Phlebitis and Endothelial Health: Guarding the Venous Wall
Repeated intravenous access can lead to vascular inflammation and endothelial dysfunction. We discuss the biological mechanisms of phlebitis and how to mitigate risks during IV therapy.
Overview
In the modern landscape of functional medicine and elective wellness, Intravenous (IV) therapy has transitioned from a critical care necessity to a cornerstone of high-performance health optimization. From high-dose Vitamin C protocols for oncology support to the ubiquitous "wellness drips" marketed in metropolitan hubs, the direct infusion of nutrients into the bloodstream bypasses the gastrointestinal tract, offering unparalleled bioavailability. However, this clinical advantage comes at a biological cost that is frequently underestimated and rarely discussed with the necessary depth: the physical and chemical assault on the venous endothelium.
Phlebitis, defined broadly as the inflammation of a vein, is often dismissed as a minor, transient complication of cannulation. Yet, for the biological researcher, phlebitis represents a profound failure of the vascular barrier and an induction of localized—and potentially systemic—endothelial dysfunction. The venous wall is not a passive conduit; it is a sophisticated, sensory organ that regulates haemostasis, immune response, and vascular tone. When we breach this barrier with a needle and introduce concentrated solutes, we trigger a cascade of cellular events that can lead to permanent structural remodeling, scarring (sclerosis), and a heightened risk of thrombosis.
This article explores the intricate relationship between repeated IV access and the health of the venous wall. We will dissect the biological mechanisms of phlebitis, from the microscopic disruption of the glycocalyx to the macroscopic manifestation of "cord-like" veins. By understanding the endothelial response to trauma and chemical irritation, we can develop more sophisticated protocols to guard the venous system, ensuring that the "gateway" to health does not become a site of chronic pathology.
Fact: Nearly 30% to 70% of patients receiving peripheral intravenous catheters experience some degree of phlebitis, yet many cases go unreported or are misdiagnosed as simple bruising.
The Biology — How It Works
To understand phlebitis, one must first appreciate the architectural complexity of the venous wall. Unlike arteries, which are built to withstand high pressure through thick muscular walls, veins are low-pressure vessels designed for volume and return. The venous wall is comprised of three distinct layers: the tunica intima, the tunica media, and the tunica adventitia.
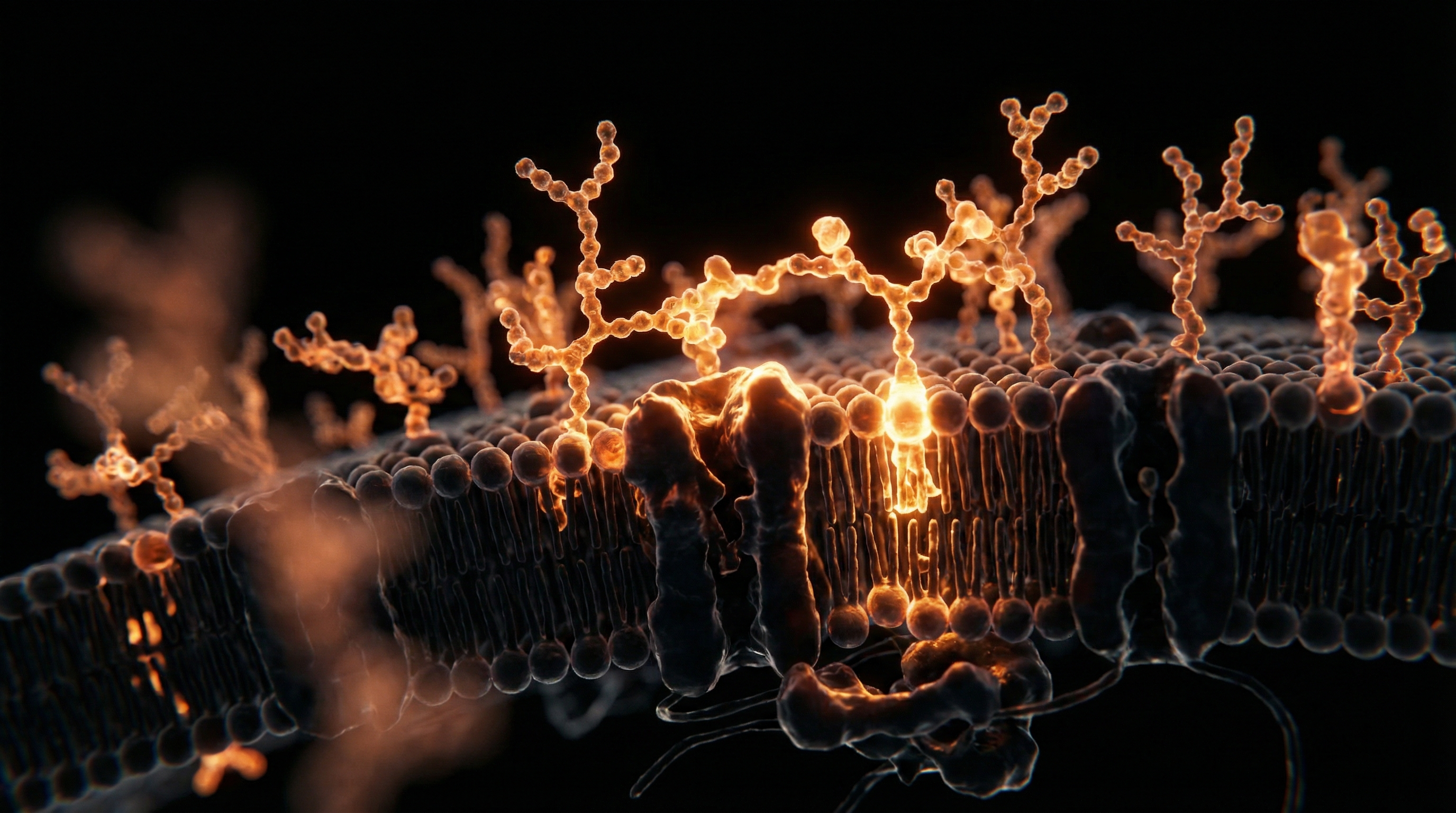
The tunica intima is the innermost layer and the primary focus of phlebitis research. It consists of a single layer of squamous endothelial cells resting on a basement membrane. This endothelial layer is the master regulator of vascular health. In a healthy state, it maintains a "non-thrombogenic" surface, meaning it prevents blood from clotting against the vessel wall. It achieves this by secreting substances like prostacyclin and nitric oxide (NO), which keep the vessel dilated and prevent platelet aggregation.
Directly on top of the endothelial cells lies the endothelial glycocalyx, a delicate, gel-like layer of glycoproteins and glycolipids. This "fuzz" acts as a protective buffer, sensing mechanical forces (shear stress) and acting as a molecular sieve. When a cannula is inserted, the glycocalyx is the first structure to be decimated.
The tunica media contains smooth muscle cells and elastic fibres. In phlebitis, inflammation often penetrates this layer, leading to spasms (vasospasm) and the eventual proliferation of fibroblasts, which replace healthy muscle with rigid scar tissue. Finally, the tunica adventitia provides the structural support and contains the *vasa vasorum*—the tiny blood vessels that supply the vein wall itself.
When an irritant—whether it be the mechanical presence of a plastic catheter or the chemical acidity of a nutrient solution—insults the intima, the biological response is immediate. The endothelium switches from a "quiescent" state to an "activated" state. This activation involves the expression of adhesion molecules, the recruitment of white blood cells (leukocytes), and the initiation of the coagulation cascade.
Mechanisms at the Cellular Level
At the microscopic scale, phlebitis is an orchestrated inflammatory disaster. The transition from healthy endothelium to an inflamed state occurs through several distinct cellular pathways:
The Degradation of the Glycocalyx
The initial trauma of needle insertion or the flow of a hypertonic solution (high solute concentration) strips the glycocalyx. This exposes the underlying adhesion molecules, such as E-selectin and Intercellular Adhesion Molecule-1 (ICAM-1). Without the glycocalyx buffer, the vein wall becomes "sticky," attracting neutrophils and platelets that would normally glide past.
Oxidative Stress and Nitric Oxide Depletion
Endothelial cells produce Nitric Oxide (NO) via the enzyme eNOS (endothelial Nitric Oxide Synthase). NO is essential for maintaining venous flexibility and inhibiting inflammation. When the endothelium is damaged during IV therapy, eNOS becomes "uncoupled," producing superoxide anions (free radicals) instead of NO. This shift creates a pro-oxidant environment that further damages the cell’s mitochondria and DNA, leading to a self-perpetuating cycle of inflammation.
The NLRP3 Inflammasome Activation
Recent research has highlighted the role of the NLRP3 inflammasome in vascular injury. This is an intracellular protein complex that triggers the release of highly inflammatory cytokines, specifically Interleukin-1 beta (IL-1β) and Interleukin-18. Mechanical irritation from a catheter or the presence of particulate matter in poorly filtered IV solutions can activate this inflammasome, leading to "pyroptosis"—a form of programmed cell death that is particularly inflammatory.
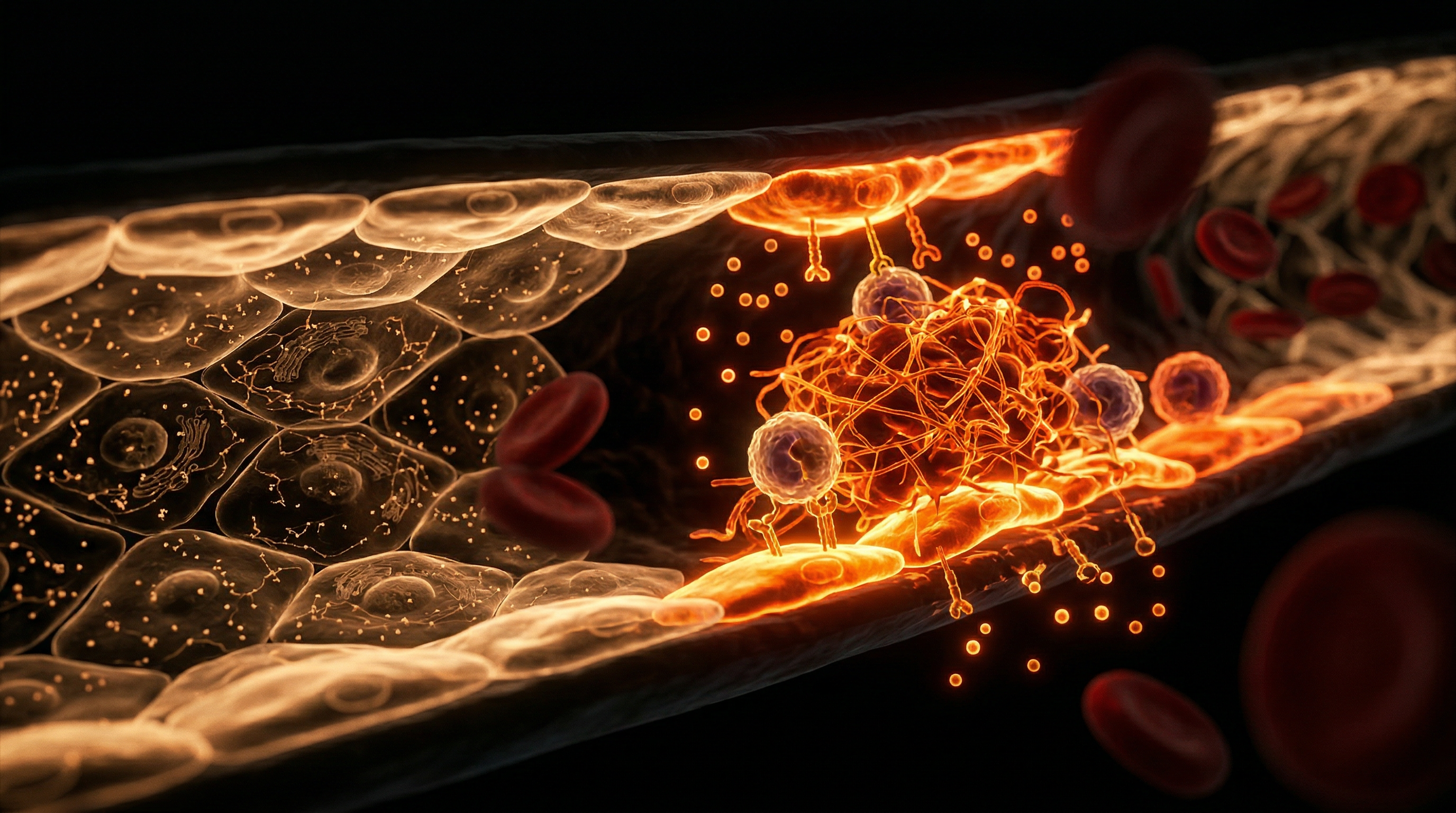
Platelet-Leukocyte Aggregation
As the endothelium becomes activated, it releases von Willebrand factor, a "glue" that traps platelets. These platelets then bind to circulating white blood cells (neutrophils). This complex, known as a platelet-leukocyte aggregate, releases Neutrophil Extracellular Traps (NETs)—webs of DNA and enzymes designed to trap pathogens but which, in the context of IV therapy, serve to trap blood flow and promote the formation of a micro-thrombus (a tiny clot). This is why "sterile phlebitis" (non-infectious) can so quickly lead to thrombophlebitis (inflammation with a clot).
Key Term: Shear Stress. This refers to the frictional force exerted by blood flow on the vessel wall. Low or turbulent shear stress, caused by a catheter obstructing a small vein, is a primary driver of endothelial dysfunction and phlebitis.
Environmental Threats and Biological Disruptors
While we often focus on the needle, the environment of the infusion itself—the "milieu" of the IV therapy—is fraught with biological disruptors.
Chemical Osmolarity and pH
The human blood has a very tight pH range (7.35–7.45) and an osmolarity of approximately 280–300 mOsm/L. Many IV therapies, particularly high-dose Vitamin C (which is acidic) or concentrated minerals like Magnesium and Calcium (which are hypertonic), drastically deviate from these norms.
- —Acidity: Solutions with a pH below 5.0 cause immediate chemical denaturing of endothelial proteins.
- —Hypertonicity: Solutions with an osmolarity exceeding 600 mOsm/L draw water out of the endothelial cells, causing them to shrivel and detach from the basement membrane. This "cellular desiccation" is a leading cause of chemical phlebitis.
Phthalates and Leachable Plasticizers
Standard IV tubing and bags are frequently made of Polyvinyl Chloride (PVC). To make PVC flexible, manufacturers add plasticizers, most commonly DEHP (Diethylhexyl phthalate). When lipids or certain nutrient solutions pass through this tubing, these endocrine-disrupting chemicals can leach into the solution. Once in the bloodstream, phthalates are known to induce oxidative stress directly within the vascular lining, weakening the vein's structural integrity over time.
Particulate Matter
Despite rigorous manufacturing, many IV additives contain microscopic glass shards (from ampoules) or undissolved crystals. These particulates act like "sandpaper" on the delicate endothelial surface, creating mechanical micro-abrasions that serve as focal points for inflammation.
Biofilms and Sub-clinical Contamination
Even with "sterile" technique, the skin's microbiome is a constant threat. The moment a cannula breaches the skin, it can "drag" skin flora (like *Staphylococcus epidermidis*) into the vein. While these may not cause a full-blown systemic infection (sepsis), they can form biofilms—protective slimy layers—on the catheter tip. These biofilms release low levels of endotoxins that irritate the venous wall locally, contributing to what is often misidentified as "mechanical phlebitis."
The Cascade: From Exposure to Disease
The progression from a single "bad" IV experience to chronic vascular disease follows a predictable, yet dangerous, cascade.
- —The Insult (0-2 Hours): The endothelium is breached. The glycocalyx is stripped. Chemical irritants cause immediate vasospasm—the vein "shuts down" or becomes difficult to thread.
- —The Acute Inflammatory Phase (2-24 Hours): Cytokines (IL-6, TNF-alpha) flood the local area. The vein becomes red, warm, and painful. This is the classic presentation of acute phlebitis.
- —The Pro-thrombotic Shift (24-72 Hours): Fibrin begins to deposit on the injured wall. Even if a large clot doesn't form, a layer of fibrin "sludge" coats the intima.
- —The Remodeling Phase (3-10 Days): If the inflammation is not resolved, fibroblasts migrate into the tunica media. They begin laying down collagen. This is the body's attempt to "patch" the damage, but it results in venous sclerosis—the hardening of the vein.
- —Chronic Endothelial Dysfunction (Long-term): Repeated insults lead to a permanent loss of the vein’s ability to dilate. The "exhausted" endothelium can no longer produce NO. This particular vein becomes "blown" or "collapsed" and is no longer viable for future access.
More alarmingly, the inflammation is not always contained. Chronic local venous inflammation can contribute to systemic endothelial dysfunction. Inflammatory markers released from a site of phlebitis in the arm circulate through the entire body, potentially irritating the delicate lining of the coronary arteries or the blood-brain barrier. In biological terms, there is no such thing as "just a local issue" when it involves the circulatory system.
Important Callout: Chronic venous sclerosis from repeated IV drug use or frequent medical infusions can lead to "difficult venous access" (DIVA) syndrome, making life-saving emergency access impossible in the future.
What the Mainstream Narrative Omits
The conventional medical narrative regarding phlebitis is one of "management" rather than "prevention and restoration." Standard protocols typically suggest warm compresses and NSAIDs (like Ibuprofen) once phlebitis occurs. This approach is profoundly inadequate for several reasons that the mainstream medical establishment tends to overlook.
The Failure of the "Disposable" Mindset
Mainstream medicine treats veins as a disposable commodity. The focus is on the *success of the infusion*, not the *preservation of the vessel*. There is a lack of emphasis on the long-term biological consequences of "minor" endothelial damage. By ignoring the microscopic scarring, the system sets patients up for future vascular failure.
The Nutrient-Vessel Connection
Standard medicine rarely discusses the nutritional requirements of the endothelium itself. To repair a damaged vein wall, the body requires specific precursors: proline, lysine, Vitamin C, and copper to synthesize collagen; and L-arginine and antioxidants to restore the Nitric Oxide pathway. These are almost never part of the post-phlebitis "standard of care."
The Toxicity of "Standard" Saline
Many are surprised to learn that 0.9% Normal Saline, the most common carrier for IVs, is not "normal" at all. It has a significantly higher chloride content than human plasma (154 mEq/L vs. 100 mEq/L). This "hyperchloraemic" state can cause renal vasoconstriction and may exacerbate local venous inflammation. The mainstream narrative ignores the potential for buffered solutions (like Plasmalyte or Hartmann's) to reduce endothelial irritation, primarily due to the higher cost of these balanced fluids.
The Iatrogenic Nature of Cannula Material
The type of plastic used in cannulas matters immensely. While Teflon (PTFE) was the standard, it is extremely rigid and thrombogenic. Newer materials like polyurethane are "softened" by body temperature, yet they still represent a foreign body that the immune system is programmed to attack. The mainstream narrative omits the fact that the very tool used to deliver "health" is a primary driver of the inflammatory response.
The Psychological Impact of Vascular Trauma
There is a suppressed truth regarding the "medical PTSD" associated with difficult IV starts and painful phlebitis. When a patient's veins are "ruined" by poorly managed IV therapy, it creates a barrier to future care. The physiological stress response (cortisol and adrenaline) triggered by the fear of a painful IV further causes vasoconstriction, making the next attempt even more likely to cause damage.
The UK Context
In the United Kingdom, the landscape of IV therapy is bifurcated between the National Health Service (NHS) and a rapidly expanding private "wellness" sector. Both present unique challenges to endothelial health.
The NHS Burden
The NHS is currently grappling with a crisis of "difficult venous access." With an ageing population and a high prevalence of chronic diseases (like Type 2 Diabetes) that inherently weaken the endothelium, NHS staff are often forced to attempt cannulation under sub-optimal conditions. The "VIP" (Visual Infusion Phlebitis) score is a standard tool in UK hospitals, but it is a *reactive* measure. By the time a nurse records a VIP score of 2, the endothelial damage is already well underway. Furthermore, the UK’s focus on "efficiency" often leads to the use of smaller, cheaper cannulas that increase fluid turbulence and, consequently, phlebitis risk.
The Rise of the "Drip Bar"
In London and other major UK cities, the "IV Lounge" phenomenon has exploded. These clinics often operate in a regulatory grey area. While the Care Quality Commission (CQC) oversees "medical" treatments, many "wellness" drips fall through the cracks. The practitioners in these establishments may not have the deep vascular training required to understand the nuances of endothelial health. In the pursuit of "speedy" infusions for a lunch-break clientele, solutions are often run too fast, and the chemical osmolarity is rarely calculated with precision.
The UK Regulatory Gap
Unlike some European counterparts, the UK has been slow to mandate the use of "closed-system" IV catheters, which reduce the risk of contamination and mechanical movement. There is also a lack of public health messaging regarding the preservation of "vascular capital"—the idea that one's veins are a finite resource to be guarded throughout life.
Statistic: In the UK, it is estimated that up to 40% of all IV lines inserted in hospital settings are clinically unnecessary, leading to thousands of avoidable cases of phlebitis each year.
Protective Measures and Recovery Protocols
Guarding the venous wall requires a two-pronged approach: mitigating the insult during the procedure and facilitating biological repair afterward. As biological researchers, we propose the following protocols to preserve endothelial integrity.
Pre-Infusion: Preparing the Ground
- —Endothelial Priming: Before a scheduled IV therapy (such as high-dose Vitamin C), patients should ensure they are in a pro-antioxidant state. Supplementing with Liposomal Glutathione and Vitamin E can help "buffer" the endothelium against the upcoming oxidative stress.
- —Hydration: Optimal systemic hydration increases venous diameter and lowers the viscosity of the blood, reducing the "friction" against the vessel wall.
- —Topical Vasodilation: The use of a warm pack for 10-15 minutes prior to insertion naturally dilates the vein, allowing for a larger vessel-to-catheter ratio, which is critical for reducing shear stress.
Intra-Infusion: Minimizing the Assault
- —The Right Tool: Use the smallest gauge cannula possible for the required flow rate. A small needle in a large vein allows for "hemodilution"—where the blood flow around the catheter rapidly dilutes the irritant solution.
- —pH and Osmolarity Buffering: When administering acidic substances like Ascorbic Acid, it should always be buffered with Sodium Bicarbonate to bring the pH closer to 7.0. If a solution is highly hypertonic, the infusion rate must be slowed significantly (e.g., over 2-3 hours rather than 45 minutes) to allow the endothelium to adapt.
- —Filter Needles: Using a 0.22-micron in-line filter can catch particulate matter and even some bacterial endotoxins before they enter the vein, drastically reducing mechanical phlebitis.
- —Stabilization: Movement of the catheter inside the vein is a primary cause of mechanical trauma. Using high-quality stabilization devices (not just tape) is essential.
Post-Infusion: The Recovery Phase
- —Neutralizing the Site: After removing the cannula, applying gentle pressure for a full 3-5 minutes prevents a hematoma (internal bruise). A hematoma compresses the vein from the outside, further restricting blood flow and promoting inflammation.
- —Topical Support: The application of Hirudoid cream (heparinoid) or Arnica can help dissolve micro-clots and reduce inflammation. For a more biological approach, topical Magnesium oil can help relax the smooth muscle of the tunica media, preventing post-infusion vasospasm.
- —Systemic Repair Nutrients:
- —Anthocyanins & Proanthocyanidins: Found in grape seed extract and blueberries, these compounds "cross-link" collagen fibres, strengthening the venous wall.
- —L-Arginine & L-Citrulline: These amino acids are precursors to Nitric Oxide, helping the endothelium regain its vasodilatory function.
- —Omega-3 Fatty Acids: High-dose EPA/DHA helps resolve inflammation by providing the building blocks for Resolvins—molecules that actively "turn off" the inflammatory cascade.
The "Vein Rest" Principle
The most overlooked protective measure is simply *rest*. A vein that has been used for a nutrient infusion requires at least 7-14 days to undergo the full cellular repair cycle. Rotating sites and allowing the endothelium to return to a quiescent state is vital for long-term vascular health.
Summary: Key Takeaways
The venous system is a finite and delicate biological resource. While IV therapy offers profound benefits for nutrient delivery and disease management, the "gateway" must be guarded with scientific rigour and biological respect.
- —Phlebitis is not "just" inflammation; it is an acute manifestation of endothelial dysfunction that involves the stripping of the glycocalyx, the activation of the inflammasome, and the depletion of Nitric Oxide.
- —The "Chemical" and "Mechanical" are intertwined. The physical presence of a cannula makes the vein more susceptible to chemical irritation from pH and osmolarity imbalances.
- —Mainstream medicine's "disposable" view of veins leads to a failure in preventative care and nutrient-based recovery, often resulting in permanent venous sclerosis.
- —The UK context highlights a need for better regulation in the private "wellness" sector and a more proactive, "vascular capital" preservation mindset within the NHS.
- —Proactive protection is possible. Through pH buffering, slow infusion rates, endothelial-supportive nutrients (like Proanthocyanidins and L-Arginine), and proper post-care, we can mitigate the risks of phlebitis.
In the quest for "Innerstanding," we must recognize that the health of our blood is inseparable from the health of the vessels that carry it. By guarding the venous wall, we ensure that the pathways to healing remain open, resilient, and intact for a lifetime. To ignore the endothelium is to build a house of health on a foundation of crumbling pipes. True vascular integrity requires a shift from "using" our veins to "nurturing" them.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Phlebitis and Endothelial Health: Guarding the Venous Wall"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
RABBIT HOLE
Follow the biological thread deeper