
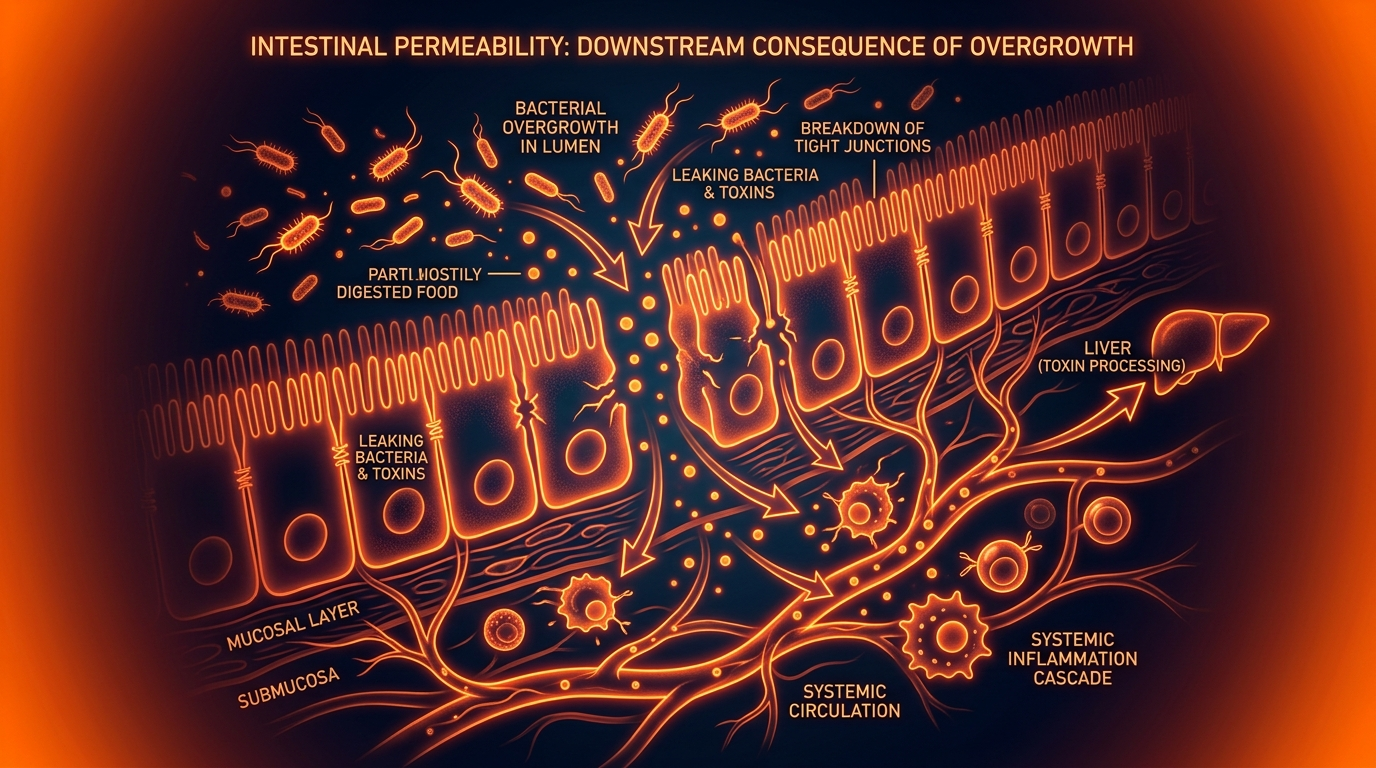
Intestinal Permeability: The Downstream Consequence of Overgrowth
Bacterial byproducts like Lipopolysaccharides (LPS) can degrade the tight junctions of the intestinal lining. This 'leaky gut' allows toxins to enter the bloodstream, triggering systemic immune activation and chronic fatigue.
Overview
The human gastrointestinal tract is a marvel of evolutionary engineering, serving as a selective gateway between the external world and our internal milieu. It is tasked with the monumental challenge of absorbing vital nutrients while simultaneously excluding a literal army of pathogens, environmental toxins, and undigested macromolecules. This delicate balance is maintained by the intestinal barrier—a sophisticated, multi-layered "biological firewall." However, in the modern era, this firewall is under siege. At the heart of this systemic collapse is a condition known as Intestinal Permeability, colloquially termed "Leaky Gut," which is increasingly recognised not as a primary disease, but as a devastating downstream consequence of microbial dysbiosis, specifically Small Intestinal Bacterial Overgrowth (SIBO).
When the small intestine—an area designed for nutrient absorption and kept relatively sterile compared to the colon—becomes colonised by an overgrowth of bacteria, the ecological fallout is profound. These bacteria produce metabolic byproducts, the most notorious being Lipopolysaccharides (LPS). These endotoxins act as molecular chisels, relentlessly degrading the structural integrity of the gut lining. As the "tight junctions" between epithelial cells fail, the barrier becomes porous. This is the inflection point where a localised digestive issue transforms into a systemic inflammatory catastrophe.
The implications are far-reaching. Once the barrier is breached, the systemic circulation is flooded with bacterial debris and environmental toxins, a state known as metabolic endotoxemia. This triggers a persistent, low-grade immune activation that exhausts the body's resources, manifesting as chronic fatigue, brain fog, and autoimmune activation. In this article, we will peel back the layers of this silent epidemic, exposing the cellular mechanisms of destruction and the environmental catalysts that the mainstream medical narrative has, until now, largely ignored.
##
The Biology — How It Works
To understand the pathology of intestinal permeability, one must first appreciate the intricate architecture of the healthy gut barrier. The barrier is not a single wall but a dynamic, three-tiered defence system.
The Biochemical Tier: The Mucosal Veil
The first line of defence is the mucous layer. In the small intestine, this layer is relatively thin but highly functional, containing antimicrobial peptides (AMPs) and Secretory Immunoglobulin A (sIgA). This "biochemical soup" is designed to neutralise pathogens before they even reach the cellular surface. In a state of SIBO, the sheer volume of bacteria and their enzymatic output can deconjugate bile acids and degrade this protective mucous, leaving the underlying cells exposed.
The Physical Tier: The Epithelial Monolayer
The second tier consists of a single layer of columnar epithelial cells (enterocytes). Unlike the skin, which is many layers thick, the gut lining is a single cell deep. This is a design necessity—nutrients must pass through easily—but it creates an inherent vulnerability. These cells are tethered together by a complex protein network known as the Apical Junctional Complex, of which the Tight Junctions (TJs) are the most critical. These junctions act as the "gatekeepers," regulating the paracellular pathway (the space between cells).
The Immunological Tier: The GALT
Beneath the epithelial layer lies the Gut-Associated Lymphoid Tissue (GALT), housing approximately 70% of the body’s immune system. This includes T-cells, B-cells, and macrophages residing in the *lamina propria*. In a healthy state, these immune cells are "tolerant." However, when the physical barrier fails, these cells transition into a state of "high alert," initiating an inflammatory cascade that can reverberate throughout the entire body.
UK FACT: Chronic fatigue syndrome (ME/CFS) affects approximately 250,000 people in the UK. Emerging research suggests that up to 70% of these patients exhibit clinical markers of intestinal permeability and SIBO, indicating a direct link between gut barrier failure and systemic energy depletion.
##
Mechanisms at the Cellular Level
The transition from a healthy gut to a "leaky" one is a highly orchestrated molecular failure. The primary antagonist in this process is Lipopolysaccharide (LPS), a structural component found in the outer membrane of Gram-negative bacteria (the type most commonly associated with SIBO).
LPS and the TLR4 Activation
LPS is a potent endotoxin. When bacteria overgrow and subsequently die or replicate in the small intestine, LPS is released in massive quantities. These molecules bind to Toll-Like Receptor 4 (TLR4), which are embedded in the membranes of both intestinal epithelial cells and underlying immune cells.
The activation of TLR4 triggers a signal transduction pathway involving the protein MyD88. This culminates in the activation of Nuclear Factor-kappa B (NF-κB), the "master switch" of inflammation. Once NF-κB is activated, the cell begins producing pro-inflammatory cytokines such as TNF-alpha and IL-6. These cytokines do not stay localised; they circulate, inducing systemic inflammation.
The Disruption of Tight Junction Proteins
The physical "leaking" occurs because of the degradation of specific proteins: Occludin, Claudins, and Zonula Occludens (ZO-1). Under the influence of LPS-induced inflammation:
- —Zonulin Release: The body releases zonulin, a protein that modulates intestinal permeability. High levels of zonulin act as a key that unlocks the tight junctions, causing them to physically pull apart.
- —Myosin Light Chain Kinase (MLCK) Activation: Inflammation activates the MLCK pathway, which causes the perijunctional actin-myosin ring to contract. Imagine a drawstring bag being pulled too tight—the "opening" (the space between cells) widens, allowing large molecules to slip through.
Metabolic Endotoxemia: The Silent Flood
When the junctions are open, LPS enters the portal circulation (the blood flow from the gut to the liver). This state is known as Metabolic Endotoxemia. While a massive bacterial infection (sepsis) leads to an acute, life-threatening response, metabolic endotoxemia is a "stealth" version. The levels of LPS are 10-100 times lower than in sepsis, but they are persistent. This constant drip-feed of toxins ensures that the immune system never returns to a state of rest, leading to the cellular exhaustion characteristic of chronic fatigue.
##
Environmental Threats and Biological Disruptors
While SIBO is the internal driver of permeability, several external factors act as catalysts, priming the gut for barrier failure. We are currently living in an environment that is biologically "hostile" to the intestinal lining.
The Glyphosate Paradigm
In the UK and globally, the use of glyphosate-based herbicides has surged. Glyphosate acts as a "stealth antibiotic," selectively killing beneficial gut bacteria while allowing pathogenic, LPS-producing strains to flourish. Furthermore, glyphosate has been shown to directly interfere with the tight junction proteins by stimulating the overproduction of zonulin.
Ultra-Processed Foods (UPFs) and Emulsifiers
The modern British diet is heavily reliant on UPFs. Common food additives like carboxymethylcellulose and polysorbate-80 act like detergents. They literally wash away the protective mucous layer of the gut, bringing bacteria into direct contact with the epithelial cells and accelerating the inflammatory cycle.
Pharmaceutical Over-reliance
The widespread use of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) such as ibuprofen is a major contributor. NSAIDs inhibit prostaglandins, which are necessary for the maintenance and repair of the gastric and intestinal mucosa. When combined with the bacterial pressure of SIBO, NSAIDs can cause "micro-ulcerations," creating literal holes in the barrier.
ALARMING STATISTIC: According to data from the British Society of Gastroenterology, prescriptions for Proton Pump Inhibitors (PPIs) have risen dramatically. By suppressing stomach acid, PPIs remove the primary "acid barrier" that prevents bacteria from migrating into the small intestine, directly facilitating the development of SIBO and subsequent intestinal permeability.
##
The Cascade: From Exposure to Disease
The progression from intestinal permeability to systemic disease follows a predictable, yet devastating, cascade. It is not merely a "tummy ache"; it is a total systemic breakdown.
Phase 1: Localised Malabsorption
In the early stages of SIBO and leaky gut, the damage to the brush border enzymes (enzymes located on the tips of the microvilli) leads to malabsorption. Carbohydrates and proteins go undigested, further feeding the bacterial overgrowth and creating a vicious cycle of fermentation, bloating, and gas.
Phase 2: The Liver-Gut Axis Overload
Every drop of blood leaving the gut goes to the liver via the portal vein. The liver is tasked with filtering out the LPS and toxins that have leaked through. However, in cases of chronic intestinal permeability, the liver becomes overwhelmed. This leads to Non-Alcoholic Fatty Liver Disease (NAFLD) and the release of further inflammatory markers into the systemic circulation.
Phase 3: Systemic Immune Activation
Once the liver is bypassed, LPS reaches every organ system. In the joints, it triggers rheumatoid-like symptoms; in the skin, it manifests as eczema or psoriasis; and most critically, in the brain, it triggers neuroinflammation.
Phase 4: The Breach of the Blood-Brain Barrier (BBB)
The most alarming aspect of intestinal permeability is its effect on the brain. The same proteins that regulate the gut barrier also regulate the Blood-Brain Barrier. When zonulin levels are high in the gut, they are often high in the brain. This "Leaky Brain" allow LPS and immune cells to enter the central nervous system, activating the brain's resident immune cells (microglia). This results in the profound "brain fog," cognitive decline, and chronic fatigue that define the modern patient experience.
##
What the Mainstream Narrative Omits
The refusal of mainstream clinical medicine to fully integrate the concept of "Leaky Gut" into standard practice is perhaps the greatest tragedy of modern healthcare. While the scientific literature is overflowing with evidence—searching "Intestinal Permeability" on PubMed yields over 15,000 results—the clinical application remains decades behind.
The Diagnostic Lag
Most GPs are trained to look for "macro" diseases: Crohn’s, Ulcerative Colitis, or Celiac Disease. If a patient does not present with overt tissue destruction visible on an endoscopy, they are often dismissed with a diagnosis of "IBS"—a "wastebasket" diagnosis that describes symptoms without explaining the underlying cause. Intestinal permeability is a "functional" disorder; it is a failure of *operation*, not just *structure*.
The Pharmaceutical Bias
The current medical model is built on "one pill for one ill." There is no single drug to "fix" a leaky gut. Repairing the barrier requires a multi-faceted approach involving diet, lifestyle, and targeted supplementation. Because this doesn't fit the profitable pharmaceutical model, it is often relegated to the realm of "alternative medicine," despite its rigorous biological basis.
The SIBO Blind Spot
Furthermore, the mainstream narrative often treats SIBO as a rare condition associated only with "Short Bowel Syndrome" or major surgery. In reality, SIBO is an epidemic driven by our modern lifestyle, and it is the primary engine behind the "leaking" of the gut. By failing to test for and treat SIBO using breath testing and prokinetic therapy, doctors are merely "moping the floor while the tap is still running."
##
The UK Context
The United Kingdom presents a unique landscape for the proliferation of intestinal permeability. Several factors make the British population particularly vulnerable to this biological "perfect storm."
The "Standard British Diet" (SBD)
The UK has one of the highest consumptions of ultra-processed foods in Europe. The reliance on refined grains, emulsifiers, and low-fibre "convenience" foods provides the ideal substrate for Gram-negative bacteria to thrive in the small intestine. The lack of fermentable fibre also means our beneficial colonic bacteria are starved, leading to a breakdown in the cross-talk between the colon and the small intestine.
NHS Limitations and the "Zip-Code Lottery"
While the NHS provides essential care, its resources for functional gastrointestinal disorders are severely overstretched. Access to Hydrogen/Methane Breath Testing (HBT)—the gold standard for SIBO diagnosis—is inconsistent across different trusts. Many patients are forced to seek private testing or remain in a cycle of "managing" symptoms with antacids and laxatives.
Environmental Factors in the UK
The UK’s damp climate and the prevalence of older housing stock contribute to mould and mycotoxin exposure. Mycotoxins are potent disruptors of the intestinal barrier, often working synergistically with LPS to exacerbate "leaky gut." For a British patient, the combination of a UPF-rich diet, chronic stress, and environmental mould can make gut recovery exceptionally challenging.
CALLOUT: A 2022 study highlighted that nearly 40% of UK adults suffer from at least one digestive symptom. This is not "normal"; it is a sign of a collapsing biological barrier.
##
Protective Measures and Recovery Protocols
Recovery from intestinal permeability and SIBO is not an overnight process. It requires a strategic, tiered approach to remove the offenders, repair the masonry, and restore the ecological balance.
Step 1: Eradicate the Overgrowth
You cannot fix the barrier if LPS is still being produced in excess. This involves:
- —Targeted Antimicrobials: Using herbal protocols (e.g., Allicin, Berberine, Neem) or specific antibiotics (e.g., Rifaximin) that remain in the gut to reduce the bacterial load without systemic side effects.
- —The Low FODMAP or Elemental Diet: Starving the bacteria of their preferred fuel source to reduce fermentation and LPS production.
Step 2: Seal the Breach (The Repair Phase)
Once the bacterial pressure is reduced, the focus must shift to structural repair:
- —L-Glutamine: The primary fuel for enterocytes. It helps "knit" the tight junctions back together.
- —Zinc Carnosine: A potent compound that has been clinically shown to stabilise the small intestinal mucosa and promote the repair of the epithelial lining.
- —Colostrum or Serum-Derived Immunoglobulins: These act as "molecular sponges," binding to LPS in the gut lumen and preventing it from ever reaching the epithelial wall.
Step 3: Support the "Gatekeepers"
- —Prokinetics: To prevent SIBO from recurring, the "Migrating Motor Complex" (the gut's internal sweeping mechanism) must be supported. This ensures that bacteria are physically moved from the small intestine into the colon.
- —Vagus Nerve Support: The gut-brain axis is a two-way street. Managing stress and supporting vagal tone is essential for maintaining the biochemical integrity of the gut lining.
Step 4: Environmental Mitigation
- —Filtration: Using high-quality water filters to remove chlorine and fluoride, both of which can disrupt the microbiome and the mucous layer.
- —Organic Sourcing: Prioritising organic produce to reduce glyphosate exposure, particularly in "high-risk" foods like oats and wheat.
##
Summary: Key Takeaways
Intestinal permeability is far more than a digestive inconvenience; it is a foundational collapse of human biology. When SIBO takes hold, the small intestine becomes a factory for LPS—a toxin that acts as a biological wrecking ball against our cellular defences.
- —The Mechanism: LPS triggers the TLR4/NF-κB pathway, leading to the release of zonulin and the physical pulling apart of tight junctions.
- —The Consequence: Metabolic endotoxemia—the systemic flood of toxins—leads to chronic inflammation, neuroinflammation, and the "leaky brain" phenomenon.
- —The Cause: SIBO is the primary driver, exacerbated by glyphosate, ultra-processed foods, and a medical system that focuses on symptoms rather than root causes.
- —The Solution: A comprehensive approach that addresses the microbial overgrowth, repairs the structural proteins, and mitigates environmental toxins.
As we move forward, we must stop viewing the gut as an isolated tube and start seeing it for what it truly is: the front line of our immune system. To ignore the health of the intestinal barrier is to ignore the foundation of human vitality. At INNERSTANDING, we believe that reclaiming your health begins with understanding these invisible mechanisms and taking decisive, biologically-informed action to restore your internal firewall. The "downstream" consequences are clear; it is time we head upstream to the source.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Small intestinal bacterial overgrowth contributes to intestinal barrier dysfunction by altering tight junction protein expression and increasing paracellular permeability.
Bacterial lipopolysaccharides derived from gut microbiota overgrowth trigger metabolic endotoxemia by crossing the impaired intestinal epithelial barrier into the systemic circulation.
Chronic dysbiosis in the small intestine induces a proinflammatory response that degrades the mucosal layer, leading to increased intestinal permeability and systemic inflammation.
Malabsorption and bacterial byproduct accumulation in SIBO patients correlate with structural changes in the intestinal mucosa that facilitate the translocation of antigens.
The regulation of the intestinal epithelial barrier is directly compromised by bacterial toxins which induce the phosphorylation of myosin light chain, leading to tight junction opening.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Intestinal Permeability: The Downstream Consequence of Overgrowth"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper


