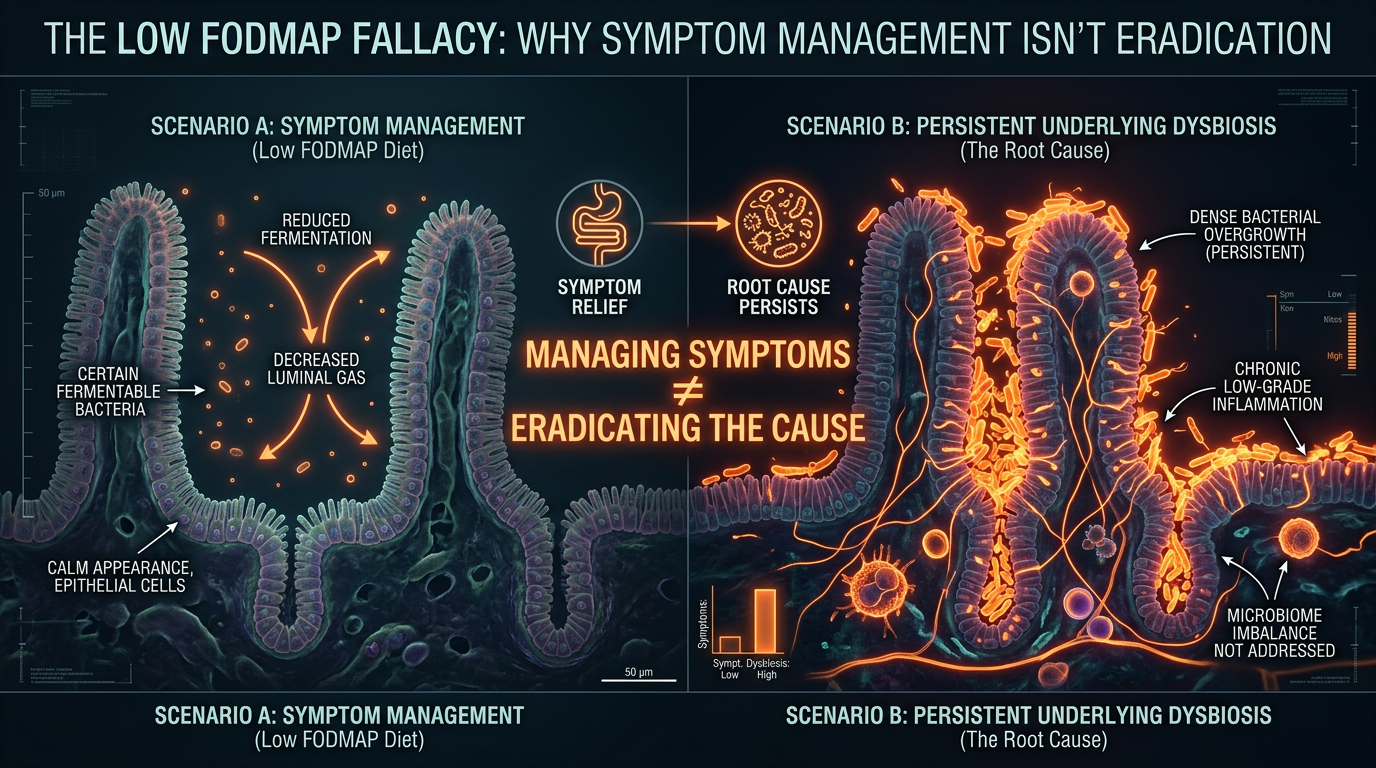
The Low FODMAP Fallacy: Why Symptom Management Isn't Eradication
While a low FODMAP diet reduces the gas produced by bacteria, it does not kill the overgrowth and may lead to long-term microbiome depletion. We argue against using restrictive diets as a primary solution for SIBO.
Overview
The modern gastroenterological landscape is currently dominated by a singular, restrictive paradigm: the Low FODMAP (Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols) diet. Marketed as the "gold standard" for managing irritable bowel syndrome (IBS) and its primary underlying driver, Small Intestinal Bacterial Overgrowth (SIBO), this dietary intervention has become a global phenomenon. However, as we delve deeper into the molecular biology of the human microbiome and the physiological mechanics of the small intestine, a troubling reality emerges. The Low FODMAP diet is not a cure; it is a temporary suppression of symptoms that, when used as a long-term strategy, risks permanent ecological damage to the host’s internal environment.
At INNERSTANDING, we classify the over-reliance on the Low FODMAP diet as a "biological fallacy." The fallacy lies in the assumption that by depriving bacteria of their preferred fuel sources, we are somehow "starving out" the infection or resolving the dysbiosis. In reality, SIBO is not a problem of food; it is a problem of location and motility. By focusing on the removal of fermentable carbohydrates, we are merely silencing the alarm bells while the fire continues to smoulder beneath the floorboards. Furthermore, the systematic removal of these prebiotic fibres leads to a catastrophic decline in microbial diversity within the large intestine, potentially predisposing patients to a host of secondary metabolic and immunological disorders.
This article serves as an exhaustive investigation into the mechanisms of SIBO, the failure of the restrictive dietary model, and the biological necessity of shifting our focus from "starvation" to "eradication and restoration." We will explore why the current mainstream approach is failing millions of patients, particularly within the United Kingdom’s overstretched healthcare system, and provide a roadmap for true biological recovery.
##
The Biology — How It Works

Panaceum – Prebiotic Oligosaccharide Complex
Panaceum is a specialist eight-oligosaccharide blend designed to restore the microbial diversity missing from the modern Western diet. By providing the complex fibres our ancestors once consumed, it feeds and sustains a resilient gut microbiome for long-term health.
Vetting Notes
Pending
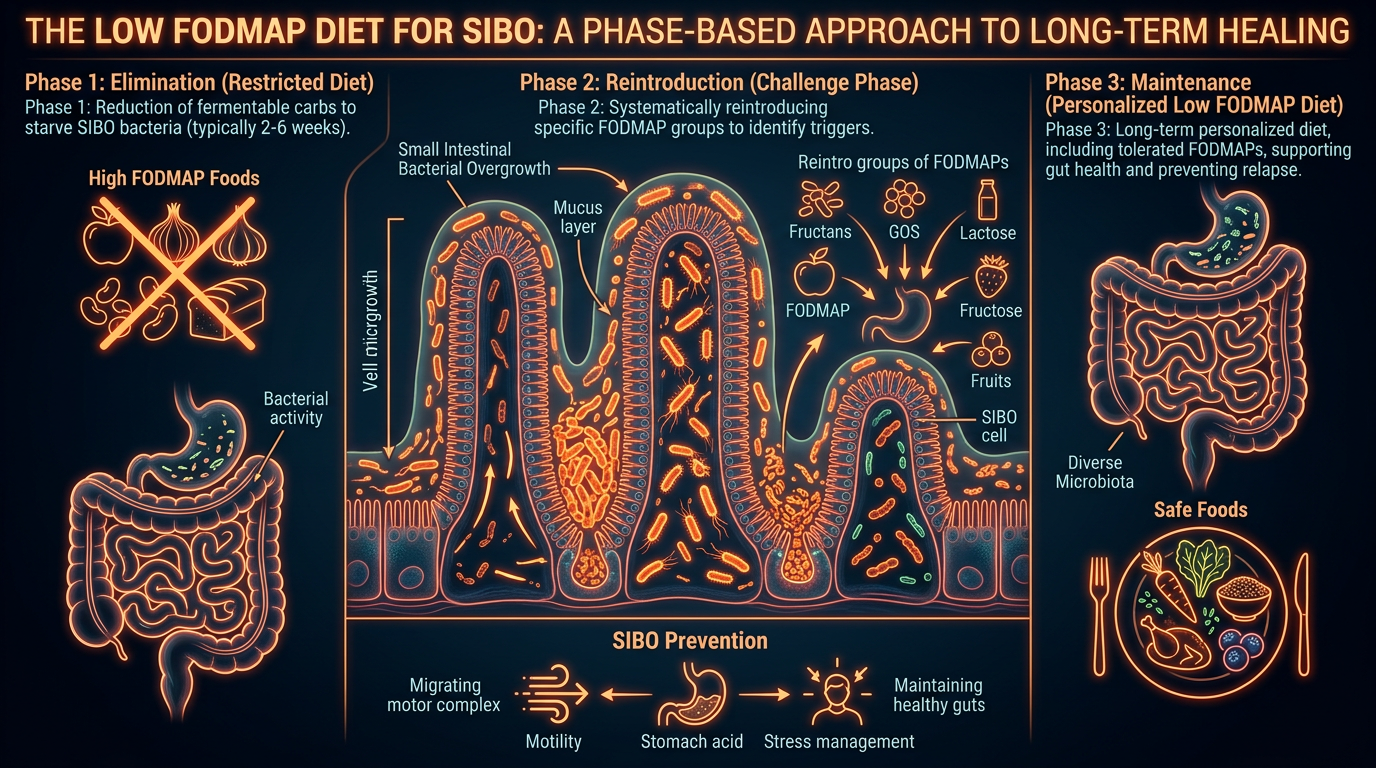
To understand why the Low FODMAP diet fails as a curative measure, one must first understand the biological topography of the human digestive tract. The small intestine is designed to be a relatively sterile environment, containing approximately $10^3$ bacteria per millilitre of fluid, compared to the $10^{12}$ found in the colon. Its primary function is the chemical digestion of food and the absorption of nutrients. SIBO occurs when the microbial populations typically resident in the large intestine migrate upwards or when indigenous small intestinal populations proliferate uncontrollably.
The FODMAP Mechanism
FODMAPs are short-chain carbohydrates and sugar alcohols that are poorly absorbed in the small intestine. They are highly osmotic, meaning they pull water into the intestinal lumen, and they are rapidly fermented by bacteria. In a healthy individual, this fermentation occurs primarily in the large intestine, where it produces beneficial short-chain fatty acids (SCFAs) like butyrate, which fuel the colonic lining and regulate the immune system.
However, in the SIBO-afflicted gut, these carbohydrates meet a dense population of bacteria long before they reach the colon. The result is a rapid, premature fermentation process. The bacteria metabolise these sugars and release gases—hydrogen ($H_2$), methane ($CH_4$), or hydrogen sulphide ($H_2S$)—as metabolic byproducts. These gases cause the physical distension of the small intestine, leading to the clinical symptoms of bloating, abdominal pain, and altered bowel habits.
The Fallacy of Starvation
The logic of the Low FODMAP diet is simple: remove the fuel, stop the gas. While this successfully reduces the physical pressure on the intestinal wall and alleviates pain, it does nothing to address the presence of the bacteria themselves. Bacteria are highly adaptable biological entities. When deprived of their primary carbohydrate sources, many SIBO-related species can enter a state of dormancy or switch to metabolising the protective mucus layer (the glycocalyx) of the intestinal lining. This "starvation" approach does not kill the overgrowth; it merely forces it to change its metabolic strategy, often at the expense of the host’s mucosal integrity.
UK STATISTICAL ALERT: It is estimated that 1 in 10 people in the UK suffer from IBS symptoms, yet over 80% of those with IBS are believed to have underlying SIBO. Despite this, SIBO testing remains largely unavailable on the NHS, leading to a "diagnosis by diet" approach that ignores the root cause.
##
Mechanisms at the Cellular Level
To truly grasp the failure of symptom management, we must look at the cellular and molecular triggers that maintain the SIBO state. The small intestine is not a passive tube; it is a highly sophisticated muscular and neurological organ.
The Migrating Motor Complex (MMC)
The most critical mechanism in SIBO pathology is the failure of the Migrating Motor Complex (MMC). The MMC is a distinct pattern of electromechanical activity observed in gastrointestinal smooth muscle during periods of fasting. It acts as a "cleansing wave" or "intestinal housekeeper," physically sweeping undigested food and excess bacteria out of the small intestine and into the colon.
At the cellular level, this process is coordinated by the Interstitial Cells of Cajal (ICC)—the pacemakers of the gut—and the enteric nervous system. When the MMC is impaired, bacteria remain stagnant in the small intestine, where they find a warm, moist environment perfect for colonisation. A Low FODMAP diet does absolutely nothing to restore the MMC. In fact, by focusing on frequent, small, "safe" meals, many patients inadvertently keep themselves in a "fed" state, which chronically suppresses the MMC, thereby exacerbating the very condition they are trying to treat.
The Brush Border and Enzymatic Failure
The lining of the small intestine is covered in microscopic projections called microvilli, collectively known as the brush border. This is where crucial enzymes like lactase, sucrase, and maltase are produced to break down carbohydrates. In a state of SIBO, the bacterial overgrowth can physically damage these microvilli and produce enzymes that deconjugate bile acids and interfere with the host’s digestive enzymes.
When we apply a Low FODMAP diet, we are essentially compensating for a damaged brush border. We stop eating the foods that require these enzymes. However, this lack of stimulation can lead to further atrophy of the brush border. The cells of the small intestine require the presence of certain nutrients and the "work" of digestion to maintain their structural integrity. Long-term avoidance leads to a "lazy" gut, where the capacity to produce these vital enzymes diminishes even further, making the patient increasingly reactive to a wider range of foods.
##
Environmental Threats and Biological Disruptors
The rise of SIBO and the subsequent reliance on restrictive diets cannot be viewed in isolation from the environmental toxins that have compromised human biology over the last five decades.
Glyphosate and the Shikimate Pathway
The pervasive use of glyphosate-based herbicides in UK and global agriculture is a primary driver of gut dysbiosis. While proponents of glyphosate argue that it is non-toxic to humans because we lack the shikimate pathway, this ignores the fact that our gut bacteria do possess this pathway. Glyphosate acts as a potent antibiotic, selectively killing beneficial species while allowing pathogenic, SIBO-associated bacteria (which are often resistant) to thrive. Furthermore, glyphosate acts as a mineral chelator, stripping the body of the manganese and zinc required for the production of digestive enzymes and the maintenance of the intestinal barrier.
The PPI Epidemic
Mainstream medicine’s reflexive prescription of Proton Pump Inhibitors (PPIs) for any sign of indigestion is a direct precursor to SIBO. Gastric acid is the first line of defence against bacterial ingestion. By chemically suppressing stomach acid to treat symptoms of reflux—which is often itself caused by a *lack* of acid or SIBO-driven gas pressure—we open the gates for bacterial invasion. In the absence of an acidic "firewall," the small intestine becomes an open colony for oral and colonic flora.
FACT: Long-term use of PPIs has been clinically shown to increase the risk of developing SIBO by up to 50%. In the UK, over 60 million prescriptions for PPIs are issued annually, creating a self-perpetuating cycle of digestive dysfunction.
Stress and the Vagus Nerve
Modern environmental stress is a biological disruptor that directly impacts the physical movement of the gut. The vagus nerve is the primary conduit for the "rest and digest" system. Chronic sympathetic nervous system activation (the "fight or flight" response) inhibits vagal tone. Without strong vagal signalling, the MMC fails to fire, stomach acid production drops, and the ileocecal valve (the gate between the small and large intestine) may become "leaky" or stuck open, allowing colonic bacteria to backflow into the small intestine.
##
The Cascade: From Exposure to Disease
The progression from initial bacterial overgrowth to systemic disease is a multi-stage cascade that a Low FODMAP diet is powerless to stop.
Stage 1: Dysbiosis and Gas Production
The initial stage is characterized by the fermentation of carbohydrates and the production of gases. Hydrogen-dominant SIBO typically correlates with diarrhoea, as the hydrogen gas speeds up transit time. Methane-dominant overgrowth (technically caused by archaea like *Methanobrevibacter smithii*) correlates with constipation, as methane acts as a local paralytic to the gut muscles.
Stage 2: Intestinal Permeability (Leaky Gut)
As the bacteria proliferate, they produce metabolic byproducts such as Lipopolysaccharides (LPS)—endotoxins found in the cell walls of Gram-negative bacteria. LPS triggers an inflammatory response that degrades the "tight junctions" between the cells of the intestinal lining. This results in intestinal permeability, or "leaky gut." At this stage, undigested food particles and bacterial toxins leak into the bloodstream.
Stage 3: Systemic Inflammation and Immune Activation
Once these foreign substances enter the systemic circulation, the immune system goes into a state of high alert. This leads to the production of pro-inflammatory cytokines and the formation of circulating immune complexes. This is why SIBO is so frequently associated with extra-intestinal symptoms such as:
- —Fibromyalgia and Chronic Fatigue: Driven by systemic inflammation and mitochondrial dysfunction.
- —Brain Fog: Caused by the production of D-lactic acid and ammonia by the overgrowth.
- —Skin Conditions: Including acne rosacea and eczema, which are often "skin manifestations" of gut-derived inflammation.
Stage 4: Nutrient Depletion
Bacteria in the small intestine are "first at the table." They consume the host’s nutrients before they can be absorbed. Specifically, they have a high affinity for Vitamin B12 and iron, leading to refractory anaemias and neurological symptoms. They also deconjugate bile acids, leading to the malabsorption of fat-soluble vitamins (A, D, E, K). A Low FODMAP diet, by its very nature, is nutrient-poor compared to a diverse whole-food diet, often accelerating these deficiencies rather than correcting them.
##
What the Mainstream Narrative Omits
The promotion of the Low FODMAP diet by national health services and dietetic associations is a masterpiece of reductionist medicine. It treats the body as a collection of symptoms rather than a complex ecological system. Here is what the mainstream narrative conveniently omits:
The Great Extinction
The most dangerous consequence of the Low FODMAP fallacy is the "Great Extinction" of the colonic microbiome. Our beneficial bacteria—the ones responsible for producing anti-inflammatory compounds, regulating our mood via neurotransmitters, and preventing colon cancer—depend on the very fibres that the Low FODMAP diet removes.
Studies have shown that just three to four weeks on a strict Low FODMAP diet significantly reduces the concentration of *Bifidobacteria* and *Akkermansia muciniphila*. *Akkermansia* is a keystone species that maintains the gut barrier; its loss is linked to obesity, diabetes, and autoimmune disease. By "starving" the SIBO in the small intestine, we are effectively nuking the rainforest of the large intestine.
Biofilms: The Bacterial Fortress
Mainstream advice almost never mentions biofilms. Bacteria in SIBO do not just float freely; they secrete a protective extracellular matrix (a biofilm) that shields them from the host’s immune system and from antimicrobials. A restrictive diet does nothing to penetrate these fortresses. This is why many patients find that as soon as they reintroduce a "high FODMAP" food—even after months of strict adherence—their symptoms return instantly. The bacteria were never gone; they were just hiding behind a biofilm wall, waiting for a fuel source to arrive.
The Psychological Cost of Orthorexia
We must also address the psychological impact of being told that "healthy" foods like apples, garlic, onions, and lentils are "poison." The Low FODMAP diet often leads to a form of medically-induced orthorexia, where patients become terrified of food. This stress response further inhibits the vagus nerve and the MMC, creating a self-fulfilling prophecy where the patient’s digestion becomes so fragile that they can only tolerate a handful of "safe" foods.
##
The UK Context
In the United Kingdom, the management of SIBO and the application of the Low FODMAP diet are particularly fraught with systemic issues. The NHS model is built on "cost-effectiveness" and "stabilisation," which is fundamentally at odds with the complex, individualised care required to treat chronic dysbiosis.
UK REALITY CHECK: The average wait time for a gastroenterology consultation in some NHS trusts exceeds 40 weeks. During this time, the standard primary care advice is "try a Low FODMAP diet." This leaves patients in a state of chronic nutrient deprivation and microbiome depletion for nearly a year before any diagnostic testing is even considered.
The Rise of Ultra-Processed "Safe" Foods
UK supermarkets—Tesco, Sainsbury's, and Waitrose—have capitalised on the FODMAP trend by introducing "Low FODMAP" ranges. These products are often highly processed, containing refined starches, industrial seed oils, and synthetic emulsifiers. While they may not cause immediate bloating (because they lack fermentable sugars), these ingredients are notoriously inflammatory and harmful to the gut lining. We are seeing a generation of UK patients who are "symptom-free" on a diet of gluten-free white bread and processed snacks, but who are internally malnourished and systemically inflamed.
The Lack of Breath Testing
While breath testing (using glucose or lactulose) is the standard for SIBO diagnosis globally, its availability on the NHS is patchy at best. Many UK consultants still view SIBO as a "niche" condition only relevant to those with "Short Bowel Syndrome" or structural abnormalities, ignoring the massive body of evidence linking it to functional dyspepsia and IBS in the general population. This diagnostic vacuum is what allows the Low FODMAP fallacy to flourish.
##
Protective Measures and Recovery Protocols
If the Low FODMAP diet is a fallacy, what is the solution? True eradication and recovery require a multi-phasic biological approach that prioritises function over deprivation.
Phase 1: Biofilm Disruption and Antimicrobial Intervention
Instead of merely starving the bacteria, we must actively dismantle their defences and reduce their numbers.
- —Biofilm Disruptors: Substances like bismuth subnitrate, alpha-lipoic acid, and specific enzymes (interphase plus) can be used to "crack open" the bacterial shields.
- —Herbal Antimicrobials: Clinical trials (notably from Johns Hopkins University) have shown that herbal protocols using Oregano oil, Berberine, Neem, and Allicin (from garlic) are as effective, if not more so, than the pharmaceutical antibiotic Rifaximin. Unlike Rifaximin, these herbs have a broad-spectrum effect that also addresses fungal overgrowth (SIFO), which often co-exists with SIBO.
Phase 2: Restoring the Migrating Motor Complex (MMC)
This is the most critical and most ignored step. To prevent relapse, we must fix the "housekeeping" waves.
- —Prokinetics: Substances that stimulate the MMC. This can include pharmaceutical options like low-dose Erythromycin or Prucalopride, or natural options like Ginger and Artichoke extract.
- —Meal Spacing: At INNERSTANDING, we advocate for a minimum of 4–5 hours between meals and a 12-hour overnight fast. This ensures the MMC has the time and the "fasted state" environment it needs to function.
- —Vagal Nerve Stimulation: Techniques such as gargling, singing, and cold-water immersion can help reset the parasympathetic nervous system and improve gut motility.
Phase 3: The Strategic Reintroduction of Fiber
The goal is not to stay Low FODMAP forever, but to become FODMAP resilient. Once the bacterial load is reduced, we must slowly and systematically reintroduce fermentable fibres to rebuild the colonic microbiome.
- —PHGG (Partially Hydrolysed Guar Gum): A unique fibre that is generally well-tolerated by SIBO patients and has been shown to increase the effectiveness of eradication treatments.
- —Diversity Over Restriction: The focus should be on "The 30 Plant Rule"—aiming for 30 different plant species per week to provide a diverse range of prebiotics for the colon.
Phase 4: Environmental Detoxification
Recovery is impossible if the biological terrain remains toxic.
- —Organic Sourcing: Transitioning to organic produce is non-negotiable for the SIBO patient to avoid glyphosate-induced dysbiosis.
- —Water Filtration: Using high-quality filters to remove chlorine and fluoride from tap water, both of which have antimicrobial properties that can further disrupt the delicate small intestinal balance.
##
Summary: Key Takeaways
The Low FODMAP diet is a pharmacological tool masquerading as a nutritional strategy. While it offers a much-needed reprieve from the debilitating symptoms of SIBO, it is essentially a "biological pause button" that fails to address the underlying physiological dysfunction.
- —SIBO is a Motility Disorder: The root cause is almost always a failure of the Migrating Motor Complex (MMC), not the consumption of onions or garlic.
- —Starvation is Not Eradication: Bacteria can adapt to nutrient deprivation; they must be actively cleared through antimicrobial intervention and biofilm disruption.
- —Long-term Restriction is Dangerous: Chronic avoidance of FODMAPs leads to the "Great Extinction" of the colonic microbiome, increasing the risk of systemic disease and permanent metabolic damage.
- —The UK System is Flawed: Reliance on "diagnosis by diet" due to NHS constraints is failing patients. Proactive, private testing and a functional medicine approach are often necessary for true recovery.
- —The Goal is Resilience: Success is not measured by how many foods you can avoid, but by how many foods your body can successfully digest and metabolise without reaction.
We must move beyond the era of restrictive dieting and enter an era of restorative gastroenterology. The small intestine is a temple of absorption and vitality; it is time we stopped treating it like a sterile tube that needs to be starved, and started treating it like the sophisticated, living ecosystem that it is. The fallacy is over; the era of eradication and restoration begins now.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "The Low FODMAP Fallacy: Why Symptom Management Isn't Eradication"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.
Panaceum – Prebiotic Oligosaccharide Complex

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper