Electromagnetic Frequencies (EMFs)
The heart is an electrical organ. It produces the strongest electromagnetic field in the human body, detectable several feet away with sensitive equipment. The proliferation of high-frequency Non-Ionising Radiation (from 5G infrastructure and ubiquitous Wi-Fi) is increasingly linked to disruptions in voltage-gated calcium channels (VGCCs). This constant "noise" may prevent the delicate electromechanical coupling required for stem cell integration.
Heavy Metal Accumulation
Cadmium, Lead, and Mercury are potent cardiotoxins. They accumulate in the cardiac tissue over decades, replacing essential minerals like Zinc and Magnesium. This "toxic substitution" weakens the structural proteins of the myocyte and promotes the very fibrosis that regenerative therapies are trying to overcome.
---
The Cascade: From Exposure to Disease
The journey to heart failure is rarely a sudden event; it is a "cascade" of biological failures exacerbated by the modern environment.
- —Systemic Inflammation: Chronic exposure to pollutants and a high-linoleic acid diet triggers a state of constant low-grade inflammation. This activates Fibroblasts, the cells responsible for laying down scar tissue.
- —Oxidative Stress: When the heart’s antioxidant defences (like Glutathione) are overwhelmed by environmental toxins, "Reactive Oxygen Species" (ROS) damage the DNA of the cardiomyocytes.
- —Epigenetic Silencing: The "regenerative genes" that are active during our time in the womb are not gone; they are "silenced" by epigenetic markers. Environmental toxins act as "silencers," ensuring that the heart remains in a state of permanent non-repair.
- —Microvascular Dysfunction: Before the large coronary arteries fail, the tiny capillaries—the Microvasculature—are damaged. This starves the myocytes of oxygen and nutrients, making the heart more susceptible to a major attack and less capable of receiving stem cell therapies.
Recent data suggests that air pollution (specifically PM2.5 particles) is directly linked to an increase in myocardial fibrosis, even in individuals without overt cardiovascular disease.
---
What the Mainstream Narrative Omits
In the hallowed halls of traditional medicine, the focus remains stubbornly fixed on pharmaceutical interventions: Statins, Beta-Blockers, and ACE Inhibitors. While these drugs have their place in emergency management, they do absolutely nothing to regenerate the heart. In fact, they may actively hinder it.
The Statin Contradiction
Statins work by inhibiting the HMG-CoA reductase pathway to lower cholesterol. However, this same pathway is responsible for the production of Coenzyme Q10 (CoQ10), a vital nutrient for mitochondrial energy production in the heart. By depleting CoQ10, long-term statin use can paradoxically weaken the heart muscle, a condition some researchers have dubbed "statin-induced cardiomyopathy."
The Suppression of Autophagy
The body has a built-in "recycling" mechanism called Autophagy, where it breaks down damaged cells and proteins to create new ones. Prolonged fasting and specific dietary protocols can trigger autophagy in the heart. Yet, you will rarely hear a cardiologist prescribe a "fasting-mimicking diet" to clear out cardiac fibrosis. Why? Because there is no profit in a patient who heals themselves through the strategic absence of food.
The Ethics and Economics of Stem Cells
The "Gold Standard" of cardiac regeneration—iPSCs—is incredibly expensive to produce. There is a quiet tension in the medical-industrial complex: is it better to develop a one-time regenerative cure, or a series of expensive, lifelong "management" drugs? Currently, the funding for the latter vastly outweighs the former. Furthermore, the push for "Off-the-Shelf" (allogeneic) stem cell products—which would be easier to patent and mass-produce—often ignores the superior safety and efficacy of "Patient-Specific" (autologous) therapies.
The mRNA Controversy
We cannot discuss cardiac health in the current era without addressing the "elephant in the room": the reported rise in Myocarditis and Pericarditis following the mass administration of lipid-nanoparticle-based mRNA platforms. The mainstream narrative asserts these cases are "mild and transient," but from a biological perspective, any inflammation of the heart muscle results in the death of myocytes and the formation of microscopic scars. This creates a "regenerative debt" that the heart may not be able to pay back in the years to come.
---
The UK Context
The United Kingdom presents a unique landscape for cardiac research and challenges. With an ageing population and a high prevalence of metabolic syndrome, the NHS is currently buckling under the weight of heart failure cases.
The British Heart Foundation (BHF) and "Mending Broken Hearts"
The BHF has been at the forefront of funding regenerative research in the UK. Their "Mending Broken Hearts" appeal has poured millions into Centres of Regenerative Medicine in London, Edinburgh, and Oxford. British researchers are currently pioneering the use of "Heart Patches"—engineered tissue grown in the lab that can be surgically sewn onto a patient’s heart to provide new myocytes and structural support.
The NHS Paradox
While the UK boasts world-class researchers, the NHS’s "standard of care" remains heavily reliant on outdated models. There is a significant lag—often decades—between a laboratory breakthrough and its availability to the average patient in Birmingham or Manchester. Furthermore, the UK’s environmental landscape, characterised by high levels of urban pollution and a reliance on processed, glyphosate-heavy "convenience" foods, creates a "toxic soup" that counteracts much of the good work being done in regenerative clinics.
The "North-South" Health Divide
In the UK, cardiovascular mortality is significantly higher in the North of England and Scotland compared to the South East. This is not just a matter of "lifestyle choices" but is deeply tied to industrial legacies, soil depletion of essential minerals like Selenium and Magnesium, and the lack of access to cutting-edge regenerative screenings.
---
Protective Measures and Recovery Protocols
If the goal is truly to heal the "broken heart," we must move beyond the laboratory and into a holistic framework that addresses both the cellular and environmental levels.
1. Nutritional Support for Myocyte Health
- —Coenzyme Q10 (Ubiquinol): Essential for mitochondrial ATP production.
- —Magnesium Taurate: Magnesium is the ultimate "relaxant" for the heart, and taurine is an amino acid that supports calcium handling.
- —L-Carnitine: Aids in the transport of fatty acids into the mitochondria for fuel.
- —Omega-3 Fatty Acids (DHA/EPA): Crucial for maintaining the fluidity of the myocyte membrane and reducing inflammation.
2. Promoting Endogenous Autophagy
Implementing a Time-Restricted Feeding (TRF) window of 16:8 or occasional 24-hour fasts can help the heart clear out "senescent" (zombie) cells and misfolded proteins that contribute to stiffness and fibrosis.
3. Mitigating Environmental Impact
- —Water Filtration: Using high-quality reverse osmosis filters to remove fluoride, chlorine, and heavy metals from drinking water.
- —EMF Hygiene: Turning off Wi-Fi routers at night and using wired connections where possible to protect the heart’s delicate electrical signalling.
- —Organic Nutrition: Choosing organic produce to minimise glyphosate and pesticide exposure.
4. Advanced Therapies (The "Innerstanding" Approach)
- —Peptide Therapy: Compounds like BPC-157 (Body Protection Compound) have shown remarkable angiogenic properties in animal models, helping to grow new blood vessels into damaged heart tissue.
- —Hyperbaric Oxygen Therapy (HBOT): By increasing the concentration of dissolved oxygen in the blood, HBOT can stimulate the recruitment of circulating stem cells to the site of injury.
- —Pulsed Electromagnetic Field (PEMF) Therapy: Using specific, low-frequency fields to support the heart’s natural rhythm and enhance cellular repair.
---
Summary: Key Takeaways
The road to true cardiac regeneration is not merely a technical challenge of injecting cells into a muscle; it is a battle against a biological and environmental system that seems designed for degradation.
- —Myocytes are the goal: Replacing lost heart muscle cells is the only way to reverse heart failure; everything else is just slowing the decline.
- —iPSCs are the future: Reprogramming a patient's own cells offers the best hope for integration without rejection, provided we can solve the "arrhythmia" problem.
- —The Environment is the enemy: You cannot heal a heart in the same environment that broke it. Glyphosate, EDCs, and EMFs are the silent saboteurs of regeneration.
- —Mainstream medicine is incomplete: Current protocols focus on "managing" the scar rather than removing it. Autophagy and mitochondrial support are the missing pieces of the puzzle.
- —UK leadership is vital: The UK has the research talent to lead the world in "Heart Patches" and stem cell technology, but the NHS must be willing to embrace these "disruptive" cures.
In the final analysis, "Innerstanding" the heart means recognising it not as a mechanical pump, but as a sophisticated bio-electrical organ that requires a clean environment, specific nutrients, and the courage to challenge the pharmaceutical status quo. The "broken heart" can be healed, but only if we are willing to look at the whole human being, not just the muscle.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Cardiac Regeneration: Healing the Broken Heart with Myocytes"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Stem Cell Science & Regenerative Medicine — products curated by our research team for educational relevance and biological support.

Energy Blend Supports

Peptides, one of the secret Russian military health marvels, now available. 40 years research

Albedextrin – Specialist Cyclodextrin Complex
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper