NMDA Receptor Antagonism: The Frontier of Refractory Pain Management
The NMDA receptor plays a pivotal role in the 'wind-up' phenomenon of chronic pain. Targeting these receptors offers a way to reset the nervous system's gain control, though many effective protocols remain under-utilised in the UK.
Overview
The landscape of modern medicine is currently grappling with a silent, pervasive epidemic: the crisis of refractory chronic pain. In the United Kingdom alone, millions of individuals exist in a state of "permanent alarm," where the initial physiological signal of injury has long since passed, yet the perception of agony remains—and often intensifies. This is not a failure of the patient’s willpower, nor is it merely a psychological manifestation. It is a fundamental, structural, and electro-chemical failure of the central nervous system’s "gain control." At the heart of this malfunction lies a single, sophisticated molecular gatekeeper: the N-methyl-D-aspartate (NMDA) receptor.
For decades, the mainstream clinical approach to pain has been dominated by the "Opioid Model"—a strategy of suppression that targets mu-opioid receptors to dampen the perception of pain. While effective for acute trauma and end-of-life care, this model has proven catastrophically inadequate for chronic, refractory conditions. In many cases, prolonged opioid use actually facilitates a phenomenon known as Opioid-Induced Hyperalgesia (OIH), where the patient becomes *more* sensitive to pain over time. The frontier of pain science has moved beyond suppression; we are now entering the era of "recalibration."
NMDA receptor antagonism represents the most promising biological "reset button" available to modern medicine. By targeting the NMDA receptor (NMDAR), researchers and forward-thinking clinicians are finding ways to interrupt the "wind-up" phenomenon—a state of pathological neuroplasticity where the spinal cord and brain become hyper-excitable. This article explores the deep biological architecture of the NMDAR, the environmental factors that are causing a widespread "unplugging" of our natural inhibitory systems, and the sophisticated pharmacological protocols that remain tragically under-utilised within the British National Health Service (NHS).
Over 28 million adults in the UK are estimated to be living with some form of chronic pain, representing nearly 43% of the population. Despite this, specialized NMDA-targeted interventions like ketamine infusions or memantine protocols are available to fewer than 0.5% of these patients.
To understand why chronic pain is so difficult to treat, one must understand that the nervous system is not a static set of wires. It is a dynamic, plastic organ that learns. Unfortunately, it can "learn" pain. This article serves as a deep-dive into the mechanism of that learning and the biological tools required to unlearn it.
##
The Biology — How It Works
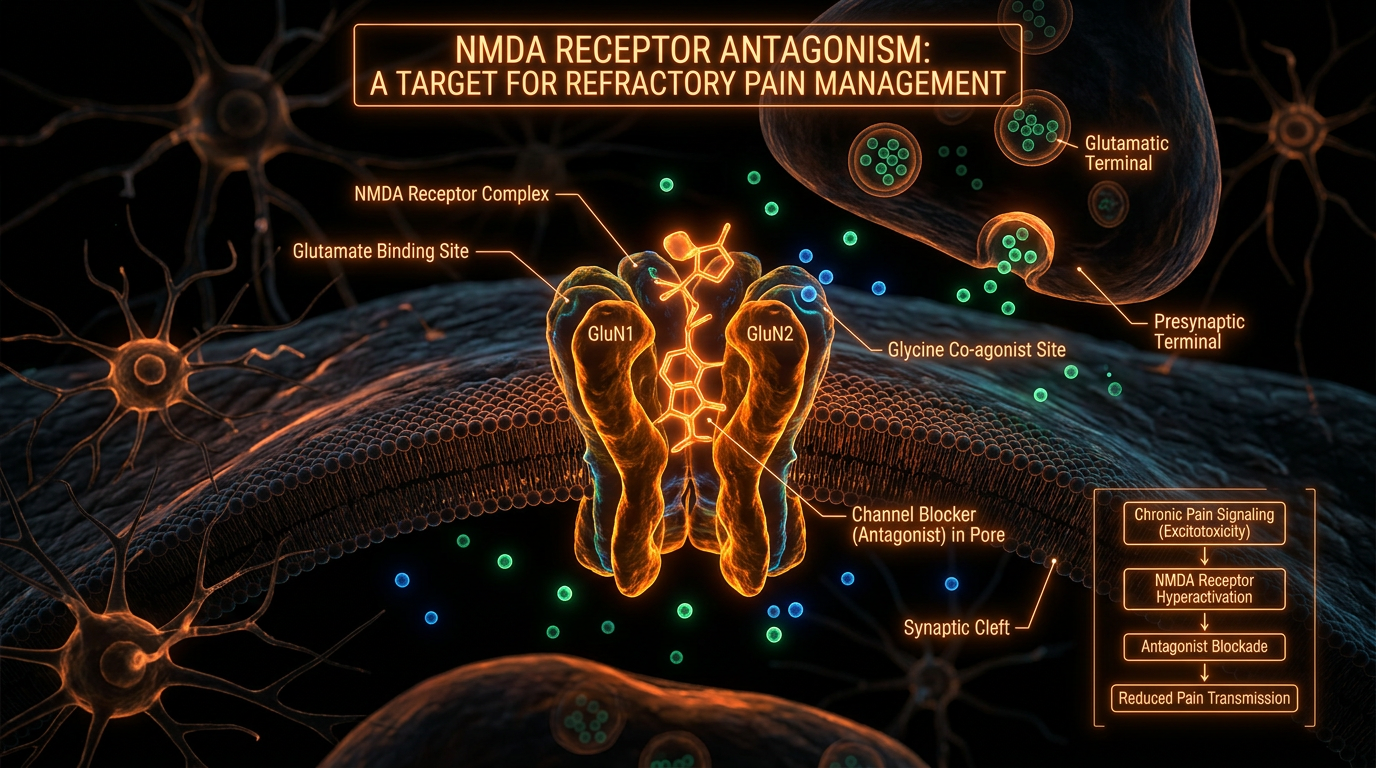
The NMDA receptor is a glutamate-gated cation channel, but it is unique among its peers (such as the AMPA or Kainate receptors) because it is both ligand-gated and voltage-dependent. This dual-requirement makes it a "coincidence detector"—a biological logic gate that only opens when specific conditions are met. Under normal physiological conditions, the NMDAR is effectively "plugged" by a magnesium ion ($Mg^{2+}$). This magnesium plug serves as the nervous system's primary safety catch, preventing the uncontrolled influx of calcium into the neuron.
In a healthy state, brief flashes of glutamate (the body’s primary excitatory neurotransmitter) activate the faster AMPA receptors. This allows for normal signal transmission—the kind that tells you your shoe is tied too tight or that you’ve touched a hot cup. The NMDA receptor remains silent because the magnesium ion stays firmly in place, blocked by the negative electrical potential of the cell's interior.
However, when a pain signal becomes persistent—due to chronic injury, inflammation, or repeated nerve trauma—the AMPA receptors fire so frequently that the post-synaptic membrane becomes partially depolarised. This change in electrical charge repels the positively charged magnesium ion, literally "unplugging" the NMDA receptor. Once the plug is removed, the floodgates open. Calcium ($Ca^{2+}$) and sodium ($Na^{+}$) pour into the neuron, while potassium ($K^{+}$) flows out.
This calcium influx is the "Holy Grail" of chronic pain biology. Calcium is not just an ion; it is a powerful intracellular signalling molecule. It triggers a cascade of second messengers that tell the neuron to "turn up the volume." It increases the number of AMPA receptors on the surface, making the cell even more sensitive to glutamate. It triggers the expression of genes that physically remodel the synapse. This is the "wind-up" phenomenon. The system has shifted from a state of transient signalling to a state of permanent amplification.
The Heterotetrameric Structure
The NMDAR is not a single protein but a complex assembly, typically a heterotetramer composed of two GluN1 subunits and two GluN2 (A, B, C, or D) or GluN3 subunits. The specific composition of these subunits determines the receptor's kinetic properties—how long it stays open, how sensitive it is to magnesium, and how much calcium it lets through.
In the context of refractory pain, the GluN2B subunit is of particular interest. It is associated with longer channel-open times and is found in high concentrations in the dorsal horn of the spinal cord—the primary processing station for pain signals. When the GluN2B-containing NMDARs are over-activated, they facilitate "Long-Term Potentiation" (LTP) of pain pathways. In simple terms, the spinal cord develops a "memory" of the pain. Even after the original tissue damage has healed, the NMDARs remain in a state of hyper-readiness, firing at the slightest provocation.
The Role of Glycine and D-Serine
It is often overlooked that glutamate alone cannot open the NMDAR. It requires a co-agonist, either glycine or D-serine, to bind to the GluN1 subunit. This adds another layer of control. In the modern environment, shifts in our neurochemistry—often driven by gut dysbiosis or chronic inflammatory states—can lead to an overabundance of these co-agonists. This lowers the threshold for NMDA activation, effectively making our nervous system "leaky" and more prone to the transition from acute to chronic pain.
##
Mechanisms at the Cellular Level
When we zoom into the synapse of a patient suffering from refractory pain, we see a battlefield of molecular signalling. The persistent activation of NMDARs leads to a state known as central sensitisation. This is the process where the central nervous system (CNS) enters a state of high reactivity.
The intracellular calcium influx triggered by NMDAR activation activates several key enzymes:
- —Protein Kinase C (PKC): This enzyme phosphorylates the NMDA receptor itself, further reducing its affinity for the magnesium plug. This creates a vicious feedback loop: the more the receptor fires, the easier it becomes to fire again.
- —Nitric Oxide Synthase (NOS): Calcium activates the production of Nitric Oxide (NO). NO is a gas that can diffuse *backwards* across the synapse to the pre-synaptic neuron, telling it to release even more glutamate. This "retrograde signalling" ensures that the pain signal is reinforced from both sides of the synaptic gap.
- —Calm-Kinase II: This leads to the "trafficking" of more AMPA receptors to the membrane, increasing the density of excitatory "antennas" on the neuron.
Epigenetic Remodelling
Beyond immediate enzymatic changes, chronic NMDA activation reaches deep into the nucleus of the neuron. It triggers the phosphorylation of CREB (cAMP response element-binding protein), a transcription factor that regulates the expression of genes involved in synaptic plasticity. This results in the production of Brain-Derived Neurotrophic Factor (BDNF) in the spinal cord.
While BDNF is often hailed as "Miracle-Gro for the brain" in the context of learning and memory, in the spinal pain pathways, it is a disaster. It causes a functional "rewiring" of the dorsal horn. Neurons that normally carry light touch signals (A-beta fibres) begin to cross-wire with pain-carrying neurons (C-fibres). This results in allodynia—a condition where a breeze on the skin or the touch of a shirt is perceived by the brain as searing, burning pain. The hardware of the nervous system has been physically altered.
Glial Cell Involvement
We must also consider the role of the "non-neuronal" cells: the microglia and astrocytes. For a long time, these were thought to be mere structural support. We now know they are active participants in NMDA-mediated pain. When NMDARs on neurons fire excessively, they release "danger signals" (like ATP and Fractalkine) that activate nearby microglia. These activated immune cells then release pro-inflammatory cytokines like IL-1β and TNF-alpha.
These cytokines have a direct effect on the NMDAR: they increase its conductance. Thus, a "neuro-inflammatory soup" is created. The pain is no longer just an electrical issue; it is an immunological one. This is why refractory pain often feels like a "flu of the nervous system," accompanied by fatigue, brain fog, and systemic sensitivity.
##
Environmental Threats and Biological Disruptors
In the "INNERSTANDING" view of biology, we must ask: why is the modern human so susceptible to this NMDA-driven breakdown? The answer lies in the systematic degradation of our biological buffers. The NMDA receptor is a finely tuned instrument that requires a specific environmental and internal milieu to function correctly. We are currently living in an environment that is "pro-NMDA" and "anti-magnesium."
The Magnesium Crisis
As established, magnesium is the natural antagonist of the NMDA receptor. Without sufficient intracellular magnesium, the NMDAR safety catch is permanently off. However, UK soil surveys have shown a decline in mineral content of up to 40% since the 1940s. Intensive farming practices prioritize yield and calorie count over mineral density. Furthermore, the modern British diet—rich in processed grains and refined sugars—is naturally low in magnesium.
According to data from the National Diet and Nutrition Survey (NDNS), approximately 80% of UK adults are failing to meet the Reference Nutrient Intake (RNI) for magnesium. This creates a "population-level" vulnerability to central sensitisation and chronic pain syndromes.
Furthermore, certain lifestyle factors actively deplete magnesium. Chronic stress triggers the release of catecholamines (adrenaline and noradrenaline), which cause the kidneys to excrete magnesium at an accelerated rate. This is the "Stress-Pain Cycle": stress leads to magnesium loss, which leads to NMDA disinhibition, which leads to increased pain, which causes more stress.
Excitotoxins in the Food Supply
The modern food environment is saturated with "excitotoxins"—compounds that mimic or enhance the action of glutamate. Monosodium Glutamate (MSG) and its various aliases (yeast extract, hydrolysed vegetable protein) are pervasive. While the blood-brain barrier is designed to protect the CNS from systemic glutamate, chronic inflammation and "leaky gut" can compromise this barrier. When excess dietary glutamate reaches a sensitised nervous system, it acts like fuel on a fire, directly stimulating the NMDARs that are already lacking their magnesium plugs.
Circadian Disruption and Blue Light
The NMDA receptor's activity is modulated by the circadian rhythm. Melatonin, the hormone of sleep, has been shown to have inhibitory effects on NMDA-mediated calcium influx. Conversely, the "blue light" environment of modern Britain—pervasive LED lighting and screen use—suppresses melatonin production. This leaves the nervous system "electrically naked" at night, a time when the body should be down-regulating excitatory activity to allow for synaptic "pruning" and recovery. Without this nightly reset, the "wind-up" of the day’s pain signals is never fully unwound.
##
The Cascade: From Exposure to Disease
The journey from a healthy individual to a patient with refractory pain is a predictable biological cascade. Understanding this sequence is vital for intervention, as each stage offers a different window for NMDA-targeted therapy.
- —The Insult: An initial injury occurs. This could be a surgical incision, a viral infection (as seen in Long-COVID), or a mechanical trauma.
- —The Acute Surge: Glutamate is released in massive quantities at the site of the injury and in the spinal cord. AMPA receptors fire rapidly.
- —The Plug Displacement: If the pain is intense or prolonged, the magnesium plug is displaced from the NMDAR. The "gate" is now open.
- —The Calcium Flood: Intracellular calcium levels spike. This initiates the enzymatic cascades (PKC, NOS) described earlier.
- —The Reinforcement (Wind-up): The neuron becomes hyper-excitable. "Silent synapses" are awakened. The threshold for firing drops.
- —Central Sensitisation: The "wind-up" spreads from the local site to the entire spinal segment and eventually to the thalamus and cortex. The patient now feels pain in areas far removed from the original injury.
- —Systemic Failure: The constant state of "alarm" leads to HPA-axis (Hypothalamic-Pituitary-Adrenal) exhaustion. The descending inhibitory pathways—the body’s natural opioid and serotonergic "brakes"—fail.
- —Refractory State: The pain is now self-sustaining. It no longer requires an external stimulus. This is the state of most Fibromyalgia, CRPS (Complex Regional Pain Syndrome), and phantom limb pain sufferers.
In the UK, the medical system typically intervenes at Stage 7 or 8, usually with antidepressants or high-dose opioids. By this point, however, the "hardware" is already rewritten. Trying to stop the pain with opioids is like trying to put out a forest fire by turning off the smoke alarm. The fire (NMDA over-activation) continues to burn underneath.
##
What the Mainstream Narrative Omits
The mainstream medical narrative in the UK often frames chronic pain as a "management" problem rather than a "curable" or "reversible" physiological state. This is a profound omission. By ignoring the NMDA receptor's role in neuroplasticity, the standard care model condemns millions to a lifetime of chemical palliation.
The Opioid Trap
Mainstream medicine has been slow to acknowledge the "dark side" of mu-opioid agonists. While they provide short-term relief, opioids actually *stimulate* the NMDA receptor through a variety of pathways. Morphine-3-glucuronide, a metabolite of morphine, is known to be neuro-excitatory. This is why many patients find that their pain becomes wider and more "vibrant" after years of opioid therapy. The drugs intended to soothe the system are actually reinforcing the very NMDA-driven pathways that cause the pain.
The Profitability of Suppression
There is an uncomfortable economic reality: NMDA antagonists like ketamine, memantine, and magnesium are either off-patent, incredibly cheap, or naturally occurring. There is little incentive for a pharmaceutical company to fund the massive Phase III trials required to change NICE (National Institute for Health and Care Excellence) guidelines for "refractory pain." It is far more profitable to continue the cycle of patented, slightly modified opioid or gabapentinoid medications.
The Psychology Fallacy
When biological treatments fail, the mainstream narrative often shifts the blame to the patient’s "psychology." Patients are told they have "centralised" their pain and are offered Cognitive Behavioural Therapy (CBT). While CBT can help with the *coping* aspect of chronic pain, it does nothing to re-insert the magnesium plug into the NMDAR. Framing a molecular ion-channel failure as a "faulty thinking" problem is a form of medical gaslighting that ignores the hard science of neuroplasticity.
##
The UK Context
The situation in the United Kingdom is unique and, in many ways, more challenging than in other developed nations. The NHS, while an incredible institution for acute care, is structurally resistant to the "frontier" treatments required for NMDA-driven refractory pain.
The Postcode Lottery
Access to NMDA antagonists like Ketamine is a "postcode lottery." Some forward-thinking trusts in London or Oxford have established "Ketamine Clinics" for refractory pain, but these are rare. In the North of England—areas like Blackpool, Middlesbrough, and Hull—opioid prescription rates remain among the highest in Europe, and access to NMDA-targeted interventions is almost non-existent.
Recent data indicates that the North-South divide in the UK extends to pain management. Patients in the most deprived deciles are nearly 3 times more likely to be prescribed a high-dose opioid than those in the least deprived, yet they are 5 times less likely to be offered NMDA-targeted therapies or multidisciplinary "reset" protocols.
NICE and the "Evidence" Gap
The NICE guidelines are notoriously slow to adapt. They require a specific level of "gold standard" evidence that is difficult to produce for off-patent drugs. Consequently, doctors who wish to prescribe Memantine (an Alzheimer's drug) for chronic pain must do so "off-label," which carries a burden of liability and administrative hurdle that many GPs are unwilling to take on. This results in a "clinical inertia" where the safest, most effective pharmacological "reset" buttons remain locked behind red tape.
The Stigma of Ketamine
Ketamine is perhaps the most potent NMDA antagonist we possess. It has the ability to "de-sensitise" the spinal cord and "re-boot" the brain's pain processing centres. However, in the UK, its reputation as a "horse tranquiliser" or a "club drug" has created a profound cultural stigma within the medical establishment. This prevents its use in sub-anaesthetic, controlled doses for pain, even though the safety profile for these doses is well-established.
##
Protective Measures and Recovery Protocols
If we accept that NMDA over-activation is the core driver of refractory pain, our goal must be two-fold: Protection (keeping the magnesium plug in) and Recovery (re-establishing the nervous system's gain control).
Pharmacological Antagonism
Several substances can act as NMDA antagonists, each with different strengths and clinical applications:
- —Ketamine: Used in sub-anaesthetic doses (often via IV infusion or topical cream), it provides a "chemical holiday" for the nervous system, allowing NMDARs to reset and "re-plug."
- —Memantine: A moderate-affinity, uncompetitive NMDA antagonist. Unlike ketamine, it can be taken orally and has a long half-life. It is particularly effective at "filtering" out background pain noise while allowing normal signalling to pass.
- —Dextromethorphan (DXM): Often found in cough syrups, at specific doses, it acts as a weak NMDA antagonist. It is sometimes used as an "adjunct" to make opioids more effective and prevent tolerance.
- —Agmatine Sulfate: A metabolite of the amino acid L-arginine, agmatine is a natural NMDA antagonist and nitric oxide inhibitor. It has shown immense promise in animal studies for reversing neuropathic pain.
The Magnesium Protocol
Restoring the magnesium plug is the first step in any recovery protocol. However, not all magnesium is created equal.
- —Magnesium Threonate: This form is specifically designed to cross the blood-brain barrier, making it the superior choice for targeting NMDARs in the CNS.
- —Magnesium Glycinate/Malate: High bioavailability forms for systemic support.
- —Topical Magnesium (Transdermal): Magnesium chloride flakes in a bath can bypass the digestive system, providing immediate systemic relaxation and NMDA damping.
Recommendation: For chronic pain sufferers, a daily elemental magnesium intake of 400-600mg is often required, but this must be titrated slowly to avoid gastrointestinal distress.
Nutritional Interventions
- —Eliminate Excitotoxins: A strict elimination of MSG, aspartame, and "hydrolysed" proteins is essential. This reduces the "glutamate load" on the sensitised receptors.
- —Anti-inflammatory Focus: High-dose Omega-3 fatty acids (EPA/DHA) and curcumin help to calm the glial cells, reducing the "neuro-inflammatory soup" that keeps NMDARs hyper-active.
- —The Ketogenic Influence: A ketogenic diet has been shown to increase the levels of GABA (the brain’s primary inhibitory neurotransmitter) and reduce glutamate, naturally shifting the balance away from NMDA over-activity.
Lifestyle and Neuromodulation
- —HRV Training: High Heart Rate Variability (HRV) is a marker of vagal tone. The vagus nerve is the body's primary "anti-inflammatory" circuit. By using biofeedback to increase HRV, patients can manually "down-regulate" the sympathetic nervous system, helping to re-plug the NMDAR.
- —Circadian Hygiene: Blocking blue light after sunset and ensuring early morning sunlight exposure helps to re-establish the melatonin/cortisol rhythm, providing the necessary hormonal environment for synaptic repair.
- —Cold Exposure: Brief, controlled exposure to cold (like a cold shower) can trigger a "hormetic" response, releasing endorphins and norepinephrine that help to "damp down" the central gain control.
##
Summary: Key Takeaways
The NMDA receptor is the fulcrum upon which the door of chronic pain swings. Understanding its biology is the difference between a life of managed misery and a path toward true recovery.
- —The "Wind-Up" is Structural: Chronic pain is not just a feeling; it is a physical rewiring of the nervous system driven by the removal of the NMDAR magnesium plug.
- —Magnesium is the Gatekeeper: Without sufficient magnesium, our nervous systems are "electrically naked" and prone to excitotoxicity and permanent sensitisation.
- —Opioids Can Be Counterproductive: In many cases of refractory pain, opioids act as "pro-NMDA" agents, worsening the underlying pathology through hyperalgesia.
- —The UK System is Lagging: Due to institutional inertia and the "Postcode Lottery," effective NMDA-targeted treatments like memantine and ketamine remain tragically under-utilised.
- —Recovery is Possible: Through a combination of specific NMDA antagonists, high-bioavailability magnesium, excitotoxin elimination, and circadian repair, the nervous system's gain control can be reset.
The frontier of pain management is no longer about "killing" the pain. It is about "re-plugging" the gate. For the millions of British citizens suffering in silence, the shift from opioid suppression to NMDA recalibration cannot come soon enough. We must demand a medical model that acknowledges the plastic, changeable nature of our biology—and provides the tools to change it for the better.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Clinical trials indicate that NMDA receptor antagonists can effectively reset pain sensitivity thresholds in patients suffering from complex regional pain syndrome.
Structural analysis shows that NMDA receptors contain specific binding pockets for allosteric inhibitors, offering a pathway for developing precise refractory pain treatments.
The research identifies that spinal NMDA receptor activation is essential for the long-term potentiation of pain signals in the dorsal horn.
The study demonstrates that memantine's uncompetitive antagonism of NMDA receptors specifically targets pathologically overactive channels in chronic pain states.
Evidence suggests that NMDA receptor antagonism facilitates rapid-acting analgesic effects by enhancing synaptogenesis in brain regions involved in pain processing.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "NMDA Receptor Antagonism: The Frontier of Refractory Pain Management"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper