Endocannabinoid Tone: The Master Regulator of Nociceptive Thresholds
The endocannabinoid system is the body's primary mechanism for maintaining homeostasis and modulating pain. Clinical endocannabinoid deficiency may be the root cause of conditions like migraine and fibromyalgia.
Overview
The human biological architecture is governed by a complex hierarchy of regulatory systems, but none is as foundational, or as historically neglected, as the Endocannabinoid System (ECS). Often referred to as the ‘master rheostat’ of the body, the ECS is a pervasive lipid-signalling system that appeared in evolutionary history over 600 million years ago. Its primary objective is the maintenance of homeostasis—biological stability—amidst an ever-changing and often hostile environment. Within the realm of pain science, the ECS serves as the ultimate arbiter of nociceptive thresholds, determining how we perceive, process, and ultimately resolve painful stimuli.
The concept of 'Endocannabinoid Tone' refers to the baseline functional status of this system. It is the summation of the density of cannabinoid receptors, the concentration of endogenous ligands (endocannabinoids), and the efficiency of the enzymes responsible for their synthesis and degradation. When this tone is optimal, the body remains resilient, effectively 'muting' the background noise of minor physiological stressors. However, when this tone is compromised, the threshold for pain drops significantly, leading to a state of hyperalgesia and central sensitisation.
In this comprehensive exploration, we will deconstruct the sophisticated mechanics of the ECS, exposing how modern environmental pressures have led to a silent epidemic of Clinical Endocannabinoid Deficiency (CECD). This deficiency is not merely a hypothetical construct; it is the likely common denominator in a spectrum of treatment-resistant conditions, including fibromyalgia, migraine, and irritable bowel syndrome (IBS). As we peel back the layers of mainstream medical dogma, we find that the failure to address endocannabinoid tone is the primary reason why chronic pain remains one of the most significant burdens on the UK’s public health infrastructure.
##
The Biology — How It Works
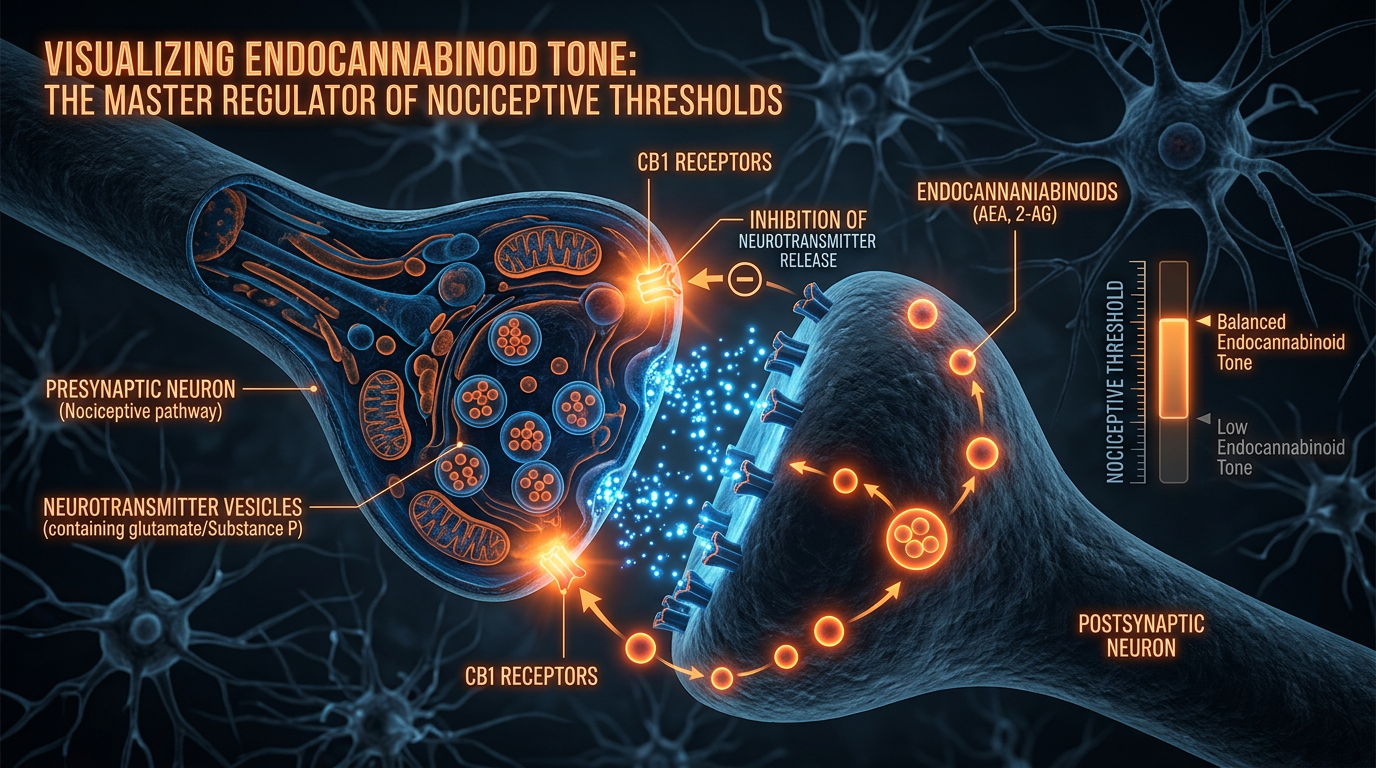
To understand the ECS, one must move beyond the reductive view of it being merely a 'cannabis receptor' system. It is a sophisticated, "on-demand" signalling network that operates primarily through retrograde neurotransmission. While most neurotransmitters (like glutamate or GABA) travel from a pre-synaptic neuron to a post-synaptic neuron, endocannabinoids travel in reverse. They are synthesised in the post-synaptic neuron and travel 'backwards' across the synaptic cleft to bind with receptors on the pre-synaptic terminal. This allows the post-synaptic cell to provide feedback, essentially telling the sending neuron to 'slow down' or 'hush.'
The system is composed of three primary pillars:
1. The Receptors: CB1 and CB2
Cannabinoid Receptor Type 1 (CB1) is one of the most abundant G-protein coupled receptors in the mammalian brain. It is concentrated in the cortex, basal ganglia, hippocampus, and cerebellum, but crucially, it is also heavily populated in the dorsal horn of the spinal cord and the periaqueductal gray—areas central to pain processing. CB2 receptors, by contrast, are found predominantly in the immune system and peripheral tissues. They modulate inflammatory responses and cytokine release, acting as a brake on the 'inflammatory fire' that often precedes chronic pain.
2. The Ligands: AEA and 2-AG
The body produces its own 'internal cannabis' molecules. The most prominent are Anandamide (N-arachidonoylethanolamine, or AEA) and 2-Arachidonoylglycerol (2-AG). Anandamide, named after the Sanskrit word for 'bliss,' is a high-affinity partial agonist for CB1. It is involved in mood regulation, the 'runner's high,' and the immediate suppression of acute pain. 2-AG exists in much higher concentrations in the brain and acts as a full agonist for both CB1 and CB2, playing a more substantial role in managing systemic inflammation and long-term homeostatic balance.
3. The Enzymes: FAAH and MAGL
Unlike traditional neurotransmitters that are stored in vesicles, endocannabinoids are synthesised from cell membrane lipids exactly when and where they are needed. Once they have delivered their signal, they are rapidly broken down by specific enzymes. Fatty Acid Amide Hydrolase (FAAH) is the primary enzyme that degrades Anandamide, while Monoacylglycerol Lipase (MAGL) breaks down 2-AG. The 'tone' of the system is largely determined by the activity of these enzymes. If FAAH is overactive, Anandamide levels plummet, the 'bliss' is extinguished, and the pain gate swings wide open.
In the UK, chronic pain affects approximately 15.5 million people—roughly 34% of the population. A significant percentage of these cases involve 'nociplastic' pain, where the nervous system remains in a state of high alert despite the absence of ongoing tissue damage, a hallmark of low endocannabinoid tone.
##
Mechanisms at the Cellular Level
At the microscopic level, the ECS functions as a sophisticated filter. In the context of nociception (the sensing of pain), the system acts at multiple levels of the neuraxis. When a peripheral injury occurs, nociceptors send signals via the dorsal root ganglia to the spinal cord. Here, the ECS performs its first major intervention.
Retrograde Inhibition and the Glutamate Brake
When the spinal cord is flooded with excitatory neurotransmitters like glutamate (the primary 'go' signal for pain), the post-synaptic neurons become overstimulated. In response, they synthesise AEA and 2-AG. These molecules travel back across the synapse to the CB1 receptors on the excitatory pre-synaptic terminals. This activation inhibits the influx of calcium ions, effectively shutting down the release of further glutamate. This is the body’s natural opioid-independent analgesic mechanism. If the ECS is functioning correctly, the 'volume' of the pain signal is turned down before it even reaches the brain.
The Periaqueductal Gray (PAG) and Descending Control
The ECS also governs the 'Top-Down' control of pain. The PAG is a key control centre in the midbrain for the descending modulatory system. When we experience fear, stress, or intense focus, the ECS triggers the PAG to send signals down the spinal cord to inhibit incoming pain. This is why a soldier might not feel a wound in the heat of battle. High endocannabinoid tone ensures that this descending inhibitory pathway is 'primed' and ready. In patients with fibromyalgia, this pathway is often dysfunctional; instead of inhibiting pain, the system may actually facilitate it, a process known as 'descending facilitation.'
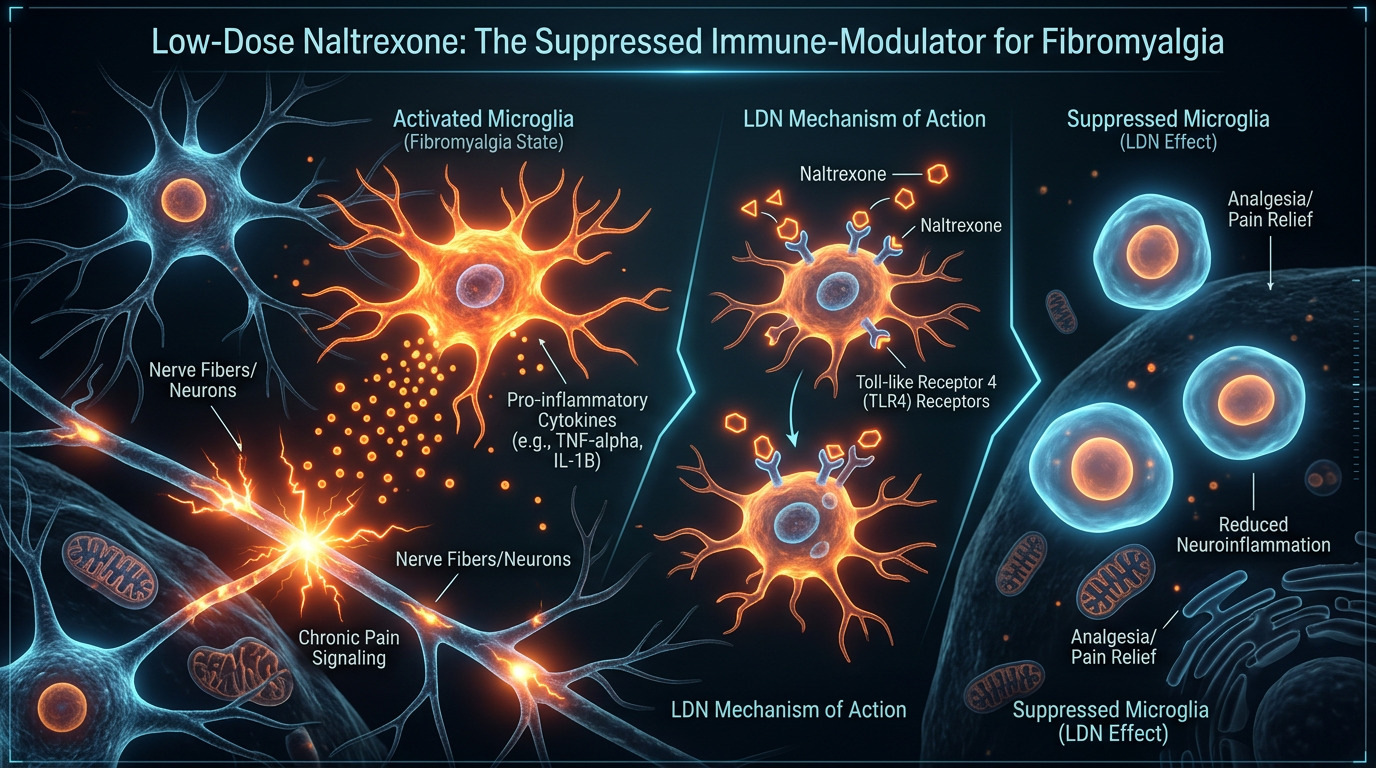
Microglial Modulation and Neuroinflammation
Beyond the neurons, the ECS is the primary regulator of microglia—the resident immune cells of the brain and spinal cord. When microglia become chronically activated, they release pro-inflammatory cytokines and neurotoxins that irritate surrounding neurons, creating a 'vicious cycle' of neuroinflammation and pain. CB2 receptor activation on microglia shifts them from a pro-inflammatory (M1) state to an anti-inflammatory, neuroprotective (M2) state. A robust endocannabinoid tone prevents the transition from acute injury to permanent neuroinflammatory chronic pain.
##
Environmental Threats and Biological Disruptors
The tragedy of the 21st century is that our modern lifestyle is an inadvertent assault on the ECS. We are living in a state of 'evolutionary mismatch,' where our environment actively degrades the very system meant to protect us from stress.
The Great Lipid Imbalance: Omega-6 vs. Omega-3
Endocannabinoids are derived from arachidonic acid, an Omega-6 fatty acid. While this sounds positive, the modern Western diet—heavily saturated with ultra-processed seed oils (soybean, sunflower, corn oils)—has created a massive oversupply of Omega-6 and a deficiency in Omega-3 (found in oily fish and flax). This imbalance creates 'noisy' endocannabinoid signalling. Excessive Omega-6 leads to an overproduction of pro-inflammatory arachidonic acid derivatives, which can over-stimulate CB1 receptors in the short term, leading to 'downregulation' or a decrease in receptor density over time. This leaves the system unresponsive and depleted.
Endocrine Disruptors and 'Body Burden'
The UK environment is saturated with endocrine-disrupting chemicals (EDCs), from phthalates in plastics to pesticides like glyphosate in our food chain. Research has shown that certain EDCs can interfere with cannabinoid receptor binding and inhibit the enzymes responsible for endocannabinoid synthesis. This 'chemical interference' essentially 'mutes' the ECS, preventing it from responding to physiological stressors.
Chronic Cortisol and HPA-Axis Exhaustion
The ECS and the Hypothalamic-Pituitary-Adrenal (HPA) axis are inextricably linked. The ECS acts as the 'off switch' for the stress response. However, chronic, unrelenting psychological stress leads to sustained high levels of cortisol. Prolonged cortisol exposure has been shown to increase FAAH activity, which aggressively breaks down Anandamide. This creates a state of 'anhedonia' (inability to feel pleasure) and hyperalgesia. We are essentially 'burning through' our internal bliss molecules just to survive the daily grind, leaving nothing left to manage physical pain.
Statistics from the Health and Safety Executive (HSE) indicate that in 2022/23, 875,000 UK workers suffered from work-related stress, depression, or anxiety. This psychological burden is a direct precursor to systemic endocannabinoid depletion and subsequent chronic pain syndromes.
##
The Cascade: From Exposure to Disease
Clinical Endocannabinoid Deficiency (CECD) is the theoretical framework that bridges the gap between environmental stress and chronic disease. First proposed by Dr. Ethan Russo, CECD suggests that certain individuals possess a genetically or environmentally induced low 'tone' of the ECS, which manifests as a triad of symptoms: migraine, fibromyalgia, and IBS.
The Path to Fibromyalgia
In fibromyalgia, the nervous system’s 'gain' is turned up too high. Studies using functional MRI have shown that fibromyalgia patients have reduced CB1 receptor binding in regions of the brain associated with pain processing. Because the ECS cannot provide the necessary 'retrograde inhibition' at the spinal level, even normal sensory input (like touch or temperature) is perceived as painful. This is not a problem with the muscles or joints; it is a failure of the master regulator—the ECS—to gate the signals.
The Migraine Connection
Migraine is increasingly viewed as a 'neuro-inflammatory storm.' Anandamide is a potent inhibitor of the trigeminovascular system, the primary pathway involved in migraine pain. Research has shown that patients with chronic migraines have significantly lower levels of Anandamide in their cerebrospinal fluid. When the ECS tone drops, the trigeminal nerve becomes hypersensitive, and the threshold for triggering a migraine cascade falls.
IBS and the Enteric Nervous System
The 'second brain' in the gut is densely packed with CB1 and CB2 receptors. They regulate gastric motility, secretion, and visceral sensation. In IBS, the lack of endocannabinoid control leads to 'visceral hypersensitivity'—where the normal movement of gas or food through the intestines is felt as intense pain. This explains why IBS so frequently co-occurs with fibromyalgia and migraine; they are all manifestations of the same underlying regulatory failure.
##
What the Mainstream Narrative Omits
The refusal of the medical establishment to place endocannabinoid tone at the centre of chronic pain management is not an accident; it is a systemic failure driven by pharmacological reductionism and historical bias.
The Failure of the 'Single-Target' Model
Modern pharmacology is built on the 'one drug, one target' model. This is fundamentally at odds with the ECS, which is a 'multi-target' pleiotropic system. Pharmaceutical companies have attempted to create synthetic cannabinoids or FAAH inhibitors, but many of these trials have failed because they lack the 'entourage effect'—the synergistic interaction of various molecules found in nature. By ignoring the holistic nature of the ECS, the industry continues to push 'band-aid' solutions like synthetic opioids or gabapentinoids, which often cause more harm than good and do nothing to restore homeostatic tone.
The Stigma and the 'War on Research'
For decades, the association of the ECS with the cannabis plant led to a de facto ban on comprehensive research. Even after the discovery of the receptors in the 1990s, medical schools in the UK have been notoriously slow to include the ECS in their curricula. It is estimated that less than 15% of UK medical schools offer specific modules on the endocannabinoid system. This 'educational blackout' ensures that the next generation of doctors remains reliant on outdated models of pain management, unaware that they are ignoring the body's primary self-healing mechanism.
The Opioid Misdirection
The mainstream response to the chronic pain crisis was the aggressive over-prescription of opioids. We now know that opioids can actually cause 'opioid-induced hyperalgesia'—making the patient *more* sensitive to pain over time—and they significantly suppress the body's natural endocannabinoid production. The medical establishment’s focus on exogenous opioids has actively contributed to the erosion of endogenous endocannabinoid tone, creating a cycle of dependency and escalating pain.
##
The UK Context
The UK presents a unique landscape for the endocannabinoid crisis. Despite the legalisation of medical cannabis in 2018, access remains prohibitively difficult for the vast majority of patients.
The NHS Barrier
The National Institute for Health and Care Excellence (NICE) guidelines are notoriously restrictive regarding the ECS and cannabinoid therapies. As a result, the NHS rarely prescribes medical cannabis, forcing patients to turn to expensive private clinics or the illicit market. This creates a 'two-tier' system where only the wealthy can access therapies that directly target endocannabinoid tone.
According to the Centre for Medicinal Cannabis, approximately 1.8 million people in the UK are using 'street' cannabis to self-medicate for chronic health conditions. This highlights a staggering disconnect between public need and official medical policy.
The 'Stiff Upper Lip' and Silent Suffering
The British cultural tendency toward 'grinning and bearing it' often masks the true scale of the pain crisis. Chronic pain in the UK is frequently dismissed as 'psychosomatic' or 'age-related,' particularly in women. This gaslighting of patients further increases psychological stress, which, as established, further depletes endocannabinoid tone. The result is a population that is biologically 'brittle,' lacking the internal resilience to handle the stressors of modern life.
The Cost of Inaction
The economic impact of chronic pain in the UK is estimated to be billions of pounds annually in lost productivity and healthcare costs. By refusing to acknowledge and treat Clinical Endocannabinoid Deficiency, the UK government and health services are presiding over a preventable crisis of human suffering.
##
Protective Measures and Recovery Protocols
Restoring endocannabinoid tone is not an overnight process; it requires a multi-faceted approach that addresses diet, environment, and lifestyle. The goal is to 'upregulate' receptors and optimise the levels of AEA and 2-AG.
Dietary Recalibration
The first step is to fix the Omega-6 to Omega-3 ratio.
- —Eliminate Seed Oils: Remove sunflower, safflower, and rapeseed oils, which are high in pro-inflammatory Omega-6.
- —Flood the System with Omega-3s: High-quality EPA and DHA from small, oily fish (sardines, mackerel) provide the building blocks for healthy cell membranes, allowing receptors to function optimally.
- —Polyphenols: Compounds like EGCG (in green tea), quercetin (in onions/apples), and curcumin (in turmeric) have been shown to modulate the ECS and reduce neuroinflammation.
Lifestyle Interventions for 'Tone'
The ECS responds remarkably well to specific non-pharmacological interventions.
- —Aerobic Exercise: Moderate-intensity exercise (reaching about 70-80% of max heart rate) is the most effective way to trigger a surge in Anandamide. This is the biological basis of the 'runner's high.'
- —Cold Exposure: Brief, deliberate cold exposure (cold showers or ice baths) has been shown to increase CB1 receptor density and enhance the ECS’s ability to manage stress.
- —Stress Management: Practices that lower cortisol—such as deep breathing, meditation, and forest bathing—directly protect Anandamide from being degraded by FAAH.
Targeted Supplementation and Phyto-Support
While medical cannabis is one route, other plants can support the ECS.
- —Caryophyllene: This is a terpene found in black pepper, cloves, and hemp. It is a 'dietary cannabinoid' that selectively binds to the CB2 receptor, providing potent anti-inflammatory effects without any psychoactive 'high.'
- —Palmitoylethanolamide (PEA): A fatty acid amide produced by the body that is also available as a supplement. It works by inhibiting FAAH, thereby naturally raising Anandamide levels. It is highly effective for neuropathic pain.
- —Magnesium: Magnesium is essential for G-protein coupled receptor function. Deficiency—which is rampant in the UK—directly impairs the ECS's ability to signal.
Environmental Detoxification
Reducing the 'body burden' of EDCs is crucial.
- —Filter Your Water: UK tap water can contain traces of pharmaceuticals and pesticides. High-quality carbon or reverse osmosis filters are essential.
- —Switch to Organic: Whenever possible, avoid 'The Dirty Dozen' fruits and vegetables that are most heavily sprayed with pesticides that disrupt the ECS.
- —Reduce Plastic Exposure: Avoid heating food in plastic containers and switch to glass or stainless steel to minimize phthalate and BPA exposure.
##
Summary: Key Takeaways
The Endocannabinoid System is the most significant physiological system you have likely never been taught about. Its role as the 'Master Regulator' of nociceptive thresholds makes it the ultimate target for the prevention and treatment of chronic pain.
- —Tone is Everything: Your baseline 'Endocannabinoid Tone' determines your resilience to pain. Low tone equals high pain sensitivity.
- —CECD is a Reality: Migraine, Fibromyalgia, and IBS are not separate conditions but symptoms of a singular underlying deficiency in the ECS.
- —The Modern Assault: Our diet, stress levels, and environment are actively 'eroding' our ECS tone, leading to a silent epidemic of chronic suffering.
- —Mainstream Failure: The pharmaceutical industry and medical establishment have largely ignored the ECS in favour of profitable, single-target 'band-aid' drugs that often exacerbate the problem.
- —The UK Crisis: Millions of Britons are suffering needlessly due to a lack of education and access to ECS-focused therapies.
- —Empowerment through Action: Restoring the ECS is possible through targeted dietary shifts, stress reduction, and the use of natural compounds that support our internal 'bliss' molecules.
The shift toward an endocannabinoid-centric model of health represents a revolution in pain science. By understanding and nurturing this ancient regulatory system, we can move beyond the management of symptoms and toward the restoration of true biological homeostasis. The path to a pain-free life is not found in a new 'magic bullet' pill, but in the intelligent support of the body's own master regulator.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Endocannabinoid Tone: The Master Regulator of Nociceptive Thresholds"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper