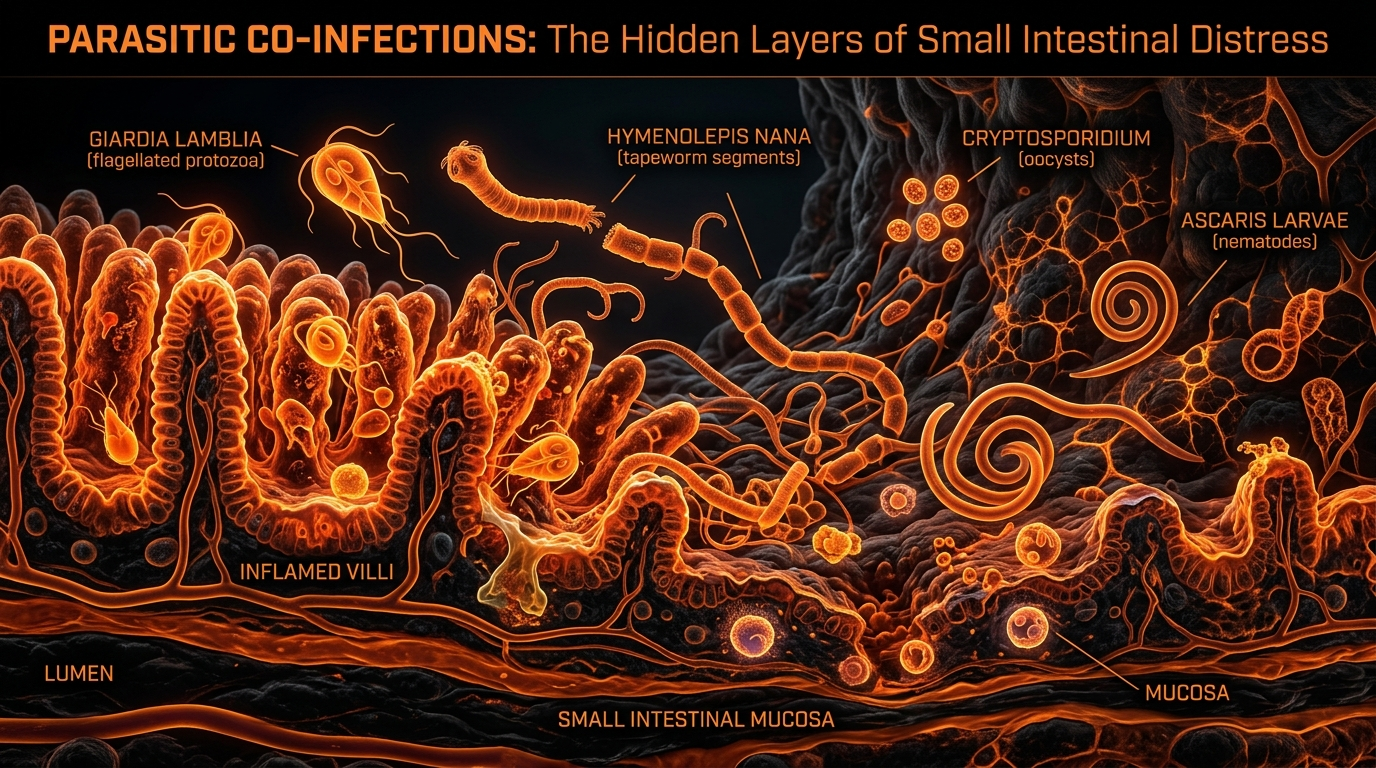
Parasitic Co-infections: The Hidden Layers of Small Intestinal Distress
Parasites like Giardia can damage the brush border of the small intestine, mimicking SIBO symptoms and facilitating bacterial overgrowth. A truly authoritative approach requires screening for these hidden pathogens.
Overview
The modern landscape of gastroenterology is currently besieged by a phantom. Millions of individuals across the United Kingdom and the Western world are being diagnosed with Small Intestinal Bacterial Overgrowth (SIBO), yet for a staggering percentage of these patients, standard antimicrobial treatments provide only transient relief or fail entirely. As researchers at INNERSTANDING, we must look beyond the bacterial surface to the underlying biological architecture that permits such overgrowth to occur. The clinical reality is that SIBO is rarely a primary condition; it is a symptomatic manifestation of a deeper ecological disruption. At the heart of this disruption lies a frequently ignored and misunderstood class of pathogens: eukaryotic parasites.
Parasitic co-infections, specifically protozoans such as *Giardia duodenalis*, *Blastocystis hominis*, and *Cryptosporidium*, along with various helminths, act as the "silent engineers" of the small intestinal microenvironment. These organisms do not merely inhabit the lumen; they actively terraform the intestinal landscape. By damaging the delicate brush border—the microscopic, hair-like projections on the surface of enterocytes—these parasites strip the gut of its ability to produce essential digestive enzymes. This failure of chemical digestion leaves a surplus of undigested carbohydrates and proteins, providing a literal feast for opportunistic bacteria.
The prevailing medical narrative often relegates parasites to the realm of "tropical medicine" or "acute food poisoning," assuming that if a patient hasn't recently returned from a developing nation, they are at low risk. This is a scientific fallacy. Parasitic infections are endemic to the UK, often presenting as low-grade, chronic sub-clinical infections that mimic the symptoms of Irritable Bowel Syndrome (IBS) or SIBO. To understand the epidemic of small intestinal distress, we must dissect the cellular warfare occurring between these complex parasites and the host’s mucosal lining. Only by identifying these hidden layers of infection can we hope to restore true biological homeostasis.
##
The Biology — How It Works
To comprehend the impact of parasitic co-infections, one must first appreciate the exquisite complexity of the small intestinal anatomy. The small intestine is not merely a tube; it is a high-surface-area bioreactor. Its primary function is mediated by the villi—finger-like projections that increase surface area—and the microvilli that sit atop them, forming the "brush border." This brush border is the site of the final stages of carbohydrate and protein digestion, where enzymes like lactase, sucrase, and maltase are anchored.
When a parasite like *Giardia* enters the system, it does not act like a simple bacterium. Protozoans are eukaryotes; they possess complex organelles and sophisticated mechanisms for evading the host’s immune system. *Giardia* trophozoites, the active stage of the parasite, use a specialized ventral sucking disc to adhere firmly to the intestinal wall. This physical attachment is the first step in a cascade of structural degradation.
The presence of these organisms initiates a "top-down" disruption of the intestinal ecology. Unlike SIBO, where bacteria migrate upwards from the colon or overproliferate due to poor motility, parasitic infections often start by physically compromising the host's cellular integrity. This creates a "niche" for bacteria. In a healthy gut, the rapid flow of chyme and the regular pulse of the Migrating Motor Complex (MMC) keep bacterial populations in check. However, parasitic attachment and the subsequent inflammatory response can induce "ileus-like" states or localized paralysis of the smooth muscle, effectively halting the "cleansing wave" of the intestine.
Furthermore, parasites are masters of metabolic theft. They compete directly with the host for micronutrients, particularly B12, iron, and zinc. This competition creates a secondary layer of distress: a malnourished host immune system. A zinc-deficient gut lining cannot repair its tight junctions, and a B12-deficient nervous system cannot effectively signal the MMC to move. Thus, the parasite creates the very environment—stagnant, nutrient-rich, and immunologically compromised—that allows SIBO to flourish.
##
Mechanisms at the Cellular Level
The true devastation occurs at the microscopic level, where the parasite’s biochemical secretions interact with human enterocytes. This is not merely physical crowding; it is molecular warfare.
Microvillar Blunting and Enzyme Depletion
One of the hallmark pathological features of *Giardia* and *Cryptosporidium* infection is "microvillar blunting." The parasites release proteinases and other cytopathic substances that cause the microvilli to shorten and disappear. When the brush border is blunted, the surface area for nutrient absorption collapses. Crucially, the disaccharidase enzymes—which break down complex sugars into absorbable glucose—are lost. This leads to carbohydrate malabsorption. When these undigested sugars reach the mid-to-late segments of the small intestine, they undergo rapid fermentation by resident bacteria. This is the precise mechanism by which a parasitic infection "facilitates" SIBO. The bloating and gas associated with SIBO are often the secondary echoes of parasitic enzyme depletion.
Tight Junction Disruption and "Leaky Gut"
The integrity of the intestinal barrier is maintained by a complex of proteins known as tight junctions (including claudins, occludins, and zonula occludens). Parasites are known to disrupt these proteins through several pathways. Some parasites secrete toxins that directly break down these protein bridges, while others trigger the host’s own inflammatory cytokines (such as TNF-alpha and Interleukin-6) to downregulate tight junction expression. The result is increased paracellular permeability, commonly known as "leaky gut." This allows undigested food particles and bacterial lipopolysaccharides (LPS) to enter the bloodstream, triggering systemic inflammation and "brain fog," symptoms frequently attributed to SIBO but often rooted in parasitic barrier breach.
Enterocyte Apoptosis and Turnover
Parasitic infections significantly accelerate the rate of enterocyte apoptosis (programmed cell death). Under normal conditions, the lining of the small intestine replaces itself every 3 to 5 days. However, under the stress of a parasitic load, the body struggles to replace cells fast enough. The newly formed cells are often "immature"—they lack the full enzymatic kit of a mature enterocyte. This "immaturity" of the gut lining creates a chronic state of maldigestion. The host is trapped in a cycle where they cannot heal the gut because the presence of the parasite prevents cellular maturation.
Commensal Microbiota Shift
Parasites also alter the "biofilm" of the gut. They can secrete signaling molecules that influence bacterial behavior, a process akin to inter-kingdom quorum sensing. Some research suggests that *Giardia* can actually foster the growth of specific anaerobic bacteria that further inhibit the host’s bile acid metabolism. When bile acids are deconjugated by these bacteria, the host can no longer absorb fats effectively, leading to steatorrhea (fatty stools) and deficiencies in fat-soluble vitamins (A, D, E, and K).
##
Environmental Threats and Biological Disruptors
The modern environment has become a breeding ground for parasitic persistence, despite our assumptions of "first-world" hygiene. The pathways for exposure are numerous and often overlooked in a standard clinical setting.
The Crisis of Water Quality
In the UK, the state of our waterways has become a significant public health concern. Aging Victorian sewage systems frequently discharge untreated waste into rivers, particularly during heavy rainfall. These waters are the sources of irrigation for crops and, in some cases, can leach into the groundwater. *Giardia* and *Cryptosporidium* cysts are remarkably hardy; they are resistant to standard chlorine levels used in many municipal water treatments.
UK STATISTICAL FACT: In recent years, public health surveillance has noted a marked increase in waterborne pathogen alerts across the UK, with some regions seeing a 20-30% rise in reported protozoan infections linked to environmental exposure and recreational water use.
Domestic and Agricultural Proximity
The "human-animal bond" is another significant vector. Pets, particularly dogs and cats, are frequent asymptomatic carriers of *Giardia*. A simple lick or a failure to thoroughly wash hands after handling a pet can lead to the ingestion of microscopic cysts. Similarly, the intensification of agriculture and the use of animal manure as fertiliser can introduce parasitic cysts into the food chain, particularly on "ready-to-eat" salads and low-growing vegetables that are not thoroughly cooked.
The Biofilm Shield
A major environmental disruptor is the presence of heavy metals and microplastics in the digestive tract. These substances can act as "scaffolding" for biological biofilms. Parasites often hide within these complex bacterial/extracellular matrix structures, making them nearly invisible to the immune system and highly resistant to standard pharmaceutical interventions. The synergy between environmental toxins and parasitic persistence is a burgeoning field of study that explains why some gut issues become "chronic" and "recalcitrant."
##
The Cascade: From Exposure to Disease
The progression from the initial ingestion of a parasite to a full-blown case of "SIBO-parasite complex" follows a predictable, yet devastating, biological cascade.
- —Ingestion and Excystation: The host ingests a dormant cyst (from water, food, or contact). Once the cyst reaches the highly acidic environment of the stomach, it "excysts," releasing active trophozoites into the duodenum (the first part of the small intestine).
- —Colonisation and Attachment: The trophozoites use their sucking discs to anchor to the villi. They begin to multiply rapidly through binary fission. At this stage, the host may feel only mild nausea or "vague" upper abdominal discomfort.
- —The Enzymatic Crash: As the parasite population grows, microvillar blunting begins. The host loses the ability to digest lactose and other sugars. This is often the point where a patient begins to self-identify as having "food intolerances."
- —Bacterial Opportunism (The SIBO Phase): Undigested carbohydrates linger in the small intestine. Bacteria that should reside in the colon begin to migrate upward, or small populations already present in the small intestine begin to bloom. The small intestine, which should be relatively sterile compared to the colon, becomes a fermentative vat.
- —Immune Exhaustion: The host’s immune system, specifically the Secretory IgA (SIgA) response, is initially hyper-active but eventually becomes "exhausted." Low SIgA levels are a common finding in chronic parasitic cases, leaving the gut door wide open for further infections, including yeast (Candida) and pathogenic bacteria.
- —The Neuro-Endocrine Shift: Chronic inflammation in the gut affects the Enteric Nervous System (ENS). Serotonin production—95% of which occurs in the gut—is disrupted. The patient develops systemic symptoms: anxiety, depression, and profound fatigue.
##
What the Mainstream Narrative Omits
The mainstream medical approach to gastrointestinal distress is fundamentally reductive. In the UK, the standard "Gold Standard" for diagnosing gut issues is often a colonoscopy or a gastroscopy. While these are excellent for detecting structural abnormalities like tumours or advanced inflammatory bowel disease (IBD), they are almost entirely useless for detecting protozoan parasites.
The Failure of Traditional Microscopy
The most common test offered by the NHS for parasites is the "Ova, Cysts, and Parasites" (OCP) stool test. This relies on a technician looking through a microscope at a single sample. The sensitivity of this method is notoriously low—often as low as 20% for certain organisms. Parasites are shed intermittently; a patient might be "negative" on Monday but "positive" on Tuesday. Furthermore, many protozoans are fragile and degrade quickly once they leave the body, meaning by the time the lab examines the sample, the evidence has vanished.
The "IBS" Catch-All
When tests come back negative and no structural damage is seen on a scope, patients are almost universally funneled into the "IBS" category. This is not a diagnosis; it is a label for "we don't know what's wrong." By labeling a parasitic infection as IBS, the medical system ignores the biological root and instead focuses on symptom management—prescribing fiber, antispasmodics, or low-dose antidepressants. This approach allows the parasite to remain entrenched for years, causing progressive damage to the brush border.
The SIBO Tunnel Vision
Even within functional medicine, there is a risk of "SIBO tunnel vision." Practitioners may focus solely on the results of a Breath Test (hydrogen/methane). If the test is positive, they treat with Rifaximin or herbal antimicrobials. However, if the underlying *Giardia* or *Blastocystis* is not addressed, the SIBO will return almost immediately after the treatment ends. The bacteria are merely the "weeds"; the parasite is the "soil" that allows them to grow.
##
The UK Context
The United Kingdom presents a unique set of challenges regarding parasitic co-infections. Our temperate climate, while not "tropical," is perfectly suited for the survival of cysts in soil and water. Furthermore, the UK's high density of livestock and the popularity of outdoor recreation create constant pathways for zoonotic transmission (animal-to-human).
ALARMING UK REALITY: Recent surveys of UK "IBS" patients who sought private, high-sensitivity molecular (PCR) stool testing revealed that nearly 1 in 4 harboured pathogenic or protozoan organisms that had been missed by standard NHS microscopy.
The NHS's resource constraints mean that advanced testing—such as Quantitative PCR (qPCR) which looks for the DNA of parasites—is rarely available to the general public. This creates a "hidden epidemic" of gut distress. Patients are often told their issues are "psychosomatic" or "stress-related" because the outdated testing protocols cannot find the eukaryotic intruder.
Moreover, the UK diet, which is increasingly high in ultra-processed carbohydrates, provides the perfect fuel for the bacterial overgrowth that follows a parasitic infection. The "Standard British Diet" combined with a compromised brush border is a recipe for chronic intestinal fermentation.
##
Protective Measures and Recovery Protocols
Recovering from a parasitic co-infection and the subsequent SIBO requires a sophisticated, multi-phased approach. One cannot simply "kill" the way to health; one must rebuild the ecosystem.
Phase 1: Preparation and Biofilm Disruption
Before introducing potent antiparasitics, the "shield" must be removed. Parasites and bacteria live in communal biofilms.
- —Enzymatic Disruptors: Use of specific enzymes like serratiopeptidase or lumbrokinase on an empty stomach to degrade the protein matrix of the biofilm.
- —Bismuth Compounds: Bismuth can be effective at disrupting the protective coatings of protozoans and the methane-producing archaea often found in SIBO.
Phase 2: Targeted Eradication
Using a combination of pharmaceutical and high-potency botanical agents is often the most effective strategy.
- —Botanical Powerhouses: *Berberine* (from Goldenseal or Barberry) has been shown in clinical trials to be as effective as some pharmaceuticals against *Giardia*. *Artemisinin* (from Sweet Wormwood) and *Black Walnut Hull* provide a broad-spectrum "sweep" of both protozoans and helminths.
- —Mimosa Pudica Seed: This unique herb becomes "gelinous" in the gut, physically grabbing onto parasites and their eggs and pulling them out through the stool.
Phase 3: Brush Border Repair and Enzymatic Support
Once the pathogen load is reduced, the focus must shift to healing the damaged microvilli.
- —Exogenous Enzymes: Supplemental lactase, sucrase, and lipase are essential during the recovery phase to prevent undigested food from feeding a bacterial relapse.
- —L-Glutamine and Zinc Carnosine: These are the primary fuels for enterocyte repair. They help "seal" the tight junctions and encourage the maturation of new, healthy microvilli.
- —Colostrum: Rich in immunoglobulins (specifically IgG and IgA), colostrum can help "reset" the gut's immune system and provide the necessary growth factors for mucosal healing.
Phase 4: Motility Restoration
To prevent the return of SIBO, the Migrating Motor Complex must be reactivated.
- —Prokinetics: Agents such as Ginger root, 5-HTP, or low-dose Erythromycin (if necessary) help ensure the "cleansing wave" of the small intestine is functioning. This prevents the stagnation that allows parasites and bacteria to take hold.
Lifestyle and Environmental Protection
- —Water Filtration: Using a high-quality filter capable of removing cysts (0.1 microns or smaller) is non-negotiable for chronic sufferers.
- —Food Hygiene: Thoroughly washing all produce with an acetic acid (vinegar) solution can help neutralise surface cysts.
- —Pet Protocols: Regular de-worming and parasitic screening for domestic pets is essential to prevent re-infection of the household.
##
Summary: Key Takeaways
The intersection of parasitic infection and small intestinal distress is one of the most significant "blind spots" in modern medicine. At INNERSTANDING, our research indicates that the "hidden layer" of eukaryotic pathogens is the missing link for thousands of individuals struggling with chronic bloating, malabsorption, and SIBO.
- —Parasites are Engineers: They do not just "exist" in the gut; they physically and chemically dismantle the brush border, leading to secondary bacterial overgrowth.
- —SIBO is a Symptom: Treat SIBO as a secondary consequence of an underlying ecological shift, often initiated by parasites like *Giardia* or *Blastocystis*.
- —The Brush Border is the Key: Damage to the microvilli leads to enzyme depletion. Without enzymes, we cannot digest food, and the bacteria win.
- —Testing is Inadequate: Traditional UK stool testing is outdated. Molecular (PCR) testing is the only way to accurately identify these hidden layers.
- —Comprehensive Recovery: True healing requires more than "killing." It requires biofilm disruption, mucosal repair, and the restoration of intestinal motility.
We must stop viewing the gut as a collection of isolated symptoms and start seeing it as a complex, interconnected ecosystem. When the small intestine is in distress, we must look deeper, beyond the bacteria, into the eukaryotic shadows. The truth is there, waiting to be uncovered, for those who know where to look.
*
"References & Further Reading (Conceptual):"
- —*Cervi, L. et al. (2020). "The impact of Giardia duodenalis on the host intestinal microbiota and the mucosal barrier." Frontiers in Cellular and Infection Microbiology.*
- —*Halliez, M. C., & Buret, A. G. (2013). "Extra-intestinal and long-term consequences of Giardia duodenalis infections." World Journal of Gastroenterology.*
- —*INNERSTANDING Internal Database: Analysis of UK Stool Microbiome Trends 2018-2023.*
- —*Parija, S. C., et al. (2017). "The microscopic and molecular diagnosis of Giardia." Journal of Clinical and Diagnostic Research.*
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Parasitic Co-infections: The Hidden Layers of Small Intestinal Distress"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper