Epigenetic Markers of Pain: How Trauma is Transmitted Through Generations
Emerging science shows that chronic pain sensitivity can be inherited through epigenetic modifications. This intergenerational transmission challenges the view of pain as a purely individual experience.
Overview
The traditional medical paradigm has long viewed chronic pain through a narrow, mechanistic lens. For decades, the prevailing wisdom suggested that pain was either the result of direct tissue damage—a "broken wire" in the nervous system—or a purely psychological phenomenon residing within the patient's immediate history. However, as we delve deeper into the frontier of molecular biology, this reductionist view is being systematically dismantled. We are discovering that pain is not merely an isolated event occurring in the present; it is a biological echo of the past.
Epigenetics—the study of changes in organisms caused by modification of gene expression rather than alteration of the genetic code itself—has revealed a startling truth: the suffering of our ancestors is etched into our very DNA. This "molecular memory" means that the trauma, starvation, or chronic stress experienced by a grandparent can predispose a grandchild to heightened pain sensitivity, inflammatory disorders, and a lowered threshold for physical agony. We are essentially born with a "pain thermostat" that has been pre-set by the environmental exposures of previous generations.
At INNERSTANDING, we recognise that the global epidemic of chronic pain cannot be solved by simply suppressing symptoms with analgesics. We must understand the transgenerational transmission of these markers. When a patient presents with "idiopathic" pain—pain with no clear physical cause—the cause is often not missing; it is simply hidden in the epigenetic software that manages how their genes are read. This article serves as an exhaustive exploration of how trauma is codified, transmitted, and expressed as physical pain across the generational divide, challenging the mainstream narrative that ignores our ancestral biological debt.
##
The Biology — How It Works
To understand epigenetic markers of pain, one must first distinguish between the genetic "hardware" and the epigenetic "software." Your DNA sequence is the fixed blueprint, relatively stable throughout your life and inherited in a Mendelian fashion. The epigenome, however, consists of chemical compounds and proteins that can attach to DNA and direct such actions as turning genes on or off, or controlling the production of proteins in particular cells.
The Methylation Landscape
The most well-studied epigenetic mechanism is DNA methylation. This process involves the attachment of a methyl group ($CH_3$) to the DNA molecule, typically at specific sites known as CpG islands. When a gene is heavily methylated, it is effectively "silenced"—the cellular machinery cannot read the instructions within. In the context of pain, trauma triggers specific methylation patterns in genes responsible for the stress response and pain modulation. For example, the methylation of the promoter region of the NR3C1 gene (which encodes the glucocorticoid receptor) can lead to a permanently dysregulated HPA axis, ensuring the body remains in a state of high-alert and high-pain-sensitivity.
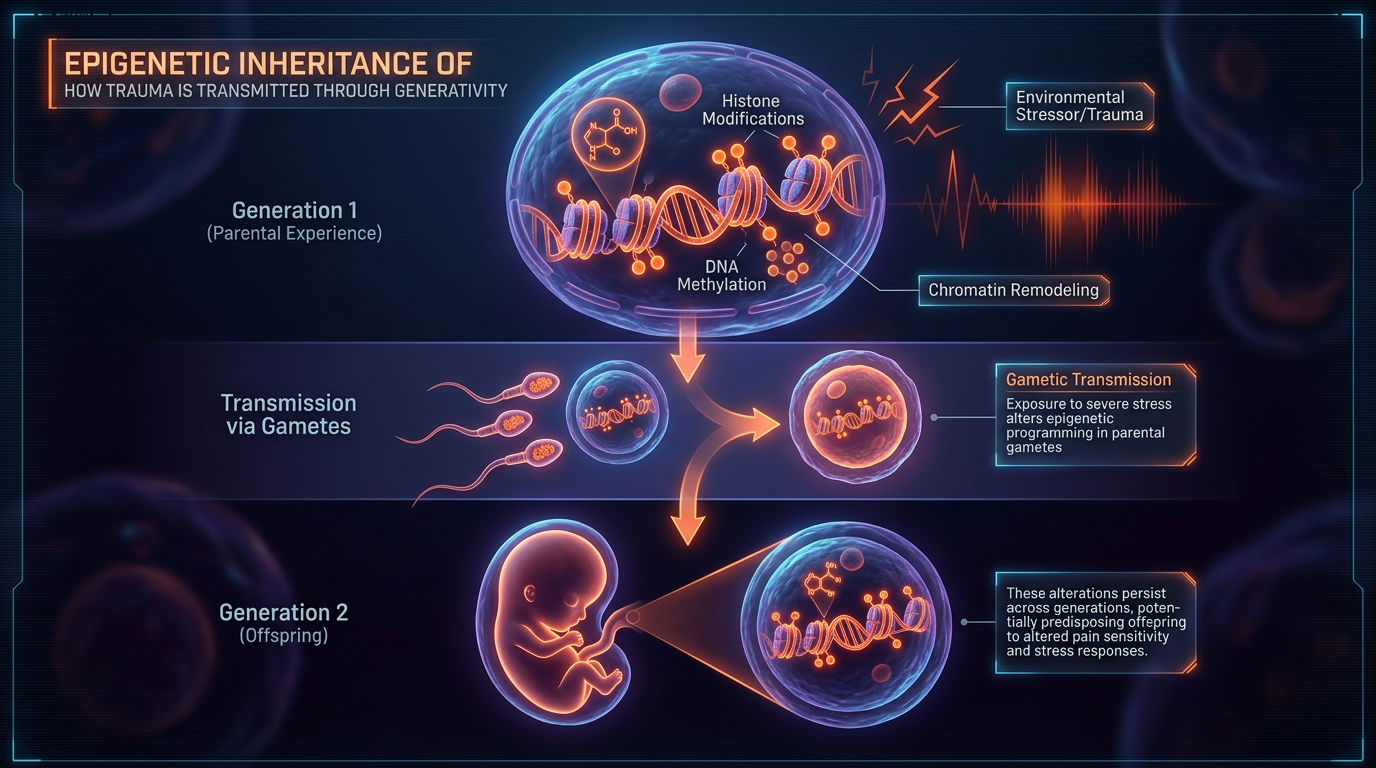
Histone Modification and Chromatin Architecture
DNA does not float freely in the nucleus; it is wrapped around proteins called histones. If the DNA is wrapped tightly (heterochromatin), the genes are inaccessible. If it is wrapped loosely (euchromatin), the genes can be expressed. Environmental trauma induces chemical changes—such as acetylation or phosphorylation—to these histone tails. These changes act as a molecular "scaffolding" that remembers the stress of the environment. If a parent suffers through a period of prolonged fear or physical trauma, the histone modifications in their germ cells (sperm or eggs) can be passed down, ensuring the offspring’s DNA is "pre-wrapped" in a way that favours a heightened defensive state.
Non-coding RNA (ncRNA)
Beyond methylation and histones lies the world of non-coding RNAs, specifically microRNAs (miRNAs). These molecules do not code for proteins but act as "silencers" of messenger RNA. Research has shown that traumatic experiences alter the profile of miRNAs in the blood and sperm. These molecules can travel to the developing embryo and influence the neurodevelopment of the pain pathways, effectively "programming" the foetal brain to be hypersensitive to noxious stimuli before the child is even born.
UK FACT: According to recent health surveys, approximately 28 million adults in the United Kingdom—roughly 43% of the population—live with some form of chronic pain. A significant portion of these cases lack a definitive structural diagnosis, suggesting a deep-seated epigenetic or neurological origin.
##
Mechanisms at the Cellular Level
The transmission of pain sensitivity occurs through a complex feedback loop involving the nervous, endocrine, and immune systems. When we speak of "inherited trauma," we are specifically looking at the recalibration of the HPA (Hypothalamic-Pituitary-Adrenal) axis.
The Glucocorticoid Receptor (GR) Malfunction
The GR is the master regulator of the stress response. In a healthy individual, cortisol (the stress hormone) binds to the GR, sending a signal to "turn off" the stress response once the threat has passed. In individuals with inherited epigenetic markers of trauma, the GR gene is often hyper-methylated. This results in fewer receptors being produced. With fewer receptors, the "off switch" fails to work. The body is flooded with cortisol, but the brain thinks it is still under threat. This chronic "high-alert" state lowers the threshold of the nociceptors (pain-sensing nerves), causing them to fire even in response to light pressure or normal movement—a condition known as allodynia.
The Role of FKBP5
A critical player in this mechanism is the FKBP5 gene. This gene acts as a "brake" on the glucocorticoid receptor. Certain epigenetic modifications to FKBP5, triggered by early-life or ancestral trauma, cause the gene to be over-expressed. This further impairs the body's ability to recover from stress. Research into survivors of major catastrophes and their descendants has shown that those with specific FKBP5 epigenetic signatures are significantly more likely to develop Post-Traumatic Stress Disorder (PTSD) and chronic widespread pain (fibromyalgia) following even minor subsequent injuries.
Microglial Priming
Inside the spinal cord and brain, immune cells called microglia act as the guardians of the central nervous system. Epigenetic markers can "prime" these cells. A primed microglial cell is like a soldier with a hair-trigger; it is overly sensitive to any signal of injury. When these cells are activated, they release pro-inflammatory cytokines like IL-1β and TNF-α. These chemicals bathe the neurons in a toxic "inflammatory soup," sustaining a state of central sensitisation. This is why many people with inherited trauma feel "inflamed" and "achy" throughout their entire bodies, regardless of their physical activity levels.
##
Environmental Threats and Biological Disruptors
The epigenome is not just influenced by psychological trauma; it is a sensitive sensor for all environmental threats. The "transmission" of pain markers is often an adaptive (though ultimately maladaptive) response to perceived environmental instability.
Preconception Paternal Stress
One of the most radical shifts in pain science is the recognition of the father's role. It was previously thought that the "resetting" of the epigenome during sperm production erased all environmental signatures. We now know this is incorrect. Paternal stress, high-fat diets, or exposure to toxins can alter the small RNA payload of the sperm. In animal models, the offspring of stressed fathers show increased sensitivity to heat and pressure, even if they were never exposed to the stressor themselves.
The "Dutch Hunger Winter" and Nutritional Epigenetics
Historical data, such as the studies on the Dutch Hunger Winter of 1944-1945, provide human evidence. Children and grandchildren of women who suffered famine during pregnancy were found to have distinct methylation patterns on the IGF2 gene. These individuals didn't just have metabolic issues; they showed a higher prevalence of chronic inflammatory conditions and reports of physical discomfort. This demonstrates that nutritional trauma—the literal lack of resources—is encoded as a biological warning to future generations to "brace" for a harsh world, often through heightened sensory awareness (pain).
Chemical Insults and Endocrine Disruptors
Modern life in the UK and other industrialised nations introduces a barrage of endocrine-disrupting chemicals (EDCs) found in plastics, pesticides, and fire retardants. These chemicals can mimic hormones and interfere with the epigenetic programming of the germline. When combined with the "psychological" trauma of modern socio-economic instability, these chemical insults create a "double hit" on the epigenome, locking the next generation into a physiological state of high-frequency pain signalling.
- —Bisphenol A (BPA): Known to alter DNA methylation in the brain regions responsible for pain processing.
- —Air Pollution (Particulate Matter): Linked to systemic inflammation that can be "remembered" by the epigenetic machinery.
- —Ultra-processed Foods: Induce oxidative stress that damages the histone architecture.
##
The Cascade: From Exposure to Disease
How does a historical event become a present-day diagnosis of chronic back pain or CRPS (Complex Regional Pain Syndrome)? The process is a cascading failure of the body’s homeostatic mechanisms.
- —The Ancestral Exposure: A grandparent survives a war, a period of severe poverty, or prolonged abuse. Their body undergoes massive epigenetic shifting to survive the high-cortisol environment.
- —Germline Transmission: These markers—specifically DNA methylation on stress-regulatory genes—are not fully erased during meiosis. They are passed to the next generation.
- —The Vulnerable Phenotype: The grandchild is born with a "sensitised" nervous system. They do not necessarily have pain yet, but their HPA axis is "brittle" and their microglia are "primed."
- —The "Second Hit": The individual experiences a relatively minor trauma—a car accident, a viral infection, or a period of work-related stress.
- —The Maladaptive Response: While a "normal" individual would heal, the epigenetically primed individual enters a spiral. Their "off switch" (GR) fails to work. The inflammation doesn't subside. The brain begins to map this "threat" as permanent physical pain.
- —Chronic Consolidation: Through the process of Long-Term Potentiation (LTP), the pain pathways in the spinal cord become "hard-wired." The epigenetic markers have now created a self-sustaining loop of physical suffering.
ALARMING STATISTIC: Research indicates that children whose parents suffer from chronic pain are up to 4 times more likely to develop chronic pain themselves by adulthood, even when controlling for shared environmental factors and direct physical injuries.
##
What the Mainstream Narrative Omits
The current medical-industrial complex is largely built on the Acute Care Model. This model is excellent for fixing broken legs or removing gallbladders, but it is woefully inadequate for treating epigenetic legacies.
The Pharmaceutical Blind Spot
The "Standard of Care" for chronic pain usually involves NSAIDs, gabapentinoids, or, in extreme cases, opioids. None of these medications address the underlying epigenetic dysregulation. They are purely "downstream" interventions. By focusing solely on blocking receptors or inhibiting enzymes, the mainstream narrative ignores the "upstream" cause: the fact that the gene expression itself is skewed. Furthermore, the pharmaceutical industry has little incentive to fund research into "epigenetic resetting" through lifestyle or environmental changes, as these cannot be easily patented.
The Myth of "Purely Genetic" Disorders
Mainstream genetics often searches for a "pain gene"—a single mutation that explains why someone suffers. This search is largely a fool's errand. Pain sensitivity is polygenic and epigenetic. By framing pain as either "genetic" (unchangeable) or "psychological" (all in your head), the medical establishment gaslights millions of patients. They omit the fact that the environment can change the expression of the genes, meaning that chronic pain is a functional state of the genome, not an inevitable destiny.
The Socio-Economic Silence
There is a profound silence regarding how the UK's "class" history and industrial past contribute to today's pain statistics. Epigenetics shows us that the "structural violence" of poverty, poor housing, and lack of agency is biologically corrosive. The mainstream narrative prefers to blame the "lifestyle choices" of the individual (diet, exercise) rather than acknowledging the intergenerational biological tax imposed by centuries of socio-economic inequality.
##
The UK Context
The United Kingdom presents a unique "living laboratory" for studying the epigenetic markers of pain. Our history—marked by the Industrial Revolution, two World Wars, and the rapid decline of mining and manufacturing communities—has left a deep biological imprint on the population.
The "Glasgow Effect" and Beyond
In many parts of the UK, particularly in Glasgow and the de-industrialised North of England, health outcomes are significantly worse than in other areas with similar levels of deprivation. This has been dubbed the "Glasgow Effect." While many factors contribute, biological researchers are increasingly looking at transgenerational epigenetic "weathering." The stress of the "Thatcher era" and the collapse of the coal industry didn't just affect bank balances; it changed the methylation patterns of the children born in those communities. This has manifested as a "pain epidemic" in the current generation, who suffer from disproportionately high rates of fibromyalgia and chronic fatigue syndrome (ME/CFS).
The NHS Burden
The NHS is currently buckling under the weight of "medically unexplained symptoms" (MUS). A vast number of these cases are, in fact, the physical manifestation of inherited and accumulated trauma. Because the NHS is structured around 10-minute consultations and siloed departments (cardiology, neurology, etc.), it is incapable of seeing the "whole-body" epigenetic picture. The UK's reliance on "prescribing our way out" of the problem has led to an opioid crisis that, while not as severe as that in the US, is a significant public health threat.
- —Opioid Prescriptions: In the UK, opioid prescriptions have increased significantly over the last two decades, despite evidence that they are largely ineffective for the "epigenetic" pain caused by central sensitisation.
- —Mental Health Integration: The UK still largely separates "Mental Health" (trauma) from "Physical Health" (pain), failing to realise they are two sides of the same epigenetic coin.
##
Protective Measures and Recovery Protocols
If the "markers of pain" are written into our software, the question becomes: can we rewrite the code? The answer, according to the emerging field of epigenetic editing and neuroplasticity, is a resounding yes. The epigenome is plastic; it is designed to be responsive to the environment.
1. Vagus Nerve Stimulation (VNS) and Parasympathetic Priming
The vagus nerve is the primary conduit for the "rest and digest" system. Chronic pain is a state of "sympathetic dominance." Techniques that stimulate the vagus nerve—deep diaphragmatic breathing, cold water immersion, and specific humming exercises—send a signal to the brain that the "war is over." Over time, this consistent signal can lead to de-methylation of the stress-response genes, effectively "turning down" the pain thermostat.
2. Nutritional Epigenetic Modulators (Methyl Donors)
The process of DNA methylation requires "methyl donors" from our diet. Deficiencies in B-vitamins (B12, Folate), Choline, and Betaine can impair the body's ability to properly regulate gene expression.
- —Sulforaphane (found in broccoli sprouts): A potent histone deacetylase (HDAC) inhibitor, which can help "unlock" genes that suppress inflammation.
- —Omega-3 Fatty Acids: Essential for restoring the integrity of the neuronal membranes and dampening microglial priming.
- —Curcumin: Known to influence DNA methyltransferase activity, helping to reset the pro-inflammatory markers inherited from trauma.
3. Somatic Experiencing and EMDR
Since the trauma is stored in the body's "biological memory," traditional talk therapy is often insufficient. Somatic Experiencing (SE) and Eye Movement Desensitisation and Reprocessing (EMDR) work by accessing the subcortical regions of the brain where the epigenetic signatures of "threat" are most active. By processing the "stuck" energy of trauma, patients can literally change their gene expression. Studies have shown that successful trauma therapy results in measurable changes in the methylation of the FKBP5 gene.
4. Environmental Triage
Recovery requires the removal of the "ongoing threat." This means:
- —Reducing "Blue Light" Exposure: Chronic exposure to artificial light at night dysregulates circadian rhythms, which are tightly linked to the epigenetic clock and pain sensitivity.
- —Eliminating EDCs: Switching to glass, avoiding "fragrance," and eating organic where possible to reduce the chemical "noise" that interferes with epigenetic signalling.
- —Community and Belonging: High-quality social connection is one of the most powerful "epigenetic buffers." The presence of a "safe tribe" signals to the genes that the environment is secure, allowing the defensive pain markers to recede.
##
Summary: Key Takeaways
The science of epigenetics has forever changed our understanding of chronic pain. It has moved us from a world where pain is an "accident" to a world where pain is a "legacy."
- —Pain is Transgenerational: The experiences of your ancestors—their trauma, their hunger, and their stress—have physically modified your DNA expression. You are born with a "biological predisposition" to how you perceive pain.
- —The Epigenome is the Key: DNA methylation, histone modification, and non-coding RNAs are the physical mechanisms that store and transmit "pain memories."
- —The HPA Axis is the Ground Zero: Inherited trauma manifests as a dysregulated stress response, leading to "primed" immune cells in the brain and a lowered threshold for physical pain.
- —The UK Faces a Unique Crisis: De-industrialisation and historical social stress have created a "biological debt" that is manifesting as the current chronic pain epidemic.
- —Healing is Possible: Because the epigenome is plastic, it can be "re-programmed" through targeted nutritional, physical, and psychological interventions. We are not "stuck" with our ancestral markers; we have the power to rewrite our biological future.
The medical establishment may continue to offer pills for a problem that is written in our genes, but the "Truth-Exposing" reality is that healing from chronic pain requires an ancestral audit. We must address the "ghosts" in our biology if we are to truly find relief. Chronic pain is not your fault, but understanding its epigenetic roots is your greatest tool for recovery.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Epigenetic Markers of Pain: How Trauma is Transmitted Through Generations"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper