Heavy Metal Chelation: Biological Risks of Synthetic Ligands
Chelation therapy uses IV agents to strip heavy metals from the blood, but it can also deplete essential minerals. This article warns of the physiological risks involved in aggressive chelation.
Overview
In the contemporary landscape of functional medicine and the burgeoning "biohacking" movement, chelation therapy has ascended from a niche toxicology treatment to a mainstream wellness intervention. Marketed as the ultimate "system reset" for the modern, polluted human, intravenous (IV) chelation promises to strip the body of industrial toxins, heavy metals, and arterial plaque. However, beneath the polished aesthetic of boutique IV lounges lies a complex and potentially perilous biochemical reality.
As a senior researcher at INNERSTANDING, it is my responsibility to look beyond the marketing collateral of "detoxification" and examine the raw molecular interactions of synthetic ligands. Chelation—derived from the Greek word *chele*, meaning "claw"—is a process whereby a chemical compound (the ligand) binds to a central metal atom, forming a ring-like structure known as a coordination complex. While this mechanism is a cornerstone of emergency toxicology, its elective use in sub-clinical scenarios presents a profound risk-to-benefit ratio that is frequently glossed over by practitioners.
The fundamental danger of synthetic chelation lies in its non-selectivity. The "claw" does not possess an innate intelligence; it follows the laws of thermodynamics and binding affinities. In the aggressive pursuit of removing lead, mercury, or cadmium, these synthetic agents frequently strip the body of essential divalent cations—zinc, magnesium, calcium, and manganese—which are the foundational cofactors for thousands of enzymatic reactions.
This article serves as a comprehensive interrogation of the physiological risks involved in aggressive chelation. We will explore how these "synthetic claws" can disrupt cellular homeostasis, induce oxidative stress through the redistribution of metals, and potentially leave the patient more biochemically depleted than when they began.
Key Fact: While EDTA (Ethylenediaminetetraacetic acid) is often promoted for cardiovascular health, its primary industrial use is as a sequestering agent in detergents and paper manufacturing, highlighting its aggressive nature as a metal-stripper.
---
The Biology — How It Works

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus
Clean Slate is a cellular-level detoxifier that targets heavy metals, pesticides, and environmental toxins to unblock your body's natural defense pathways. It helps reduce systemic inflammation and restores the nutrient absorption sites often compromised by modern toxicity.
Vetting Notes
Pending
To understand the risks, one must first understand the chemistry of the coordination complex. A chelating agent is a polydentate ligand, meaning it has multiple "teeth" (usually oxygen or nitrogen atoms) that can donate electron pairs to a central metal ion.
The Chemistry of Ligands
When a synthetic ligand like EDTA, DMPS (2,3-Dimercapto-1-propanesulfonic acid), or DMSA (Meso-2,3-dimercaptosuccinic acid) is introduced into the bloodstream via an IV infusion, it creates a concentration gradient that pulls metals from the extracellular matrix. These ligands encircle the metal ion, neutralising its reactive charge and making it water-soluble so it can be excreted through the kidneys.
However, the Stability Constant of a ligand determines which metal it will grab first. Every ligand has a hierarchy of preference. For instance, EDTA has a notoriously high affinity for Lead (Pb), but it has an even higher affinity for Nickel and Copper, and a dangerously strong pull on Calcium and Magnesium.
The Route of Administration
In the context of IV therapy, the delivery is "bolus" or rapid-drip. This bypasses the body's natural rate-limiting barriers (the gastrointestinal tract and the liver's first-pass metabolism). By flooding the systemic circulation with high concentrations of synthetic ligands, we create a sudden "vacuum" effect in the blood.
- —EDTA: Primarily used for lead poisoning and occasionally for calcium-based arterial plaques. It is highly efficient but largely stays in the extracellular space.
- —DMPS: A potent sulphur-based chelator used for mercury and arsenic. It can penetrate deeper into tissues but carries a higher risk of acute allergic reactions.
- —DMSA: Often administered orally, but in "aggressive" protocols, it is used in tandem with IV agents to cross the blood-brain barrier—a practice fraught with neurological risk.
The biological reality is that our bodies are not designed to handle the sudden, massive mobilisation of stored elements. The "claws" do not distinguish between a toxic mercury atom and a vital zinc atom required for DNA repair.
---
Mechanisms at the Cellular Level
The disruption caused by synthetic ligands is most profound at the mitochondrial and enzymatic levels. Every cell in the human body relies on metallic cofactors to maintain the "spark of life."
Displacement and The "Hole" in the Enzyme
Enzymes are protein catalysts. Many of these proteins contain a "metal site"—a specific pocket where a mineral like zinc or magnesium must sit for the enzyme to function. When an aggressive synthetic ligand enters the cellular environment, it can pull the mineral out of the enzyme's active site.
This creates what we term "apo-enzymes"—proteins that are structurally present but functionally "dead." For example:
- —Zinc Fingers: These are structural motifs in proteins that facilitate DNA binding. If a chelator strips the zinc, the protein can no longer repair DNA, leading to increased mutation risks and cellular senescence.
- —Carbonic Anhydrase: This enzyme is crucial for acid-base balance and CO2 transport. It is zinc-dependent. Stripping this mineral can lead to systemic metabolic acidosis.
The Re-distribution Phenomenon
Perhaps the most overlooked mechanism is the Re-distribution Phenomenon. When a ligand binds a metal in the peripheral tissues (like fat or muscle) but the concentration of the ligand drops before the metal can be excreted by the kidneys, the metal is often "dropped" in a new, more sensitive location.
Statistic: Research indicates that improper chelation protocols can increase the concentration of lead in the brain by up to 25% shortly after administration, as the metal is mobilised from bone stores but fails to be fully cleared through the renal system.
Mitochondrial Toxicity
Mitochondria require a delicate balance of iron, copper, and manganese to facilitate the Electron Transport Chain (ETC). Synthetic ligands can interfere with the cytochromes in the ETC, essentially "choking" the cell's ability to produce ATP (adenosine triphosphate). This is why many patients report profound "detox fatigue"—which is often not detox at all, but acute mitochondrial suppression.
---
Environmental Threats and Biological Disruptors
To understand why people seek chelation, we must acknowledge the undeniable reality: we live in a "Toxic Soup." The Industrial Revolution has redistributed billions of tonnes of heavy metals from deep within the Earth's crust into our air, water, and soil.
The "Big Four" Threats
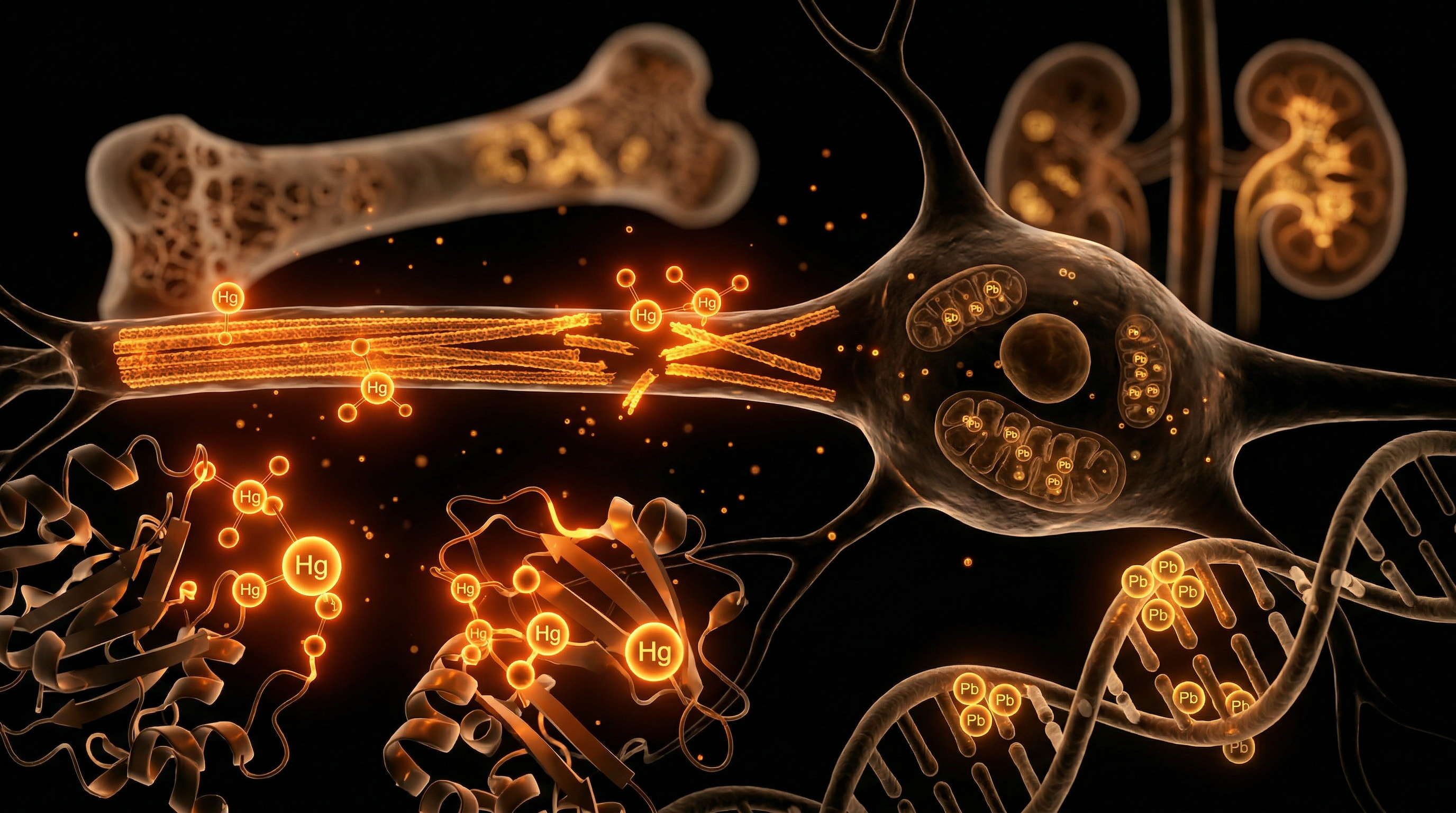
- —Mercury (Hg): Primarily from dental amalgams, large fish consumption, and industrial emissions. It is a potent neurotoxin that binds to thiol (sulphur) groups in the body, disrupting protein folding.
- —Lead (Pb): Found in old piping, aviation fuel, and legacy paint. It mimics calcium, allowing it to hide in bone tissue for decades, only to be released during menopause, pregnancy, or—dangerously—during aggressive chelation.
- —Cadmium (Cd): Linked to tobacco smoke, rechargeable batteries, and industrial fertilisers. It accumulates in the kidneys and has a half-life in the human body of up to 30 years.
- —Aluminium (Al): While technically a light metal, its ubiquity in cookware, deodorants, and vaccines has led to concerns regarding its role in neurodegenerative diseases like Alzheimer’s.
The Synergy of Toxicity
Modern science is beginning to recognise Synergistic Toxicity. The presence of mercury and lead together is significantly more toxic than the sum of their individual parts. Metals compete for the same transport proteins (such as DMT1) and the same storage sites.
When synthetic ligands are introduced into a body burdened by multiple metals, the ligands may "trade" metals. A chelator might pick up a lead atom, encounter a mercury atom for which it has a higher affinity, drop the lead, and pick up the mercury. This "shuffling" of toxins creates a state of internal chaos that the body’s natural emunctories (liver, kidneys, skin) struggle to manage.
---
The Cascade: From Exposure to Disease
The progression from heavy metal exposure to clinical disease is rarely a straight line. It is a "cascade" of falling dominoes, starting with subtle biochemical shifts and ending in systemic failure.
Phase 1: Oxidative Stress and Lipid Peroxidation
Metals like iron and copper, when displaced by synthetic ligands, can participate in the Fenton Reaction. This produces the hydroxyl radical (•OH), the most reactive and damaging free radical in biology. These radicals attack the lipid bilayer of cell membranes, a process called lipid peroxidation, which effectively "rusts" the cells from the inside out.
Phase 2: Epigenetic Dysregulation
Heavy metals are "epigenetic silencers." They can alter DNA methylation patterns, switching off protective tumour-suppressor genes. When a patient undergoes aggressive chelation, the sudden flux of these metals can trigger rapid epigenetic shifts, sometimes activating latent inflammatory pathways.
Phase 3: The Neurological Tipping Point
The brain is protected by the Blood-Brain Barrier (BBB). However, many synthetic ligands, particularly when combined with surfactants or administered in high doses, can temporarily increase the permeability of the BBB.
- —Excitotoxicity: Metals like lead and mercury can mimic or trigger the overproduction of Glutamate, the brain's primary excitatory neurotransmitter. This leads to neurons "firing to death."
- —Protein Misfolding: Metals are known to catalyse the folding of beta-amyloid plaques and tau tangles, the hallmarks of Alzheimer's disease.
Phase 4: Immune System Collapse
The immune system's "General" is the T-cell. Heavy metals disrupt T-cell signalling, often leading to a state of Autoimmunity. The body, sensing the "foreign" metal-protein complex created by a synthetic ligand, may begin to attack its own tissues. This is frequently seen in the "flare-ups" of rheumatoid arthritis or lupus following unmonitored IV "detox" sessions.
---
What the Mainstream Narrative Omits
The wellness industry presents IV chelation as a safe, routine procedure. However, the "mainstream" narrative—even within the alternative health sphere—conveniently omits several critical biological dangers.
The Mineral Stripping Crisis
The most immediate risk of synthetic ligands is the acute depletion of Magnesium and Zinc.
- —Magnesium is responsible for over 300 enzymatic reactions, including those that regulate heart rhythm. Rapid chelation of magnesium can lead to cardiac arrhythmias and, in extreme cases recorded in medical literature, sudden cardiac arrest.
- —Zinc is the primary driver of the immune system and gut integrity. Stripping zinc often leads to "leaky gut" and a profound susceptibility to viral infections post-treatment.
Renal Overload and Tubular Necrosis
The kidneys are the primary exit route for the coordination complexes formed during chelation. These complexes are often large and "sharp" at a molecular level.
Warning: Aggressive IV chelation can cause Acute Tubular Necrosis (ATN). The kidneys become overwhelmed by the sheer volume of mobilised metals, leading to temporary or permanent renal impairment. Mainstream clinics rarely perform the necessary pre-and-post-infusion creatinine and GFR (Glomerular Filtration Rate) tests to monitor this risk.
The "Bioavailability" Fallacy
Practitioners often claim that because they are providing "mineral replacements" in the IV bag, there is no risk of depletion. This is biochemically naive. A synthetic ligand in the same solution as replacement minerals will often bind to those minerals *within the IV bag* or immediately upon entering the blood, rendering both the ligand and the mineral useless. The "claw" is occupied before it can ever reach the toxic metals in the tissues.
The Profit Motive vs. Patient Safety
The cost of an IV chelation session in a London or New York clinic can range from £200 to £800. This creates a financial incentive for clinics to recommend "cycles" of 10, 20, or 30 infusions. Biological recovery, however, does not happen on a weekly billing cycle. The body requires months to safely redistribute minerals and repair the oxidative damage caused by a single aggressive chelation event.
---
The UK Context
In the United Kingdom, the landscape of chelation therapy is particularly complex due to a combination of historical environmental factors and a bifurcated healthcare system.
Post-Industrial Legacy
The UK’s history as the cradle of the Industrial Revolution has left a legacy of heavy metal contamination.
- —Lead Pipes: Despite modernisations, millions of Victorian-era homes in cities like London, Manchester, and Birmingham still have lead connecting pipes or lead soldering.
- —Thames Water and Sewage: Recent reports have highlighted the presence of heavy metals and pharmaceutical runoff in UK waterways, contributing to a baseline "body burden" that makes the UK population particularly interested in "detox" solutions.
The Regulatory Gap
In the UK, the Care Quality Commission (CQC) regulates clinics that provide "medical treatments." However, many wellness centres market IV infusions as "nutritional supplements" rather than medical chelation to circumvent strict oversight.
- —The NHS Position: The National Health Service (NHS) only provides chelation for acute, life-threatening poisoning (e.g., acute lead ingestion or iron overload from frequent blood transfusions).
- —The Private Boom: This has pushed the "worried well" into the private sector, where the lack of standardised protocols for "preventative chelation" increases the risk of the biological disruptions discussed in this article.
The "London Lifestyle" Factor
The high-stress, high-pollution environment of London leads many to seek "quick fixes." This has led to the rise of "lunchbreak chelation," where professionals receive EDTA drips without adequate prior testing of their mineral status or renal function. At INNERSTANDING, we view this trend with extreme caution. The British physiology, already burdened by "grey sky" Vitamin D deficiency, is particularly vulnerable to the mineral-stripping effects of synthetic ligands.
---
Protective Measures and Recovery Protocols
If one is to navigate the world of metal detoxification, it must be done with surgical precision and a "Biology First" mentality. The goal should be Safe Efflux, not Aggressive Stripping.
1. Metabolic Priming
Before a single drop of a synthetic ligand enters the body, the patient must undergo at least 4-6 weeks of Metabolic Priming.
- —Mineral Saturation: Optimising intracellular levels of Magnesium (using glycinate or malate forms) and Zinc.
- —Glutathione Support: Boosting the body's natural "Master Antioxidant" through precursors like N-Acetyl Cysteine (NAC) and Liposomal Glutathione. Glutathione is the body's endogenous chelator; it is far "smarter" than EDTA.
2. The Use of "Gentle" Binders
Rather than jumping to IV synthetic ligands, one should utilise gastrointestinal binders to capture metals that are naturally secreted in the bile.
- —Modified Citrus Pectin (MCP): Shown in clinical studies to increase the urinary excretion of lead and mercury without stripping essential minerals.
- —Zeolite (Clinoptilolite): A volcanic mineral with a cage-like structure that selectively traps heavy metals while leaving smaller nutrient minerals alone.
- —Chlorella: A "green" binder that is particularly effective at binding mercury in the gut, preventing "enterohepatic recirculation."
3. Liposomal Delivery over IV
Emerging research suggests that Liposomal EDTA (taken orally) may be safer than IV administration. The liposomal spheres protect the ligand from binding to minerals in the gut and allow for a slower, more controlled release into the bloodstream, reducing the "vacuum effect" on the kidneys.
4. Post-Chelation Remineralisation
Following any chelation event, there must be a 48-hour "window" where no ligands are taken, and high-dose trace minerals are re-introduced. This "pulsed" approach allows the body to fill the "holes" in the enzymes before the next round of mobilisation.
5. Genetic Testing (SNPs)
Before considering chelation, individuals should test for mutations in the MTHFR and GST (Glutathione S-Transferase) genes.
- —Those with "slow" detoxification genetics will be unable to process the metals mobilised by synthetic ligands, leading to severe "Herxheimer" (die-off) reactions and systemic toxicity.
---
Summary: Key Takeaways
The path of heavy metal chelation is fraught with biological traps. While the desire to cleanse the body of industrial filth is noble, the methods used must respect the intricate balance of human biochemistry.
- —Synthetic Ligands are Non-Selective: EDTA, DMSA, and DMPS do not distinguish between toxic and essential metals. They will strip your zinc and magnesium with the same "ferocity" they use for lead.
- —The Danger of Redistribution: Aggressive chelation can move metals from "safe" storage sites (like bone) into "sensitive" sites (like the brain and kidneys).
- —Kidney Health is Paramount: Never undergo chelation without a full renal panel. The kidneys are the "bottleneck" of the detox process.
- —The "Biology First" Rule: Always prime the body with minerals and glutathione for weeks before introducing a synthetic chelator.
- —Beware the Wellness Hype: IV lounges often prioritise profit and "aesthetic" over the deep, slow biochemical work required for true heavy metal clearance.
At INNERSTANDING, we advocate for a return to "Biological Integrity." The human body possesses remarkable systems for detoxification, provided it has the mineral cofactors and the metabolic energy to drive them. Synthetic ligands should be viewed as a "last resort" or a "targeted tool," not a routine wellness "boost." In the war against heavy metals, the most powerful weapon is not a synthetic claw—it is a well-nourished, biochemically stable cell.
Final Thought: True detoxification is a marathon, not a sprint. To strip the body too quickly is to risk the very foundation of the health you are trying to reclaim.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Synthetic chelating agents often lack specificity for toxic metals, leading to the unintended depletion of essential trace elements like zinc and manganese during clinical application.
While intravenous EDTA chelation therapy may offer benefits in specific diabetic populations, it carries inherent risks of hypocalcemia and requires rigorous monitoring of renal function.
The redistribution of heavy metals from peripheral tissues to the central nervous system is a significant risk factor when synthetic chelators are administered without adequate preparation of excretion pathways.
The clinical utility of synthetic ligands is frequently limited by their inherent systemic toxicity and the potential for mobilizing sequestered metals into highly sensitive organs like the brain.
Certain synthetic ligand-metal complexes can trigger intracellular oxidative stress and mitochondrial dysfunction if the resulting complex is not promptly eliminated from the body.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Heavy Metal Chelation: Biological Risks of Synthetic Ligands"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on IV Therapy & Nutrient Infusions — products curated by our research team for educational relevance and biological support.
Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

C60 Charcoal – Supports Healthy Digestion and Detoxification.

Lugol’s Iodine – Hormonal Issues, Menopause, Immune System, Brain Fog, Memory, Thyroid, Dry Skin
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper