Genetic Polymorphisms in UK Lipid Metabolism
Variations in genes like APOE and PCSK9 dictate how different individuals respond to dietary fats. Understanding your genetic blueprint is essential for personalized lipid management in the UK.
# Genetic Polymorphisms in UK Lipid Metabolism: The Hidden Blueprint of Cardiovascular Destiny
Overview
For decades, the United Kingdom’s public health apparatus has operated under the reductionist "Lipid Hypothesis"—the notion that dietary cholesterol and saturated fat are the primary drivers of cardiovascular disease (CVD). However, as we stand at the precipice of a revolution in Precision Medicine, this "one-size-fits-all" approach is being exposed as fundamentally flawed. The reality is far more complex and is etched into our very DNA.
The variation in how British citizens process dietary lipids is dictated by Genetic Polymorphisms—minor variations in our DNA sequence that alter the function of enzymes, receptors, and transport proteins. While one individual may thrive on a traditional high-fat ancestral diet, another may find their arteries rapidly occluded by the same nutritional profile. This article delves into the clandestine world of Nutrigenomics, specifically focusing on how the British genepool—a unique mosaic of Anglo-Saxon, Celtic, and Viking lineages—interacts with modern lipid challenges.
Understanding your genetic blueprint is no longer an elective luxury; it is a biological necessity. In the UK, where cardiovascular disease remains a leading cause of mortality, the failure to account for polymorphisms such as APOE, PCSK9, and SLCO1B1 is a systemic oversight that costs thousands of lives annually. We are not merely what we eat; we are what our genes *do* with what we eat.
The Biology — How It Works
To understand genetic polymorphisms, one must first master the basics of the Lipid Transport System. Cholesterol is not a "poison" but a vital structural component of every cell membrane and a precursor to essential hormones (oestrogen, testosterone, cortisol) and Vitamin D. Because lipids are hydrophobic (water-fearing), they cannot travel freely in the blood. They must be packaged into spherical vehicles called Lipoproteins.
The Lipoprotein Hierarchy
Lipoproteins are categorised by their density, which is determined by the ratio of protein to lipid:
- —Chylomicrons: Transport dietary fats from the intestines.
- —VLDL (Very-Low-Density Lipoprotein): Created by the liver to distribute triglycerides.
- —LDL (Low-Density Lipoprotein): Often maligned as "bad" cholesterol, its primary role is delivering cholesterol to cells.
- —HDL (High-Density Lipoprotein): Responsible for Reverse Cholesterol Transport, picking up excess cholesterol and returning it to the liver.
The Role of Polymorphisms
A Single Nucleotide Polymorphism (SNP) is a variation at a single position in a DNA sequence. In the context of lipid metabolism, these SNPs can change the "shape" of a receptor or the "speed" of an enzyme.
Fact: Approximately 1 in 250 people in the UK carry a mutation for Familial Hypercholesterolaemia (FH), yet the vast majority remain undiagnosed until a major cardiac event occurs.
The most significant player in this landscape is the Apolipoprotein E (APOE) gene. Located on chromosome 19, APOE provides the instructions for making a protein that combines with fats to form lipoproteins. There are three common alleles (variants) in the British population: ε2, ε3, and ε4.
- —ε3 is considered the "neutral" baseline.
- —ε4 is associated with higher LDL levels and increased risk of Alzheimer’s disease.
- —ε2 is associated with lower LDL but a higher risk of Type III Hyperlipoproteinaemia.
Mechanisms at the Cellular Level
The interplay between genes and lipids occurs primarily at the surface of the Hepatocyte (liver cell) and within the Endothelium (the lining of the blood vessels).
The LDL Receptor (LDLR) Pathway
The LDLR is the "gatekeeper." It sits on the surface of cells and pulls LDL particles out of circulation. In individuals with high-functioning LDLR genes, LDL is cleared efficiently. However, polymorphisms in the PCSK9 gene can sabotage this process.
PCSK9 (Proprotein Convertase Subtilisin/Kexin Type 9) is an enzyme that binds to the LDL receptor and marks it for degradation.
- —Gain-of-function mutations in PCSK9 lead to fewer receptors, causing LDL levels to skyrocket.
- —Loss-of-function mutations result in a surplus of receptors, leading to naturally very low LDL levels and "super-immunity" to heart disease.
The SREBP Pathway and Feedback Loops
Inside the cell, the Sterol Regulatory Element-Binding Protein (SREBP) pathway acts as a thermostat. When cellular cholesterol is low, SREBP migrates to the nucleus to trigger the production of more LDLRs and HMG-CoA Reductase (the enzyme that produces cholesterol). Genetic variations can "break" this thermostat, causing the liver to overproduce cholesterol even when the blood is already saturated with it.
APOE and the Blood-Brain Barrier
The APOE4 variant is particularly treacherous because its mechanism extends beyond the liver. In the brain, APOE4 is less efficient at transporting essential omega-3 fatty acids (like DHA) across the blood-brain barrier. This leads to increased neuro-inflammation and the accumulation of amyloid-beta plaques. For a British citizen carrying the ε4 allele, a high-carbohydrate, high-processed-fat diet is not just a risk for the heart; it is a direct assault on the brain.
Environmental Threats and Biological Disruptors
The British environment has become a "perfect storm" for those with lipid-sensitive genotypes. Our biology, evolved over millennia in a nutrient-sparse environment, is now bombarded by Xenobiotics and industrial food by-products.
The Seed Oil Catastrophe
The UK food supply is inundated with Industrial Seed Oils (sunflower, rapeseed, corn). These oils are high in Linoleic Acid, an omega-6 fatty acid that is highly susceptible to oxidation. When individuals with certain PON1 (Paraoxonase 1) polymorphisms—which govern the antioxidant capacity of HDL—consume these oils, their LDL particles become oxidised (Ox-LDL).
Callout: Oxidised LDL is significantly more atherogenic than standard LDL; it is the "damaged cargo" that the immune system perceives as a foreign invader.
Endocrine Disruptors and Lipid Signalling
Chemicals found in UK tap water and plastic packaging, such as Bisphenol A (BPA) and Phthalates, interfere with PPAR (Peroxisome Proliferator-Activated Receptors). These receptors are the master regulators of lipid metabolism. For someone with a polymorphism in the PPAR-gamma gene, exposure to these environmental toxins can trigger rapid weight gain and systemic insulin resistance, further derailing lipid profiles.
The "Ultra-Processed" UK Diet
The UK consumes more ultra-processed food (UPF) than any other nation in Europe. UPFs are designed to bypass the body's natural satiety signals. For those with polymorphisms in the FTO (Fat Mass and Obesity-Associated) gene, the high-palatability of these foods leads to a hyper-insulinemic state. Insulin is a powerful activator of HMG-CoA Reductase; thus, high sugar intake in the UK is a more direct driver of high cholesterol than dietary fat for a large segment of the population.
The Cascade: From Exposure to Disease
The journey from a genetic SNP to a myocardial infarction (heart attack) is a multi-stage cascade of biological failure.
- —Stage One: Genetic Susceptibility. The individual inherits a variant like APOB-100, which makes their LDL particles smaller and denser (Pattern B).
- —Stage Two: Environmental Trigger. The individual consumes the standard UK diet (high in refined flour and vegetable oils) and lives a sedentary lifestyle in a polluted urban centre like London or Manchester.
- —Stage Three: Lipid Oxidation. Due to a lack of dietary antioxidants and a genetic deficiency in the GSHPx (Glutathione Peroxidase) enzyme, the LDL particles oxidize.
- —Stage Four: Endothelial Injury. The Ox-LDL penetrates the endothelial wall. The immune system sends Macrophages to engulf the "damaged" lipids.
- —Stage Five: Foam Cell Formation. The macrophages become bloated with fat, turning into "Foam Cells." These cells die and form a necrotic core—the basis of an Atherosclerotic Plaque.
- —Stage Six: Plaque Rupture. Chronic inflammation, often exacerbated by a high Omega-6 to Omega-3 ratio, destabilizes the plaque. It ruptures, a clot forms, and blood flow is blocked.
Statistic: In the UK, someone is admitted to a hospital with a heart attack every five minutes. A significant percentage of these individuals have "normal" cholesterol levels but highly abnormal Lipoprotein Subfractions that were never tested.
What the Mainstream Narrative Omits
The current medical orthodoxy in the UK, largely driven by NICE (National Institute for Health and Care Excellence) guidelines, focuses almost exclusively on LDL-C (LDL Cholesterol). This is a volumetric measurement—it tells you how much cholesterol is in the "boats," but not how many "boats" there are or what condition they are in.
The Statin Monopoly
The mainstream narrative pushes Statins (HMG-CoA Reductase inhibitors) as a universal solution. While statins are life-saving for some, they are often prescribed without checking the SLCO1B1 genotype. This gene controls how the liver takes up statins.
- —Individuals with the C allele of SLCO1B1 have a much higher risk of Statin-Induced Myopathy (muscle pain and damage).
- —In the UK, millions are prescribed statins without this £30 genetic test, leading to widespread "unexplained" fatigue and muscle wasting.
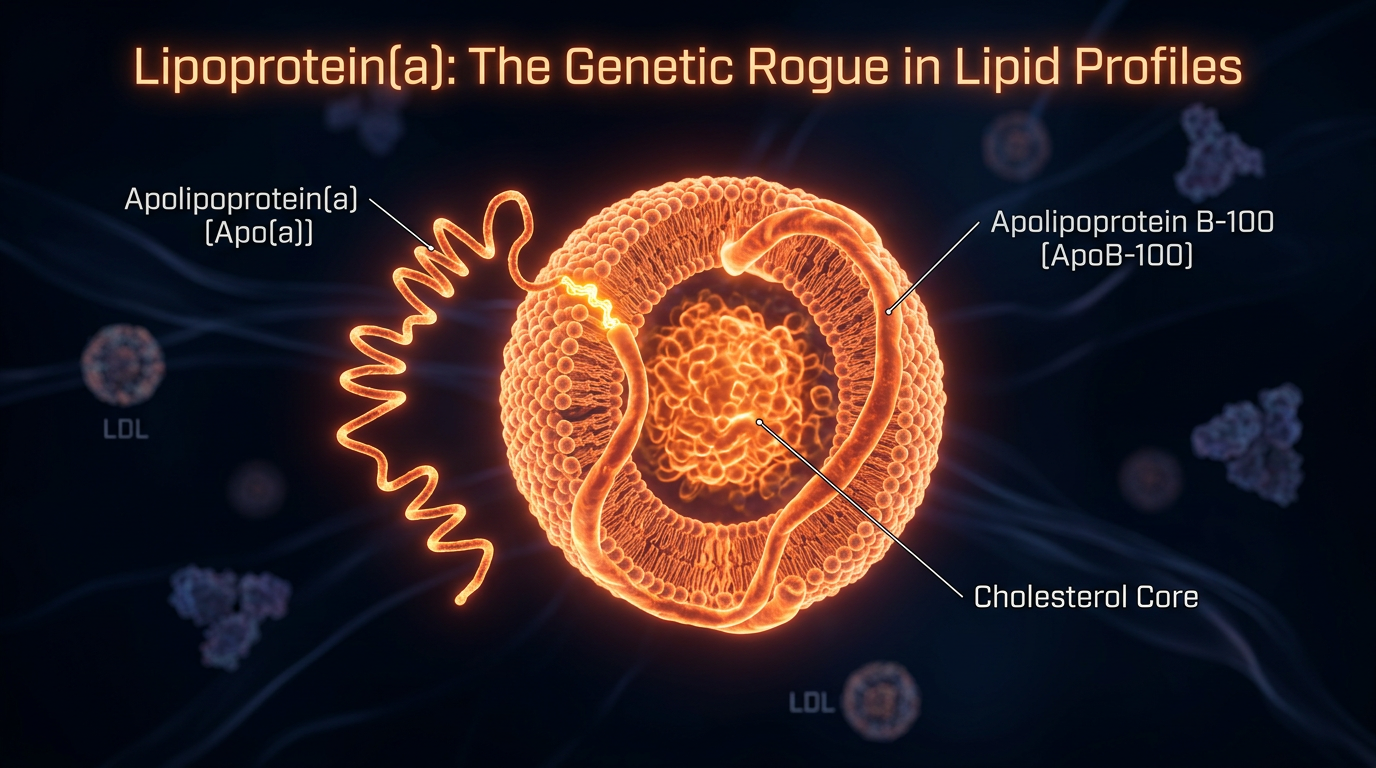
The Lipoprotein(a) Silence
Perhaps the most egregious omission is the failure to routinely test for Lipoprotein(a), or Lp(a). This is a highly inflammatory, genetically determined particle that acts like "sticky tape" on the artery walls.
- —Lp(a) levels are 90% determined by genetics and are largely unaffected by diet or statins.
- —Despite its massive role in "premature" heart attacks in the UK, it is rarely part of a standard NHS lipid panel.
The APOE4/Saturated Fat Conflict
The mainstream often advises everyone to lower saturated fat. However, for APOE4 carriers, saturated fat significantly increases LDL levels. Conversely, for APOE2 carriers, saturated fat may have a negligible effect, but they are highly sensitive to simple carbohydrates. By giving the same advice to both, the "experts" are inadvertently harming 25% of the population.
The UK Context
The UK presents a unique case study in lipid genetics due to its history of migrations and the "Founder Effect" in certain regions.
The Celtic Fringe and Iron Overload
In Scotland, Wales, and Northern Ireland, there is a higher prevalence of Hereditary Haemochromatosis (HFE gene mutations). Excess iron is a potent pro-oxidant. When combined with typical British lipid polymorphisms, this high iron load acts as a catalyst, accelerating the oxidation of LDL and the progression of heart disease.
Postcode Lottery of Diagnostics
Access to advanced lipid testing—such as Apolipoprotein B (ApoB) or LDL Particle Number (LDL-P)—is currently a postcode lottery in the UK. While private clinics in Harley Street offer comprehensive nutrigenomic panels, the average NHS patient in a deprived area of the North East is stuck with a 1970s-era "Total Cholesterol" test.
The Vitamin D Deficiency Factor
The UK’s lack of sunlight creates a chronic Vitamin D deficiency. Vitamin D is synthesized from cholesterol and plays a role in regulating the Renin-Angiotensin System, which affects vascular health. The synergistic effect of low Vitamin D and high-risk lipid genotypes in the UK is a major contributor to the "Winter Mortality" spikes in cardiovascular events.
Protective Measures and Recovery Protocols
If you carry high-risk polymorphisms, you are not "doomed." Epigenetics teaches us that we can silence or amplify certain genes through targeted interventions.
Targeted Nutrition by Genotype
- —For APOE4 Carriers:
- —Transition to a "Mediterranean-style" diet but with a strict limit on saturated fats (butter, coconut oil).
- —Prioritise Monounsaturated Fats (Extra Virgin Olive Oil).
- —Increase intake of high-quality Omega-3s (EPA/DHA) to support cognitive function.
- —Avoid alcohol, as ε4 carriers have a reduced ability to clear the lipid-disrupting toxins produced by ethanol.
- —For APOE2 Carriers:
- —Focus on a low-glycaemic index diet.
- —Be cautious with "Low Fat" processed foods, which are usually high in sugar and will spike triglycerides in this genotype.
Precision Supplementation
- —Berberine: For those with PCSK9 gain-of-function variants, Berberine has been shown to naturally inhibit PCSK9, increasing LDL receptor density without the side effects of statins.
- —Vitamin K2 (MK-7): Essential for ensuring that calcium is deposited in the bones and not in the arterial walls (calcification). This is critical for anyone with a high Genetic Risk Score for CVD.
- —Magnesium Taurate: Supports the endothelium and helps regulate heart rhythm, particularly important for those with NOS3 (Nitric Oxide Synthase) polymorphisms.
Lifestyle Modification: The "Ancestral Reset"
- —Intermittent Fasting: This triggers Autophagy, the cellular "clean-up" process. It is particularly effective for resetting the SREBP pathway in those with metabolic syndrome.
- —Cold Exposure: The British tradition of "cold water swimming" can actually improve lipid profiles by activating Brown Adipose Tissue (BAT), which uses fatty acids for thermogenesis.
- —High-Intensity Interval Training (HIIT): Specifically targets the clearance of VLDL particles and improves insulin sensitivity more effectively than steady-state cardio for those with the ADRB2 (Adrenergic Receptor) polymorphism.
Summary: Key Takeaways
The path to cardiovascular longevity in the UK requires a departure from the "Standard British Diet" and the "Standard Medical Model."
- —Your DNA is not your destiny: Genetic polymorphisms like APOE4 or PCSK9 mutations are merely "loaded guns." Your diet, environment, and lifestyle pull the trigger.
- —Demand better testing: A "Total Cholesterol" test is insufficient. Demand ApoB, Lp(a), and Homocysteine levels to get a true picture of your risk.
- —Context is everything: Saturated fat is not a universal villain; its impact depends entirely on your specific genetic receptors.
- —Beware the mainstream omissions: The lack of routine genetic screening for SLCO1B1 before statin prescription is a failure of the current system.
- —The British environment is toxic to lipids: Between seed oils, UPFs, and Vitamin D deficiency, the UK citizen must be hyper-vigilant in protecting their metabolic health.
In the era of INNERSTANDING, we must take ownership of our biological data. The era of blind adherence to generalised guidelines is over. The era of the Genetically Informed Individual has begun. Knowledge of your lipid polymorphisms is the ultimate shield against the modern epidemic of heart disease.
*
"References for further study:"
- —*The British Heart Foundation (BHF) Genetic Research Archives*
- —*The UK Biobank Lipidomics Study*
- —*Journal of Clinical Lipidology: Nutrigenetics and the APOE Allele*
- —*Nature Genetics: PCSK9 and the Evolution of Human Lipid Regulation*
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Genetic Polymorphisms in UK Lipid Metabolism"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper