Fibrin-Rich Microclots: Why Traditional Blood Tests Miss Post-Viral Vascular Damage
Explore the mechanism of amyloid-like microclots that resist normal breakdown and obstruct capillary flow in post-viral states. This article details why these microscopic obstructions remain invisible to standard medical screening.

# Fibrin-Rich Microclots: Why Traditional Blood Tests Miss Post-Viral Vascular Damage
Overview
In the wake of the global viral events of the early 2020s, a silent pathological crisis has emerged, one that the traditional medical establishment remains largely unequipped to diagnose or treat. Millions of individuals across the United Kingdom and the world find themselves trapped in a state of chronic, debilitating illness—characterised by profound fatigue, cognitive dysfunction (brain fog), and multi-systemic pain. Despite these life-altering symptoms, patients are frequently dismissed after their standard National Health Service (NHS) blood panels return as "perfectly normal."
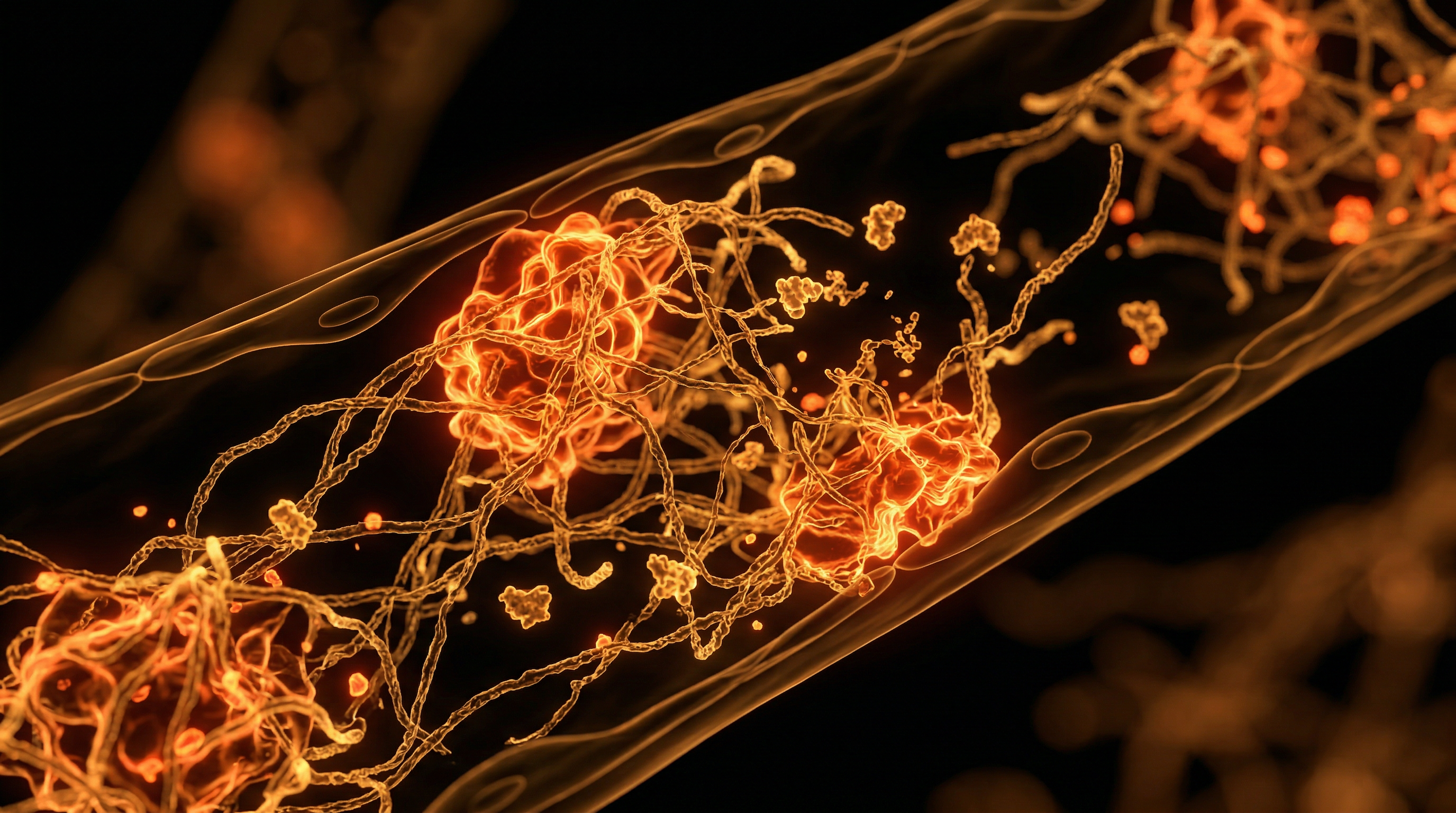
The disconnect between patient suffering and clinical data is not a failure of the patient’s psychology, but a failure of the diagnostic paradigm. Central to this failure is the presence of fibrin-rich microclots—microscopic, amyloid-like structures that obstruct the smallest vessels of the circulatory system. These are not the large, obstructive clots (thrombi) that cause strokes or pulmonary embolisms, which are easily detected via D-dimer tests or CT scans. Instead, these are microscopic "sludge-like" obstructions that resist the body’s natural fibrinolytic (clot-breaking) mechanisms.
These microclots serve as the "smoking gun" in post-viral syndromes, including Long COVID and adverse reactions to spike protein exposure. They act as physical barriers to oxygen delivery at the capillary level, leading to systemic hypoxia (oxygen starvation) and mitochondrial dysfunction. This article will expose the biochemical mechanisms of these clots, explain why they remain invisible to the mainstream medical gaze, and detail the biological pathways that turn a healthy vascular system into a graveyard of persistent, insoluble debris.
Key Fact: Standard D-dimer tests measure the breakdown products of a clot. Because fibrin-rich microclots are highly resistant to degradation, they do not break down into the fragments that these tests are designed to detect, leading to false-negative results in patients with severe vascular pathology.
##
##
The Biology — How It Works
To understand why these microclots are so insidious, one must first understand the transition from normal coagulation to pathological amyloidogenesis. In a healthy state, blood clotting is a finely tuned process. When a vessel is injured, the soluble protein fibrinogen is converted by the enzyme thrombin into insoluble fibrin threads, which form a mesh to trap platelets and seal the wound. Once the vessel heals, the enzyme plasmin dissolves the fibrin mesh, and the system returns to its liquid state.
The Amyloid Shift
In post-viral states, particularly those involving the SARS-CoV-2 spike protein, this process is hijacked. Research led by Professor Resia Pretorius and Professor Douglas Kell has demonstrated that the presence of the spike protein triggers a conformational change in fibrinogen. It forces the protein to misfold into a beta-sheet-rich structure, characteristic of amyloids (similar to the plaques found in the brains of Alzheimer’s patients).
These amyloid-like microclots are fundamentally different from normal blood clots. They are:
- —Protease-Resistant: They possess a molecular structure that makes them virtually "indigestible" by plasmin, the body's natural "clot-buster."
- —Highly Stable: The covalent cross-linking within these clots is far more robust than standard fibrin.
- —Inflammatory Reservoirs: They trap inflammatory cytokines, such as Interleukin-6 (IL-6) and Tumour Necrosis Factor-alpha (TNF-α), within their mesh, preventing these molecules from being cleared and ensuring a state of perpetual low-grade systemic inflammation.
The Capillary Chokepoint
The human body contains approximately 60,000 miles of blood vessels, the vast majority of which are capillaries. A capillary is so narrow—often only 5 to 10 micrometres in diameter—that red blood cells must deform and pass through in single file to deliver oxygen to tissues. When microclots, which can range from 10 to over 200 micrometres in size, enter the microcirculation, they act as physical plugs. They do not merely slow the blood; they stop it. This leads to perfusion defects, where organs and tissues are structurally intact but functionally starving for oxygen.
##
##
Mechanisms at the Cellular Level
The formation of these microclots is not an isolated event; it is the culmination of a "perfect storm" of cellular dysfunction involving the endothelium, the immune system, and the coagulation cascade.
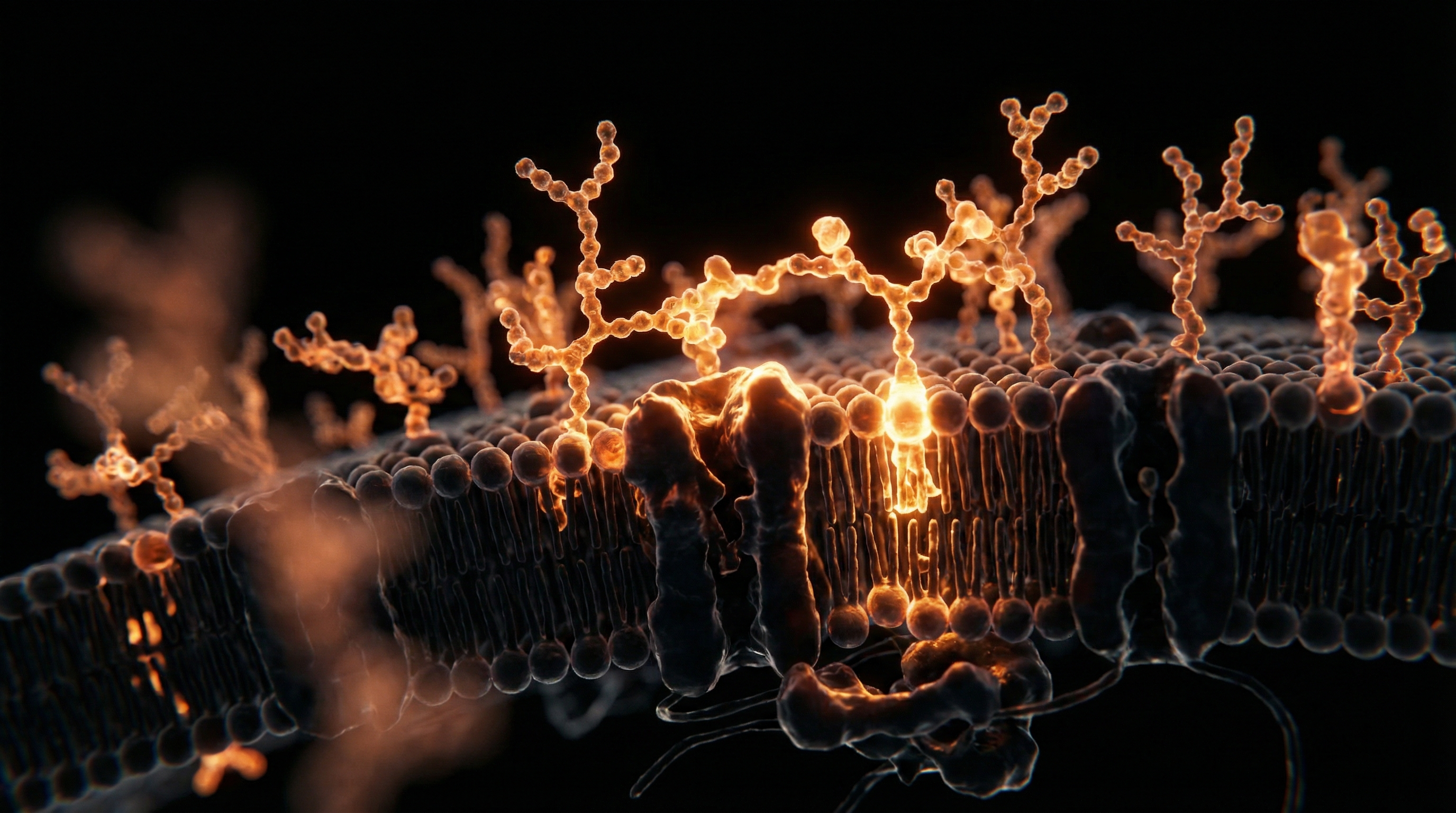
Endothelialitis and Glycocalyx Degradation
The endothelium is the single-cell layer lining every blood vessel in the body. It is protected by the endothelial glycocalyx, a delicate, hair-like forest of glycoproteins and proteoglycans that prevents blood cells from sticking to the vessel walls. Exposure to the spike protein—whether from viral infection or via the biosynthetic instructions provided by mRNA-based interventions—triggers endothelialitis (inflammation of the vessel lining). The spike protein binds to the ACE2 receptor on endothelial cells, leading to the shedding of the glycocalyx. Once this protective "non-stick" coating is lost, the underlying vessel wall becomes "sticky," promoting the adhesion of platelets and the initiation of the clotting cascade.
Platelet Hyperactivation
Under normal conditions, platelets circulate in an inactive state. However, in the presence of persistent spike protein and circulating microclots, platelets become hyperactivated. They change shape, extending pseudopodia (tentacle-like projections) and releasing pro-coagulant factors such as Platelet Factor 4 (PF4). Crucially, these microclots often contain activated platelets trapped within the fibrin mesh. These platelets continue to pump out inflammatory signals, further damaging the surrounding endothelium and creating a self-perpetuating cycle of clotting and inflammation.
The Role of Alpha-2 Antiplasmin
One of the most alarming findings in microclot research is the presence of high levels of alpha-2 antiplasmin (α2AP) within the clot structure. This molecule is a potent inhibitor of plasmin. By "locking" α2AP into the fibrin mesh, the body effectively loses its ability to dissolve the clot. This explains why the clots persist for months or years after the initial viral insult, leading to the chronic nature of the post-viral "long" syndrome.
Biological Detail: The transition from alpha-helical fibrinogen to beta-sheet fibrin is an exothermic reaction facilitated by the interaction of the spike protein’s S1 subunit with the fibrinogen D-domain. This is a direct toxic effect, independent of the immune system’s response.
##
##
Environmental Threats and Biological Disruptors
The emergence of fibrin-rich microclots does not occur in a vacuum. Modern humans are exposed to a cocktail of environmental stressors that prime the vascular system for this type of catastrophic failure.
Heavy Metals and Oxidative Stress
Trace levels of heavy metals such as lead, mercury, and cadmium, ubiquitous in the UK environment due to industrial legacy, act as catalysts for oxidative stress. These metals deplete the body’s primary antioxidant, glutathione, which is essential for maintaining the "redox" balance of the blood. In a state of high oxidative stress, fibrinogen is more prone to the misfolding that leads to amyloid formation.
Microplastics and Nanoparticles
Recent studies have identified microplastics and various nanoparticles within human blood vessels. These foreign particles can act as "nucleation sites" for microclot formation. Much like a grain of sand in an oyster creates a pearl, a nanoparticle can trigger the polymerisation of fibrin, especially when the blood is already in a pro-thrombotic state due to viral proteins.
The Impact of Modern Diets
High intake of processed seed oils (rich in linoleic acid) and refined sugars contributes to the systemic "priming" of the endothelium. High circulating levels of insulin and Advanced Glycation End-products (AGEs) damage the glycocalyx, making the vascular system more susceptible to the clotting triggers discussed above. When a person with a high-sugar, high-inflammation diet is exposed to the spike protein, the resulting microclot formation is significantly more aggressive.
##
##
The Cascade: From Exposure to Disease
The progression from initial exposure (viral or synthetic) to full-blown chronic vascular disease follows a predictable, yet often ignored, biological cascade.
- —Phase 1: Vascular Insult. The spike protein enters the bloodstream. It binds to ACE2 receptors, triggers endothelial inflammation, and begins the process of glycocalyx degradation.
- —Phase 2: Amyloidogenesis. Spike protein molecules interact directly with fibrinogen, causing it to misfold into amyloid-like fibrin. Microclots begin to form in the systemic circulation.
- —Phase 3: Microcirculatory Obstruction. These microclots are swept into the capillaries. They lodge in small vessels, particularly in highly vascularised organs such as the brain, heart, lungs, and kidneys.
- —Phase 4: Hypoxia and Mitochondrial Failure. Tissues "downstream" from the blockage receive insufficient oxygen. The mitochondria, the "powerhouses" of the cell, cannot perform oxidative phosphorylation. They switch to anaerobic metabolism, leading to a build-up of lactic acid and a profound drop in ATP (energy) production.
- —Phase 5: The Symptomatic Stage. The patient experiences Post-Exertional Malaise (PEM), brain fog (due to neuro-vascular hypoxia), and muscle pain. Because the damage is at the capillary level, standard scans and blood tests appear normal.
Callout: Without intervention, this cascade creates a state of hypoperfusion, where the patient is essentially "suffocating" at the cellular level, despite having normal blood oxygen saturation levels on a pulse oximeter.
##
##
What the Mainstream Narrative Omits
The mainstream medical narrative, largely controlled by institutional inertia and regulatory capture, continues to rely on 20th-century diagnostic tools to solve a 21st-century biological problem.
The Fallacy of the D-Dimer
The D-dimer test is the gold standard for detecting blood clots in the NHS. It works by detecting the breakdown fragments of fibrin. However, as we have established, fibrin-rich microclots in post-viral syndromes are resistant to breakdown. If the clot doesn't break down, no D-dimer fragments are produced. Consequently, a patient can have a vascular system "choked" with microclots and still return a "normal" D-dimer result. This is a catastrophic diagnostic failure that leaves patients gaslit and untreated.
The "Functional" Label
Because the pathology is microscopic, it is invisible to MRI, CT, and Ultrasound. In the absence of visible "structural" damage, the UK medical establishment often defaults to "functional" or "psychosomatic" diagnoses. Labels like "Chronic Fatigue Syndrome" or "Fibromyalgia" are frequently used as catch-all terms to avoid investigating the underlying vascular reality. This narrative omits the fact that fluorescence microscopy and Thromboelastography (TEG)—specialised tests not available in standard GP surgeries—clearly show the presence of these clots in the vast majority of Long COVID patients.
Persistent Spike Protein
The mainstream narrative maintains that the spike protein (from any source) is cleared from the body within days. However, peer-reviewed studies have found the spike protein persisting in non-classical monocytes and the vascular endothelium for 15 months or longer. This persistence provides a constant stimulus for the formation of microclots, yet this "bio-persistence" is rarely discussed in clinical guidelines.
##
##
The UK Context
In the United Kingdom, the situation is particularly acute. The NHS, while a cornerstone of British life, is a centralised bureaucracy that is slow to integrate emerging science.
NHS Guidelines and Regulatory Inertia
The National Institute for Health and Care Excellence (NICE) guidelines for Long COVID primarily focus on "symptom management" and "pacing." There is no mention of microclotting or endothelial repair in the primary care pathways. This is despite the UK being a hub for some of the world's leading researchers in this field.
The Role of the MHRA
The Medicines and Healthcare products Regulatory Agency (MHRA) is responsible for ensuring the safety of medical products in the UK. However, critics argue that the MHRA’s "Yellow Card" reporting system for adverse events is under-utilised and fails to capture the complex, delayed-onset vascular issues associated with spike protein exposure. The agency’s reliance on data from manufacturers, rather than independent microscopic blood analysis, has created a blind spot in public health surveillance.
Economic Impact
The failure to recognise microclotting as a primary driver of disability is costing the UK economy billions. Thousands of skilled professionals remain out of work, not because they are "tired," but because their brains and muscles are physiologically starved of oxygen due to microvascular obstruction. The "Great Attrition" in the UK workforce is, in many ways, a vascular crisis.
##
##
Protective Measures and Recovery Protocols
While the diagnostic landscape remains bleak within the mainstream system, biological research points toward several promising avenues for degrading these microclots and restoring vascular health.
Fibrinolytic Enzymes
The most direct way to tackle protease-resistant microclots is through the use of potent, fibrinolytic enzymes derived from fermented foods or fungi.
- —Nattokinase: An enzyme derived from the Japanese food *natto*. It has been shown in *in vitro* studies to directly degrade the SARS-CoV-2 spike protein and dissolve fibrin.
- —Serrapeptase: An enzyme originally found in silkworms, known for its ability to dissolve non-living tissue and proteinaceous debris.
- —Lumbrokinase: Derived from earthworms, this is perhaps the most potent fibrinolytic available, with a strong affinity for fibrin and the ability to break down the "locked" amyloid structures.
Support for the Glycocalyx and Endothelium
Restoring the "non-stick" coating of the blood vessels is essential to prevent new clots from forming.
- —Sulodexide: A highly purified mixture of glycosaminoglycans (including heparin-like fractions) that has shown efficacy in repairing the endothelial glycocalyx and reducing inflammation.
- —Rhamnan Sulphate: A seaweed-derived polysaccharide that has been shown to regenerate the glycocalyx and prevent spike protein binding.
Antioxidant and Anti-inflammatory Support
- —N-Acetyl Cysteine (NAC): A precursor to glutathione, NAC helps to neutralise the oxidative stress that drives fibrin misfolding. It also has mild mucolytic and anti-clotting properties.
- —Intravenous Vitamin C: High-dose Vitamin C can help restore endothelial function and act as a potent antioxidant to combat the "cytokine storm" trapped within microclots.
Diagnostic Strategies for the Proactive Patient
Since the NHS does not currently offer microclot testing, patients often seek private solutions.
- —Fluorescence Microscopy: Using thioflavin T (ThT) stains to illuminate the amyloid-like clots under a microscope.
- —TEG (Thromboelastography): A test that measures the "strength" and "breakdown time" of a clot, providing a much more accurate picture of coagulation than a standard PT/INR or D-dimer test.
Warning: Fibrinolytic protocols should always be conducted under the supervision of a qualified healthcare professional, as they involve a risk of increased bleeding and require careful monitoring of the patient's coagulation status.
##
##
Summary: Key Takeaways
The phenomenon of fibrin-rich microclots represents a major shift in our understanding of post-viral and spike-protein-induced illness. It moves the conversation away from vague "fatigue" and into the realm of concrete, measurable vascular pathology.
- —Invisible Obstructions: These microclots are amyloid-like, protease-resistant, and too small to be seen on standard medical imaging.
- —Diagnostic Gap: Standard D-dimer and routine blood tests are fundamentally flawed in their ability to detect this specific type of clotting, leading to widespread misdiagnosis and patient gaslighting.
- —Hypoxia as a Driver: The primary cause of "brain fog" and fatigue in these syndromes is cellular oxygen starvation caused by the physical blockage of the capillary beds.
- —The Spike Protein Link: Both the virus and the biosynthetic spike protein can trigger the amyloid misfolding of fibrinogen, creating a persistent "sludge" in the blood.
- —The Path Forward: Recovery requires a multi-faceted approach focused on dissolving existing microclots (via fibrinolytic enzymes), repairing the endothelial glycocalyx, and reducing systemic oxidative stress.
For the UK population, the path to health requires looking beyond the "normal" blood test results and demanding a deeper investigation into the microscopic reality of vascular health. The truth is no longer hidden in the symptoms; it is visible under the microscope, for those who choose to look.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Fibrin-Rich Microclots: Why Traditional Blood Tests Miss Post-Viral Vascular Damage"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on Spike Protein & Post-Viral Syndromes — products curated by our research team for educational relevance and biological support.

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper