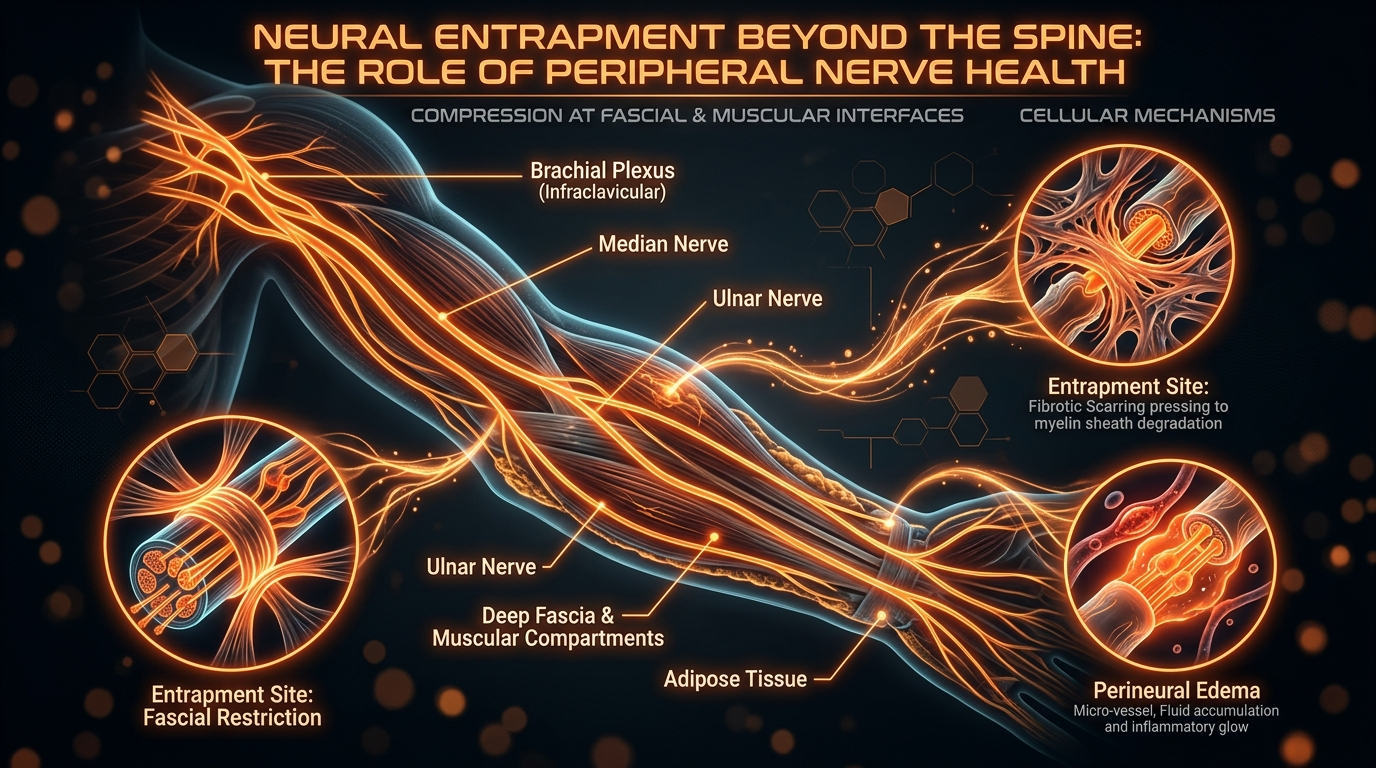
Neural Entrapment Beyond the Spine: The Role of Peripheral Nerve Health
Pain is often attributed to spinal discs while the role of peripheral nerve entrapment in the limbs is ignored. We examine how metabolic health influences the gliding capacity of nerves through musculoskeletal tunnels.
# Neural Entrapment Beyond the Spine: The Role of Peripheral Nerve Health
Overview
For decades, the architectural focus of chronic pain medicine has remained stubbornly fixated on the vertebral column. If a patient presents with radiating leg pain or tingling in the upper extremities, the diagnostic reflex is almost universally directed toward the intervertebral discs. We have become a culture obsessed with the "slipped disc," the "bulging fragment," and the "narrowed foramen." However, at INNERSTANDING, we recognise that this spinal-centric paradigm is fundamentally incomplete. While the spine is undoubtedly the gateway for the central nervous system to communicate with the periphery, it is not the only location where neural transit can be compromised.
Peripheral nerve entrapment (PNE)—the compression, constriction, or tethering of nerves as they navigate the intricate musculoskeletal tunnels of the limbs—is an under-diagnosed epidemic. It represents a failure not of the bone, but of the biological environment through which the nerve must travel. A nerve is not a static wire; it is a living, breathing, pulsing organ that requires constant movement, blood flow, and a specific biochemical milieu to function. When we ignore the health of the peripheral nerve in favour of the spine, we miss the "Double Crush" phenomena and the metabolic underpinnings of why nerves become "sticky" and prone to entrapment.
This article serves as a comprehensive interrogation of the peripheral nervous system. We will move beyond the structural obsession of the MRI and look into the cellular mechanics of nerve gliding, the metabolic disruptors that turn healthy fascia into restrictive "glue," and why the modern British lifestyle is a perfect storm for neural ischaemia. To understand chronic pain, one must understand that the nerve is only as healthy as the tunnel through which it glides.
In the United Kingdom, chronic pain affects between 33% and 50% of the adult population, yet a staggering proportion of these cases are managed with generic analgesics without ever identifying the specific site of peripheral entrapment beyond the spine.
##
The Biology — How It Works
To comprehend neural entrapment, one must first appreciate the remarkable mechanical requirements of a peripheral nerve. As you move your arm or leg, your nerves must undergo significant excursion—they must slide and stretch through anatomical tunnels formed by bone, muscle, and fascia. For example, the ulnar nerve at the elbow must lengthen by nearly 20% as the joint moves from extension to flexion. This is achieved through a combination of internal elastic recoil and external gliding.
The Anatomy of the Sliding Apparatus
A peripheral nerve is encased in several layers of connective tissue, each serving a vital protective and mechanical role:
- —The Epineurium: The outermost layer of dense irregular connective tissue. It protects the nerve from external pressure and contains the major blood vessels (vasa nervorum). Crucially, the "sliding surface" exists between the epineurium and the surrounding fascia.
- —The Perineurium: This layer surrounds bundles of nerve fibres (fascicles). It acts as a highly specialised blood-nerve barrier, maintaining the internal pressure and chemical environment necessary for signal conduction.
- —The Endoneurium: A delicate layer of connective tissue surrounding each individual axon and its Schwann cells.
When we speak of neural entrapment, we are rarely talking about a nerve being "crushed" in the way a vice crushes a pipe. Instead, we are discussing the loss of the nerve's ability to glide. If the epineurium becomes fibrotic or if the surrounding interstitial fluid becomes viscous due to metabolic dysfunction, the nerve becomes "tethered." Every time the limb moves, instead of sliding smoothly, the nerve is pulled and micro-traumatised.
The Concept of the "Double Crush"
One of the most significant biological insights in peripheral nerve health is the Double Crush Syndrome. This hypothesis posits that a minor compression of a nerve at its proximal point (the spine) makes the rest of the nerve significantly more vulnerable to compression at distal points (the wrist, elbow, or ankle). This happens because the flow of vital nutrients and proteins from the cell body in the spinal cord—known as axoplasmic flow—is disrupted. Even a 10% reduction in flow at the neck can render the median nerve at the wrist incapable of repairing itself from daily wear and tear, leading to Carpal Tunnel Syndrome that "mysteriously" refuses to heal.
The Tunnels of Transit
Nerves pass through numerous "choke points" in the body. The thoracic outlet (at the base of the neck), the cubital tunnel (at the elbow), the carpal tunnel (at the wrist), the fibular tunnel (at the knee), and the tarsal tunnel (at the ankle) are all critical transit zones. These are not just spaces; they are highly regulated biological environments. In a healthy state, these tunnels are lubricated and spacious. In a diseased state, they become sites of chronic inflammation and mechanical friction.
##
Mechanisms at the Cellular Level
To truly understand why a nerve becomes entrapped, we must look past the gross anatomy and into the microscopic world of cellular metabolism. The nerve is an incredibly "expensive" organ in terms of energy consumption. Although the nervous system accounts for only 2% of body weight, it consumes roughly 20% of the body's oxygen and glucose.
Axoplasmic Flow: The Internal Conveyor Belt
Inside every nerve fibre is a continuous stream of cytoplasm called axoplasm. This fluid carries mitochondria, neurotransmitters, and repair proteins from the cell body to the very tip of the nerve. This transport system is powered by molecular motors (kinesin and dynein) that "walk" along microtubules. Metabolic health is the fuel for these motors. When insulin resistance or systemic inflammation occurs, the production of ATP (adenosine triphosphate) in the mitochondria is compromised. The motors slow down. The "conveyor belt" stutters. This results in a nerve that is structurally intact but functionally starving, making it hypersensitive to the slightest mechanical pressure.
The Vasa Nervorum and Ischaemia
Nerves are supplied with blood by a microscopic network of vessels called the vasa nervorum. These vessels are uniquely sensitive to mechanical pressure. Even a slight increase in pressure within a musculoskeletal tunnel—caused by oedema (swelling) or fibrotic thickening of the fascia—can occlude these tiny vessels. When the blood supply is cut off, the nerve enters a state of ischaemia. The lack of oxygen causes the sodium-potassium pumps on the nerve membrane to fail. This leads to a build-up of sodium inside the nerve, causing it to swell from the inside out (endoneurial oedema). This swelling further increases the pressure within the tunnel, creating a vicious cycle of ischaemia and inflammation that is a hallmark of chronic entrapment syndromes.
Advanced Glycation End-products (AGEs) and "Sticky" Nerves
One of the most overlooked factors in peripheral nerve health is the role of blood sugar and glycation. When blood glucose levels are chronically elevated—even at "pre-diabetic" levels—sugar molecules begin to bond non-enzymatically to proteins in the nerve and the surrounding fascia. This process creates Advanced Glycation End-products (AGEs). AGEs act like biological "superglue." They cross-link collagen fibres in the epineurium and the surrounding connective tissue, making them stiff, brittle, and adhesive. This is why individuals with metabolic dysfunction often report "all-over" stiffness. Their nerves are literally being glued to the surrounding muscles, preventing the essential gliding motion required for pain-free movement.
Data from UK clinical trials suggest that patients with HbA1c levels in the upper "normal" range (39-42 mmol/mol) are significantly more likely to develop peripheral nerve compression symptoms than those in the lower range, highlighting the role of sub-clinical metabolic dysfunction.
##
Environmental Threats and Biological Disruptors
The modern environment is hostile to the delicate mechanics of the peripheral nervous system. While evolution designed our nerves to be resilient, it did not account for the biological insults of the 21st century.
Nutritional Toxicity and Linoleic Acid
The shift in the British diet toward ultra-processed foods has introduced high concentrations of Omega-6 industrial seed oils (sunflower, rapeseed, soybean). These oils are high in linoleic acid, which can accumulate in the phospholipid membranes of nerve cells. When these fats oxidise, they create toxic by-products like 4-HNE (4-Hydroxynonenal), which directly damage the nerve's DNA and mitochondria. This lipid peroxidation makes the nerve membrane "leaky" and hyper-irritable, lowering the threshold for pain signals.
The Sedentary Stagnation
Nerves require movement to maintain their health. The act of moving a limb creates a "pumping" effect that facilitates the drainage of metabolic waste from the nerve's interstitial space. The modern "desk-bound" lifestyle, common in the UK's service-based economy, creates static ischaemia. By sitting in a fixed position for eight hours, we compress the sciatic nerve and the various nerves of the brachial plexus, not with high force, but with *persistent* force. This long-term, low-grade compression is often more damaging than a single acute injury because it prevents the tissue from ever entering the "recovery" phase of the inflammatory cycle.
Environmental Toxins and Heavy Metals
Peripheral nerves are often the first victims of environmental toxicity. Substances like lead, mercury (often from old dental amalgams), and certain pesticides act as neurotoxins that disrupt the delicate microtubule structure within the axon. This disruption mimics the effects of mechanical entrapment by halting axoplasmic flow. At INNERSTANDING, we often find that what is diagnosed as "unexplained" peripheral neuropathy is actually a combination of mild mechanical entrapment and a high toxic load that has rendered the nerve incapable of maintaining its protective sheath.
##
The Cascade: From Exposure to Disease
The progression from a healthy, gliding nerve to a chronically entrapped, painful one follows a predictable biological cascade. Understanding this sequence is vital for early intervention.
Stage 1: The Functional Block
Initially, the entrapment is purely mechanical. A tight muscle or a slightly swollen joint puts pressure on a nerve. The patient might feel "pins and needles" or "heaviness" after a period of activity. At this stage, there is no permanent damage to the nerve fibres. The symptoms are caused by transient ischaemia. If the pressure is removed, the nerve recovers almost instantly.
Stage 2: Endoneurial Oedema
If the pressure persists, the vasa nervorum remains occluded. The lack of oxygen leads to a breakdown of the blood-nerve barrier. Fluid begins to leak into the endoneurium (the innermost compartment of the nerve). Because the perineurium is a tough, inelastic membrane, the pressure inside the nerve rises. This is the stage where "night pain" begins. As you sleep, your blood pressure drops and your lymphatic drainage slows, causing the already-swollen nerve to become even more congested.
Stage 3: Fibrosis and Tethering
This is the most critical stage. Chronic inflammation triggers the recruitment of fibroblasts, which begin to lay down excess collagen within the nerve and around the epineurium. The nerve begins to scar. This is where the nerve loses its "excursion" capacity. It is now physically stuck to the side of the tunnel. At this point, even movements that are far away from the site of entrapment can cause pain. A person with an entrapped median nerve at the wrist might feel pain in their shoulder when they reach for a door handle because the nerve is being yanked from the top down.
Stage 4: Wallerian Degeneration
In the final stage, the physical compression and the lack of nutrients lead to the death of the axons distal to the site of entrapment. The myelin sheath—the fatty insulation of the nerve—begins to break down. This results in permanent muscle weakness, sensory loss, and the development of neuropathic pain, where the brain interprets the "dying" signals from the nerve as intense burning or electric shocks.
It is estimated by the UK's Office for National Statistics (ONS) that musculoskeletal issues, including nerve entrapment, are the primary cause of work-related absences, costing the UK economy over £15 billion annually in lost productivity.
##
What the Mainstream Narrative Omits
The mainstream medical approach to nerve pain is riddled with blind spots. At INNERSTANDING, we believe it is essential to expose these omissions to allow patients to take control of their biological destiny.
The MRI Red Herring
The biggest failure of the mainstream narrative is the over-reliance on MRI scans of the spine. Studies have shown that up to 50% of people *without any pain* have "abnormal" findings on a spinal MRI, such as disc bulges or stenosis. When a patient with leg pain has an MRI that shows a small bulge, the doctor often stops looking. They ignore the fact that the pain might actually be coming from the fibular nerve being compressed at the knee or the tibial nerve in the tarsal tunnel. This leads to thousands of unnecessary spinal surgeries in the UK every year—surgeries that fail to provide relief because the "generator" of the pain was never in the spine to begin with.
The Failure of "Pain Management"
Mainstream medicine treats nerve pain with "management" rather than "resolution." Drugs like Gabapentin and Pregabalin are designed to dampen the central nervous system's response to pain signals. They do absolutely nothing to address the biological cause of the nerve's distress. They don't improve blood flow to the vasa nervorum; they don't reduce AGE-related fibrosis; and they don't restore axoplasmic flow. They are pharmacological earplugs that allow the patient to ignore a fire that is still burning.
The Fascial Connection
Mainstream anatomy often treats nerves, muscles, and fascia as separate systems. In reality, they are a single, integrated continuum. The "tunnels" we speak of are made of fascia. If a patient's fascia is dehydrated or pathologically cross-linked due to a high-sugar diet, the nerve *cannot* be healthy. Traditional physiotherapy often focuses on strengthening muscles, but if you strengthen a muscle that is already compressing a "stuck" nerve, you often make the problem worse. The focus must shift to the health of the interstitial space.
##
The UK Context
The United Kingdom presents a unique set of challenges regarding peripheral nerve health. The NHS model, while designed for acute care, is notoriously ill-equipped to handle the nuances of chronic neural entrapment.
The "Wait and See" Trap
In the UK, the standard pathway for nerve-related pain often involves months of waiting for a specialist appointment, during which time the patient is prescribed "conservative management" (usually ibuprofen and rest). However, as we have seen in the "Cascade" section, nerves do not respond well to static rest. By the time a UK patient sees a neurologist or a surgeon, their nerve may have progressed from Stage 1 (reversible) to Stage 3 (fibrotic).
The Diet-Pain Link in Britain
The UK has some of the highest rates of metabolic dysfunction in Europe. With the prevalence of type 2 diabetes and pre-diabetes soaring, the "metabolic substrate" for nerve entrapment is becoming more common. The British diet, traditionally high in refined carbohydrates and increasingly reliant on processed fats, is a primary driver of the AGEs and systemic inflammation that render peripheral nerves vulnerable to entrapment.
The Climate Factor
The damp, cool climate of the UK can exacerbate peripheral nerve symptoms. Cold temperatures cause vasoconstriction, which further reduces the blood supply to already-compromised nerves. Many patients in the UK report that their "entrapment" symptoms worsen in the winter months—not because their spine has changed, but because the peripheral blood flow to their limbs has diminished.
According to Arthritis Research UK, approximately 1 in 4 people in the UK live with a musculoskeletal condition. A significant, yet unquantified, percentage of these individuals are suffering from "occult" nerve entrapments that mimic joint or muscle pain.
##
Protective Measures and Recovery Protocols
Recovery from peripheral nerve entrapment requires a multi-faceted biological approach. We must address the mechanical obstruction, the metabolic environment, and the cellular health of the nerve itself.
1. Metabolic Optimisation: Removing the "Glue"
The first step in any recovery protocol is to address the biochemical drivers of fibrosis.
- —Glucoregulation: Reducing blood sugar levels is non-negotiable. By lowering HbA1c, you reduce the formation of Advanced Glycation End-products (AGEs), allowing the fascia and epineurium to regain their elasticity. A ketogenic or low-carbohydrate approach is often the fastest way to achieve this.
- —Elimination of Seed Oils: Removing linoleic acid-rich oils reduces the oxidative stress on the nerve membranes, allowing the vasa nervorum to heal and the mitochondria to produce ATP more efficiently.
- —Hydration and Electrolytes: Nerves are highly sensitive to the balance of sodium, potassium, and magnesium. Proper hydration—with added minerals—is essential for maintaining the "fluidity" of the interstitial spaces.
2. Neural Flossing and Gliding
Static stretching is often detrimental to an entrapped nerve. Instead, we advocate for neural flossing. This involves moving a limb in a way that pulls the nerve from one end while relaxing it at the other, effectively "sawing" it back and forth through its tunnel. This mechanical motion helps to break down minor adhesions and "pumps" out stagnant inflammatory fluid from the endoneurial space.
3. Targeted Supplementation
Certain nutrients have a high affinity for peripheral nerve repair:
- —Alpha-Lipoic Acid (ALA): A potent antioxidant that has been shown in clinical trials to improve blood flow to the nerves and reduce the symptoms of peripheral neuropathy.
- —Benfotiamine: A fat-soluble form of Vitamin B1 (Thiamine). It is uniquely effective at blocking the pathways that lead to AGE formation, protecting the nerve from sugar-induced damage.
- —Acetyl-L-Carnitine: Supports mitochondrial function within the nerve, providing the energy needed for axoplasmic flow and repair.
- —B-Complex (Active Forms): Methylcobalamin (B12) and Pyridoxal-5-Phosphate (B6) are essential for the maintenance of the myelin sheath.
4. Environmental and Lifestyle Adjustments
- —Thermal Therapy: Using heat on the site of a potential entrapment (like the elbow or wrist) can facilitate vasodilation, bringing much-needed oxygen to the vasa nervorum.
- —Ergonomic Variety: The key is not a "perfect" posture, but constant movement. UK workers should aim for "movement snacks" every 30 minutes to prevent the static ischaemia associated with sitting.
- —Sleep Position: Many entrapments are exacerbated by sleeping with limbs in extreme flexion (e.g., sleeping with elbows tucked tight). Using pillows or soft splints to maintain "neutral" joint positions at night can drastically reduce endoneurial oedema.
##
Summary: Key Takeaways
The path to resolving chronic pain lies in looking beyond the spine and understanding the holistic biology of the peripheral nervous system. The nerve is not a passive structure; it is a dynamic, energy-hungry organ that demands movement and metabolic clarity.
- —Nerves must glide, not just exist. If a nerve loses its ability to slide through its anatomical tunnels due to fibrosis or inflammation, pain is inevitable.
- —Metabolic health is the foundation of neural health. High blood sugar and toxic fats create "sticky" nerves through the formation of AGEs and oxidative stress.
- —The "Double Crush" is real. A minor issue in the neck or back can sensitise the entire length of a nerve, making distal entrapments (like Carpal Tunnel) more likely.
- —Mainstream diagnostics are often misleading. An MRI of the spine does not rule out peripheral entrapment in the limbs. Clinical examination and an understanding of "choke points" are superior.
- —The UK's lifestyle and medical model often fail nerve patients. Delayed intervention and a focus on pharmacological "management" allow reversible conditions to become chronic.
- —Recovery is possible. Through a combination of metabolic optimisation, neural flossing, and targeted nutritional support, even long-standing entrapments can be resolved by restoring the biological environment the nerve needs to thrive.
The mission of INNERSTANDING is to empower the individual with the scientific truth that the body is an interconnected system. Peripheral nerve health is not a niche concern; it is a fundamental pillar of human movement and freedom from pain. We must stop blaming the discs for the sins of the tunnels. It is time to free the nerves.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Neural Entrapment Beyond the Spine: The Role of Peripheral Nerve Health"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper