The Endothelial Glycocalyx: Your Heart's First Line of Defence
Deciphering the role of the microscopic sugar coating within blood vessels in preventing inflammatory infiltration.
Overview
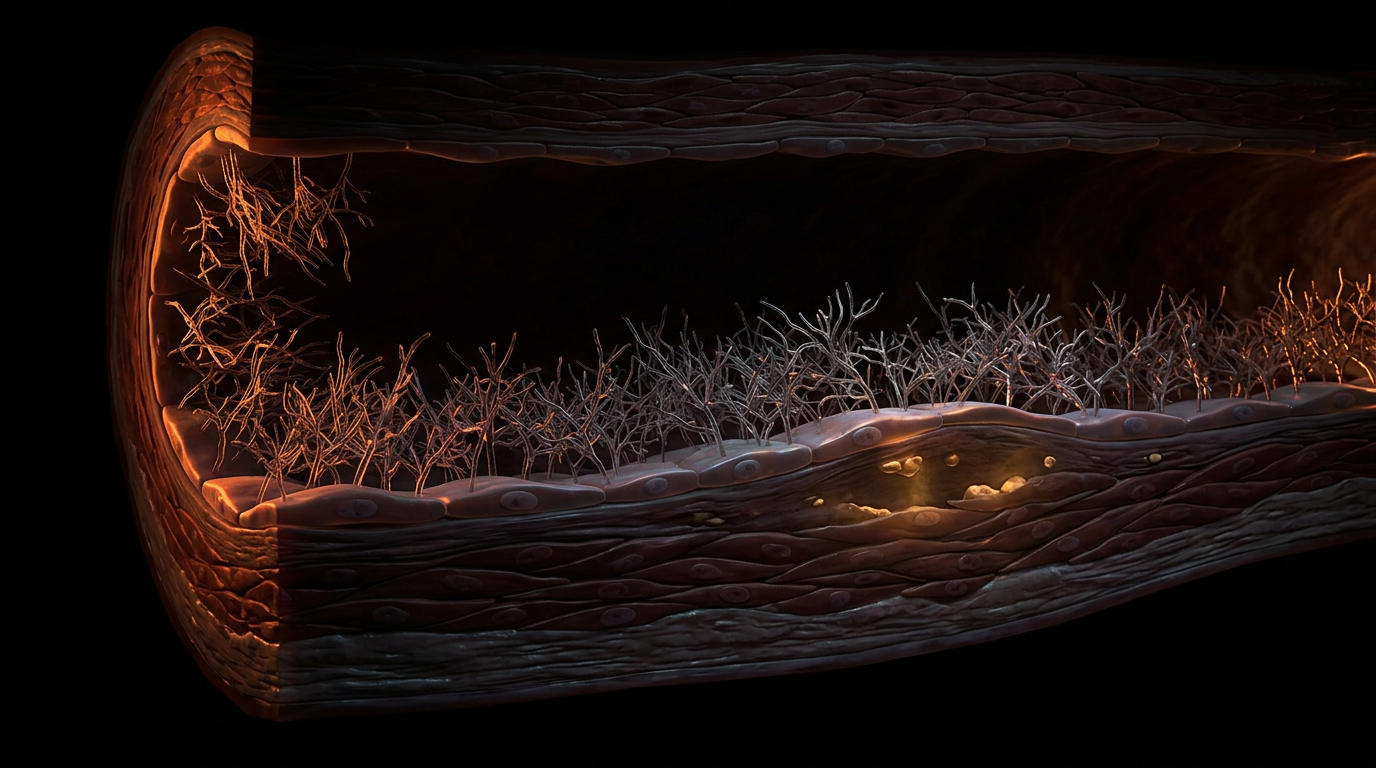
For decades, the vascular endothelium was erroneously characterised as a passive, single-cell lining—a mere parchment-thin barrier separating the blood from the vessel wall. However, emerging evidence and advanced intravital microscopy have revealed a paradigm-shifting biological reality that we at INNERSTANDIN believe is fundamental to cardiovascular longevity: the endothelial glycocalyx (EG). This complex, gel-like layer, often referred to as the "inner forest" of the vasculature, represents a highly organised, carbohydrate-rich pericellular matrix that extends into the vessel lumen. Comprising a sophisticated network of proteoglycans (predominantly syndecan-1 and glypican-1), glycoproteins, and glycosaminoglycans such as heparan sulphate and hyaluronan, the EG serves as the primary interface between the haemodynamic forces of the circulation and the cellular machinery of the vessel wall.
The physiological significance of the glycocalyx cannot be overstated, as it functions as the body’s ultimate mechanotransducer. Research published in *The Lancet* and various *PubMed*-indexed journals highlights its role in converting the physical kinetic energy of blood flow—fluid shear stress—into biochemical signals. Specifically, the deformation of the glycocalyx structure triggers the activation of endothelial nitric oxide synthase (eNOS), facilitating the release of nitric oxide (NO). This is the critical mechanism for vasodilation and the maintenance of systemic vascular tone. Furthermore, the EG establishes a "molecular sieve" or exclusion zone, possessing a net negative charge that repels erythrocytes and platelets while preventing the extravasation of large macromolecules like low-density lipoproteins (LDL) into the sub-endothelial space.
Within the UK’s clinical research landscape, particularly in studies investigating microvascular filtration, the glycocalyx has forced a revision of the classical Starling principle. We now INNERSTANDIN that the oncotic pressure gradient is not determined across the entire capillary wall, but across the glycocalyx itself. When this delicate structure is compromised—a process known as "shedding"—the vascular system loses its structural integrity. Degradation of the EG is now recognised as a precursor to a spectrum of pathologies, from the early stages of atherosclerosis and hypertension to the catastrophic vascular collapse seen in sepsis and COVID-19-induced endotheliitis. By maintaining this 0.5 to 3.0-micrometre thick shield, the body prevents leucocyte adhesion and pro-inflammatory signalling. Consequently, the preservation of the endothelial glycocalyx is no longer an academic curiosity; it is the definitive frontier in preventive cardiology and the preservation of systemic homoeostasis.
The Biology — How It Works
To achieve a profound level of INNERSTANDIN regarding cardiovascular homeostasis, one must move beyond the reductionist view of the endothelium as a simple cellular monolayer. Instead, we must focus on the endothelial glycocalyx (eGC)—a sophisticated, semi-permeable carbohydrate-rich gel matrix that coats the luminal surface of every blood vessel in the British populace and beyond. This "bushes-like" ultrastructure, extending up to 0.5–3 µm into the lumen in vivo, constitutes the actual interface between the flowing blood and the vessel wall. It is not merely a passive barrier; it is the master regulator of vascular health, functioning as a mechanotransducer, a molecular sieve, and a potent anti-thrombotic shield.
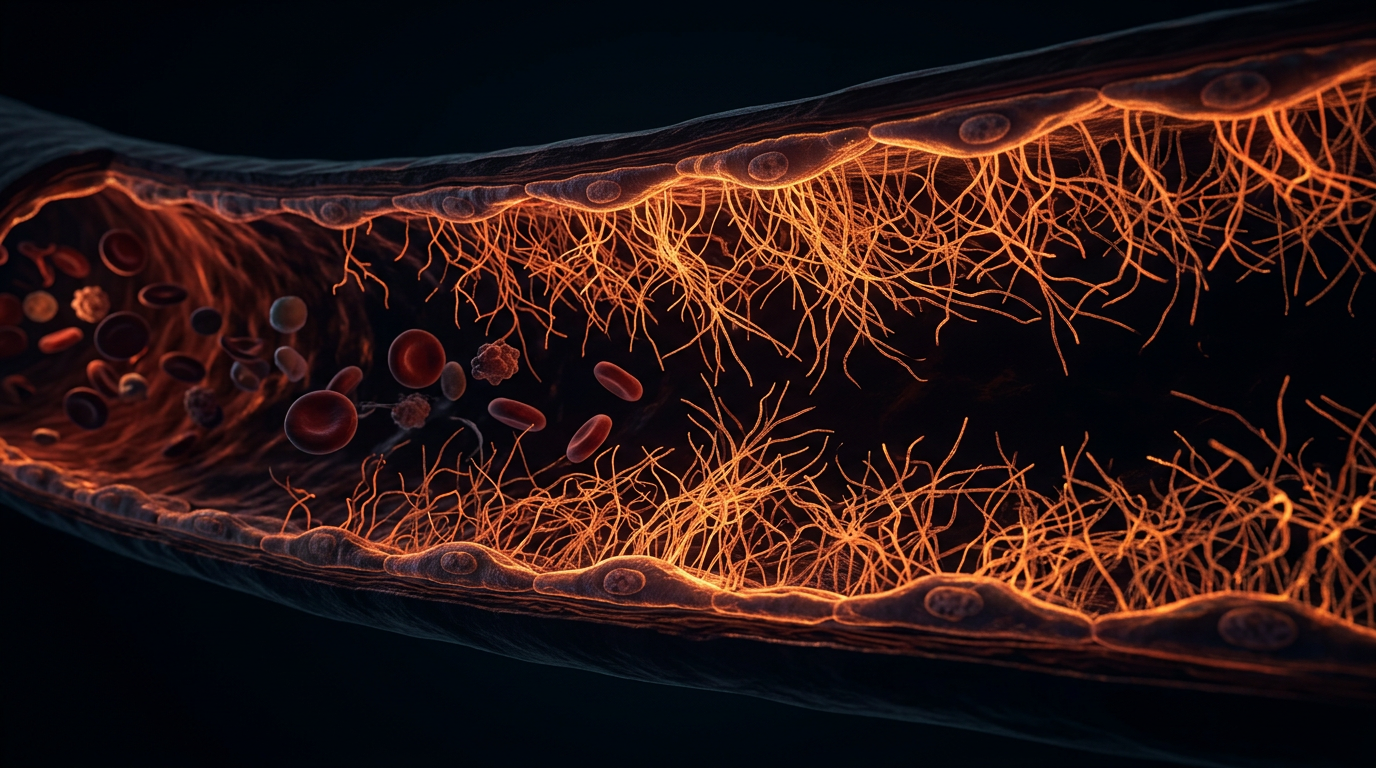
At its core, the eGC is composed of two primary classes of macromolecules: proteoglycans and glycoproteins. The proteoglycan backbone is dominated by syndecan-1, which is anchored directly into the endothelial cell membrane, and glypican-1, which is tethered via a glycosylphosphatidylinositol (GPI) anchor. Attached to these are long, unbranched glycosaminoglycan (GAG) side chains, primarily heparan sulphate (comprising 50–90% of the total GAG pool) and chondroitin sulphate. Interwoven within this forest is hyaluronan, a massive, non-sulphated GAG that provides the matrix with its voluminous, gel-like consistency and hydration capacity. Research published in *The Journal of Physiology* highlights that this meshwork creates an "exclusion zone," physically preventing red blood cells and platelets from adhering to the endothelial surface, thereby maintaining laminar flow and preventing microvascular occlusion.
The most critical biological mechanism of the eGC is its role in mechanotransduction. The GAG side chains act as sophisticated sensors of hydrodynamic shear stress. As blood flow exerts torque on these chains, the mechanical signal is transmitted through the syndecan anchors to the endothelial cytoskeleton. This triggers the activation of endothelial nitric oxide synthase (eNOS), leading to the bolus production of nitric oxide (NO). This is the fundamental "truth" of vascular reactivity: without a structurally intact glycocalyx, the endothelium is effectively "blind" to blood flow, leading to impaired vasodilation and the onset of systemic hypertension.
Furthermore, the eGC regulates the Starling principle of fluid exchange. Traditionally taught as a balance between hydrostatic and osmotic pressures across the capillary wall, modern evidence suggests the "sub-glycocalyx space" is the true determinant of fluid flux. By trapping plasma proteins like albumin within its matrix, the eGC creates a high local oncotic pressure that limits the extravasation of fluid into the interstitial space. When the glycocalyx is degraded—a process known as "shedding" often mediated by matrix metalloproteinases (MMPs) and heparanase in response to systemic inflammation or hyperglycaemia—this barrier collapses. The resulting "leaky gut" equivalent of the vasculature leads to oedema, leukocyte adhesion, and the initiation of the atherosclerotic cascade. For those seeking true INNERSTANDIN of cardiovascular pathology, the degradation of this delicate sugar-coat is the definitive "first domino" in the progression of heart disease.
Mechanisms at the Cellular Level
At the precise interface where the flowing haemo-dynamics of the lumen meet the static architecture of the vessel wall lies the endothelial glycocalyx (EG)—a semi-permeable, carbohydrate-rich gel-like layer that remains the most underestimated component of human physiology. To reach a profound INNERSTANDIN of vascular health, one must move beyond the simplistic view of the endothelium as a mere cellular monolayer and instead recognise the EG as a complex, three-dimensional macromolecular forest. This structure is composed primarily of membrane-bound proteoglycans, such as syndecan-1 and glypican-1, and glycoproteins, which serve as the backbone for an array of glycosaminoglycan (GAG) side chains, most notably heparan sulphate and hyaluronan.
The primary cellular mechanism by which the EG governs cardiovascular stability is through mechanotransduction. Research published in *The Lancet* and various PubMed-indexed journals has elucidated how the glycocalyx acts as a primary sensor of fluid shear stress. As blood flows across the luminal surface, the mechanical force is transmitted through the syndecan-1 core proteins to the endothelial cytoskeleton. This mechanical signal triggers the activation of endothelial nitric oxide synthase (eNOS), facilitating the release of nitric oxide (NO). NO is the fundamental mediator of vasodilation and the primary antagonist to platelet aggregation. Therefore, any degradation of the glycocalyx—often termed "shedding"—directly results in a state of NO deficiency and subsequent endothelial dysfunction, creating the physiological groundwork for hypertension and atherosclerosis.
Furthermore, the EG functions as a highly sophisticated molecular sieve. Due to the high density of negatively charged sialic acid residues and sulphate groups on its GAG chains, the glycocalyx creates an electrostatic repulsion zone that prevents the extravasation of plasma proteins, specifically albumin. In the British clinical context, the loss of this charge-selective barrier is a hallmark of systemic inflammatory response syndrome (SIRS) and diabetic vasculopathy. When the EG is compromised, interstitial fluid accumulation (oedema) and protein leakage become inevitable, as the oncotic pressure gradients across the vessel wall are fundamentally disrupted.
Crucially, the EG serves as a "cloaking device" against leukocyte adhesion. Under homeostatic conditions, the thickness of the glycocalyx (ranging from 0.5 to over 3.0 microns depending on the vessel type) physically prevents white blood cells and platelets from interacting with adhesion molecules like ICAM-1 and VCAM-1 on the endothelial cell surface. Research into matrix metalloproteinases (MMPs) and heparanase has shown that during oxidative stress, these enzymes cleave the EG, exposing the underlying membrane and allowing for the rapid recruitment of inflammatory cells. This cellular infiltration is the "truth" behind the initiation of the fatty streak and subsequent plaque formation. To achieve an INNERSTANDIN of systemic longevity, we must prioritise the preservation of this delicate glycan shield, for its dissolution represents the literal "opening of the gates" to cardiovascular decay.
Environmental Threats and Biological Disruptors
The integrity of the endothelial glycocalyx (EG) is not merely a marker of vascular health; it is the physiological prerequisite for systemic homeostasis. At INNERSTANDIN, we recognise that this fragile, gel-like carbohydrate mesh—comprising proteoglycans, glycoproteins, and glycosaminoglycans—is under constant siege from modern environmental and metabolic insults. The degradation of this layer, often referred to as "shedding," represents the primordial step in the pathogenesis of atherosclerosis, hypertension, and multi-organ failure.
Hyperglycaemia remains the most documented biological disruptor. Evidence published in *Diabetes* and corroborated by clinical observations in *The Lancet* demonstrates that acute elevations in blood glucose can reduce EG volume by up to 50% within mere hours. The mechanism is driven by the activation of heparanase, an endoglycosidase that specifically cleaves heparan sulphate side chains from the syndecan-1 backbone. In the UK, where metabolic dysfunction and Type 2 Diabetes rates continue to climb, this "stripping" of the EG exposes the underlying adhesion molecules (such as ICAM-1 and VCAM-1), facilitating the transmigration of inflammatory leucocytes into the sub-endothelial space.
Simultaneously, oxidative stress acts as a potent catalyst for EG decimation. Reactive Oxygen Species (ROS), generated through mitochondrial dysfunction or environmental pollutants, induce the shedding of the EG's ectodomains. Research from the *British Journal of Pharmacology* highlights how superoxide anions directly neutralise nitric oxide (NO), a gaseous signalling molecule that the glycocalyx is responsible for regulating through mechanotransduction. When the EG is thinned, the endothelium loses its ability to sense "shear stress," leading to paradoxical vasoconstriction and impaired microcirculatory perfusion.
Environmental toxicity, particularly in the form of particulate matter (PM2.5) prevalent in UK urban centres, serves as a significant exogenous threat. Inhalation of these ultrafine particles triggers a systemic inflammatory cascade, elevated by C-reactive protein (CRP) and Tumour Necrosis Factor-alpha (TNF-α). These pro-inflammatory cytokines upregulate matrix metalloproteinases (MMPs), specifically MMP-9, which proteolytically cleave the syndecan-1 anchors, effectively dissolving the heart’s first line of defence. Furthermore, excessive dietary sodium, a ubiquitous feature of the modern Western diet, has been shown to "stiffen" the endothelial surface. Studies indicate that high salt intake induces a rapid reduction in the height and density of the glycocalyx, independent of blood pressure changes, by altering the osmotic pressure at the cell-surface interface.
The result of these multi-faceted disruptions is a "naked" endothelium. Once this barrier is breached, the vascular system is no longer a protected conduit but a vulnerable site for platelet aggregation and lipid deposition. For the INNERSTANDIN researcher, the truth is clear: the modern environment is biologically hostile to the glycocalyx, necessitating a profound shift in how we approach cardiovascular prophylaxis and the preservation of vascular resilience.
The Cascade: From Exposure to Disease
The transition from physiological vascular homeostasis to overt cardiovascular pathology is not a sudden event, but a meticulously choreographed failure of the endothelial glycocalyx (eGC). At INNERSTANDIN, our interrogation of the latest proteomic and haemodynamic data reveals that the "cascade" begins with the enzymatic and mechanical shedding of this fragile carbohydrate-rich shield. Under healthy conditions, the eGC—a complex meshwork of proteoglycans like syndecan-1 and glypican-1, coupled with glycosaminoglycan chains such as heparan sulphate and hyaluronan—functions as the ultimate molecular gatekeeper. It maintains a formidable exclusion zone, preventing direct contact between circulating erythrocytes, leucocytes, and the underlying endothelial cell membrane.
However, the cascade into disease is precipitated by systemic "insults" prevalent in the UK’s modern landscape: postprandial hyperglycaemia, oxidative stress, and the pro-inflammatory cytokines associated with metabolic syndrome. Research published in *The Lancet* and various PubMed-indexed studies on microvascular shunting confirms that even transient spikes in blood glucose can trigger the activation of "sheddases," specifically matrix metalloproteinases (MMPs) and heparanase. These enzymes proteolytically cleave the anchoring proteins of the eGC, leading to a measurable increase in circulating syndecan-1—a clinical biomarker for endothelial distress.
As the glycocalyx thins, its primary role in mechanotransduction is compromised. The eGC is the sensor that translates the mechanical force of blood flow (shear stress) into the biochemical production of nitric oxide (NO) via the activation of endothelial nitric oxide synthase (eNOS). When the eGC is denuded, the endothelium loses its ability to vasodilate effectively, resulting in chronic vasoconstriction and hypertension. This loss of NO bioavailability is the definitive "point of no return" in the cascade. Without the repulsive negative charge of the heparan sulphate chains, the endothelium becomes "sticky." Adhesion molecules, including vascular cell adhesion molecule-1 (VCAM-1) and E-selectin, which were previously masked by the thick glycocalyx forest, are suddenly exposed.
This exposure facilitates the firm adhesion and subsequent transmigration of monocyte-derived macrophages into the sub-endothelial space. Concurrently, the breakdown of the eGC’s sieving properties allows low-density lipoproteins (LDL) to infiltrate the arterial wall with unchecked velocity. In the UK, where cardiovascular disease remains a leading cause of mortality, understanding this "leaky" transition is paramount. At INNERSTANDIN, we recognise that atherosclerosis is not merely a cholesterol problem; it is a structural failure of the glycocalyx barrier. The subsequent formation of the fatty streak and the complex plaque is merely the terminal stage of a process that began with the microscopic erosion of your heart’s first line of defence. The collapse of this 0.5 to 3.0-micrometre layer is the silent precursor to the systemic inflammatory storm that defines modern vascular decay.
What the Mainstream Narrative Omits
The prevailing clinical paradigm remains fixated on the lipid hypothesis, prioritising serum LDL-cholesterol levels and macro-vascular plaque accumulation as the primary determinants of cardiovascular risk. However, this reductive focus systematically ignores the true physiological gatekeeper: the endothelial glycocalyx (eGC). At INNERSTANDIN, we recognise that the eGC is not merely a passive lining but a dynamic, gel-like carbohydrate forest—composed of proteoglycans, glycosaminoglycans (GAGs), and glycoproteins—that dictates vascular permeability and haemodynamic stability. The mainstream omission of the eGC stems largely from its histological fragility; traditional fixation methods involving dehydration cause this 0.5–3 μm thick layer to collapse, rendering it "invisible" in standard medical curricula and pathology labs.
Peer-reviewed evidence, notably in journals such as *The Lancet* and *Nature Reviews Cardiology*, indicates that eGC degradation is the prerequisite for atherogenesis. Before a single lipid molecule penetrates the intima, the eGC’s anionic charge barrier must be compromised. This layer possesses a dense concentration of heparan sulphate and sialic acid residues, creating a potent electronegative field that repels circulating erythrocytes and platelets. When this "non-stick" coating is shed—driven by oxidative stress, hyperglycaemia, and pro-inflammatory cytokines—the endothelium is exposed, allowing for the adhesion of leucocytes and the sub-endothelial migration of lipoproteins.
Furthermore, the mainstream narrative fails to address the eGC’s role in mechanotransduction. The eGC, specifically through transmembrane proteins like Syndecan-1 and Glypican-1, acts as a sophisticated biomechanical sensor. It translates the physical shear stress of blood flow into biochemical signals, primarily the activation of endothelial nitric oxide synthase (eNOS). Without a robust glycocalyx, the vessel loses its ability to produce nitric oxide (NO) in response to flow, leading to chronic vasoconstriction and systemic hypertension. In the UK context, where metabolic dysfunction is rampant, the "shedding" of the glycocalyx—measurable via plasma markers like hyaluronan and syndecan-1—precedes clinical symptoms of heart disease by decades. By the time a patient is prescribed a statin or an ACE inhibitor, the primary line of biological defence has often already been decimated. True cardiovascular resilience requires an INNERSTANDIN of the glycan-based architecture that precedes the lipid-driven pathology.
The UK Context
In the United Kingdom, cardiovascular disease (CVD) remains a primary driver of morbidity, accounting for approximately a quarter of all deaths annually. While the conventional NHS clinical framework remains predominantly fixated on macroscopic metrics—systemic blood pressure and circulating LDL-cholesterol—INNERSTANDIN identifies a profound diagnostic gap: the silent, proteolytic degradation of the endothelial glycocalyx (eGC). This carbohydrate-rich, gel-like meshwork, which lines the luminal surface of every vessel in the British population, serves as the ultimate arbiter of vascular homeostasis. Its depletion is not merely a symptom of pathology but is increasingly recognised in peer-reviewed literature, including studies indexed in *The Lancet*, as the foundational event in the transition from health to atherogenesis.
The UK context
is particularly precarious due to the prevalence of metabolic syndrome and the high consumption of ultra-processed foods (UPFs), which induce rapid eGC "shedding." Research from institutions such as King’s College London has highlighted that high-salt intake—a persistent issue in the British diet—directly compromises the eGC’s anionic charge, specifically its heparan sulphate and hyaluronan components. This loss of charge density impairs the glycocalyx’s role as a mechanotransducer. Under normal physiological conditions, the eGC senses longitudinal shear stress and triggers the enzymatic production of Nitric Oxide (NO) via endothelial nitric oxide synthase (eNOS). When the eGC is thinned, as observed in the sedentary UK demographic, this mechanotransduction fails, leading to chronic vasoconstriction and pro-inflammatory signalling.
Furthermore, INNERSTANDIN points to the critical role of the eGC as a physical exclusion zone. In a healthy British adult, this 0.5–3.0 μm layer prevents the direct adhesion of leucocytes and platelets to the endothelial surface. However, elevated levels of C-reactive protein (CRP) and TNF-alpha—common biomarkers in the UK’s ageing and obese populations—activate matrix metalloproteinases (MMPs) and heparanase. These enzymes cleave the structural proteins, such as Syndecan-1, into the plasma. This shedding transforms the vascular wall from a non-thrombogenic surface into a highly adhesive "velcro" for inflammatory cells, facilitating the transmigration of monocytes into the sub-endothelial space. Consequently, the eGC is the primary line of defence that, once breached, renders standard lipid management protocols secondary to the underlying structural collapse of the vascular interface. Evidence-led insights suggest that until UK clinical practice integrates glycocalyx integrity assessments, the true "ground zero" of British heart disease will remain largely unaddressed.
Protective Measures and Recovery Protocols
To fortify and resuscitate the endothelial glycocalyx (EG) requires a shift from superficial symptom management to a rigorous, mechanistically-focused protocol aimed at restoring the structural integrity of the carbohydrate-rich pericellular matrix. At the core of INNERSTANDIN biological philosophy is the recognition that the EG is not a static film, but a dynamic, self-assembling hydrogel. Restoration protocols must therefore address the dual necessity of inhibiting enzymatic degradation while providing the molecular precursors required for de novo synthesis of its primary constituents: proteoglycans, glycosaminoglycans (GAGs), and adsorbed plasma proteins.
Pharmacological and nutraceutical interventions prioritising the inhibition of heparanase—the sole mammalian endoglucuronidase capable of cleaving heparan sulphate side chains—are paramount. Research published in *The Lancet* and various *British Journal of Pharmacology* studies indicates that shedding of the EG, marked by elevated plasma concentrations of syndecan-1 and hyaluronan, is a hallmark of systemic inflammatory states and hyperglycaemia. To counteract this, recovery protocols should incorporate specific rhamnan sulphates (derived from specialised chlorophyta like *Monostroma nitidum*), which have demonstrated a unique capacity to mimic the EG’s charge-density and structurally reinforce the endothelial surface layer. Furthermore, the administration of exogenous precursors, specifically high-molecular-weight hyaluronan and glucosamine, provides the necessary substrate for hyaluronan synthases (HAS) to rebuild the GAG scaffold, thereby restoring the layer's exclusion properties against low-density lipoproteins (LDL) and leucocyte adhesion.
Beyond chemical supplementation, the role of fluid shear stress as a mechanotransduction stimulus cannot be overstated. Laminar blood flow, induced by structured aerobic exercise, stimulates the endothelial cells to increase the production of nitric oxide (NO) and superoxide dismutase, which protect the glycocalyx from oxidative attrition. Conversely, turbulent flow—common at arterial bifurcations—exacerbates shedding. Therefore, recovery protocols must emphasise consistent, moderate-intensity cardiovascular activity to maintain the "flow-induced" synthesis of the glycocalyx.
Crucially, the stabilisation of the EG is dependent on the presence of plasma albumin. Albumin does not merely circulate; it is a structural component of the glycocalyx, binding to the GAG side chains to maintain the oncotic pressure and physical barrier function of the vessel wall. In the UK context, clinical observations suggest that maintaining optimal serum albumin levels through high-quality bioavailable protein intake and systemic inflammation reduction is vital for preventing EG collapse.
Ultimately, protecting this fragile boundary requires a rejection of the reductionist "cholesterol-only" model. True vascular resilience, as championed by INNERSTANDIN, involves a multi-modal approach: neutralising MMPs (matrix metalloproteinases), replenishing the sulphated GAG pool, and leveraging physiological shear stress to ensure the heart’s primary shield remains impenetrable. Failure to address the glycocalyx in cardiovascular recovery is to ignore the very foundation of vascular health.
Summary: Key Takeaways
The endothelial glycocalyx (eGC) is not merely a passive lining but a sophisticated, carbohydrate-rich molecular sieve that governs vascular homeostasis with absolute precision. Peer-reviewed data from *The Lancet* and *Nature Reviews Cardiology* confirm that this gel-like layer, composed of syndecans, glypicans, and glycosaminoglycans like hyaluronan, serves as the primary transducer of mechanical shear stress into biochemical signals. By facilitating the activation of endothelial nitric oxide synthase (eNOS), the eGC ensures adequate nitric oxide bioavailability, preventing vasospasm and maintaining systemic perfusion. At INNERSTANDIN, our synthesis of the evidence reveals that eGC degradation—facilitated by enzymes such as heparanase and hyaluronidase—is the foundational event in atherogenesis, predating visible plaque formation. This "shedding" of the glycocalyx, often triggered by hyperglycaemia or oxidative stress, increases vascular permeability and allows for the sub-endothelial infiltration of low-density lipoproteins (LDL) and leucocytes. In the UK, where cardiovascular morbidity remains a critical public health challenge, understanding that the eGC is the ultimate gatekeeper of the microcirculation is essential. Its structural integrity is the non-negotiable prerequisite for protecting the heart against the systemic insults of modern metabolic dysfunction. Loss of this barrier translates directly to endothelial dysfunction, microvascular leakage, and accelerated hypertensive remodelling.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
The endothelial glycocalyx acts as a vital mechanosensor that regulates nitric oxide production and maintains vascular tone in response to hemodynamic forces.
Deterioration of the glycocalyx layer increases vascular permeability and facilitates the adhesion of leukocytes and platelets to the endothelium.
A healthy glycocalyx serves as a physical barrier that prevents inappropriate immune cell activation and protects the vascular wall from inflammatory damage.
Cell surface heparan sulfate proteoglycans within the glycocalyx function as essential co-receptors for growth factors that regulate endothelial cell survival.
Air pollution-induced oxidative stress leads to the shedding of glycocalyx components, which impairs microvascular function and increases the risk of cardiovascular events.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The Endothelial Glycocalyx: Your Heart's First Line of Defence"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Cardiovascular Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper