Restless Leg Syndrome: Investigating the Iron-SIBO Connection
Small intestinal bacteria can sequestrate dietary iron, leading to local deficiencies that trigger neurological symptoms like Restless Leg Syndrome. This connection highlights the systemic impact of localized intestinal overgrowth.
Overview
Restless Leg Syndrome (RLS), historically termed Willis-Ekbom Disease, has long been relegated to the peripheries of idiopathic neurological disorders—a condition defined by its symptoms rather than its etiology. For the millions of sufferers globally, and the significant percentage of the British population grappling with its nocturnal disturbances, RLS is characterised by an irresistible urge to move the limbs, typically accompanied by uncomfortable "creeping," "crawling," or "tugging" sensations. While the mainstream medical consensus has traditionally pointed toward dopaminergic dysfunction and systemic iron deficiency, a more profound and unsettling biological truth is emerging from the nexus of gastroenterology and neurology.
At INNERSTANDING, we recognise that the human body does not function in isolation; it is a symphonic interplay of systemic feedback loops. The emerging research into the Iron-SIBO Connection suggests that RLS is not merely a "brain problem" or a simple "nutrient deficiency." Instead, it is often a secondary manifestation of a primary ecological collapse within the small intestine. Small Intestinal Bacterial Overgrowth (SIBO)—the proliferation of colonic bacteria in the upper digestive tract—serves as a biological "thief," sequestering dietary iron before it can reach the systemic circulation or the blood-brain barrier.
This article serves as a comprehensive investigation into the mechanisms by which microscopic invaders in the gut can hijack the host’s mineral stores, leading to a state of cerebral iron deficiency despite seemingly "normal" peripheral blood markers. We will deconstruct the molecular theft of iron by bacterial siderophores, the inflammatory cascades that lock iron away in storage, and the environmental factors that have turned the modern gut into a breeding ground for this neurological disruption. To understand RLS, one must look past the twitching limb and into the microscopic battleground of the duodenum and jejunum.
In the United Kingdom, it is estimated that nearly 10% of the population suffers from some form of Restless Leg Syndrome, yet only a fraction receive a diagnosis that investigates the underlying gastrointestinal pathology.
---
##
The Biology — How It Works
To comprehend the link between the gut and the restless limb, one must first understand the unique biological imperatives of both the human host and the microbial overgrowth. Iron is the most precious commodity in the biological world; it is the fundamental catalyst for DNA synthesis, cellular respiration, and the production of neurotransmitters. However, humans have no active mechanism for excreting excess iron, and similarly, we have evolved a highly complex, "tight-fisted" system for its absorption.
The Duodenal Gateway
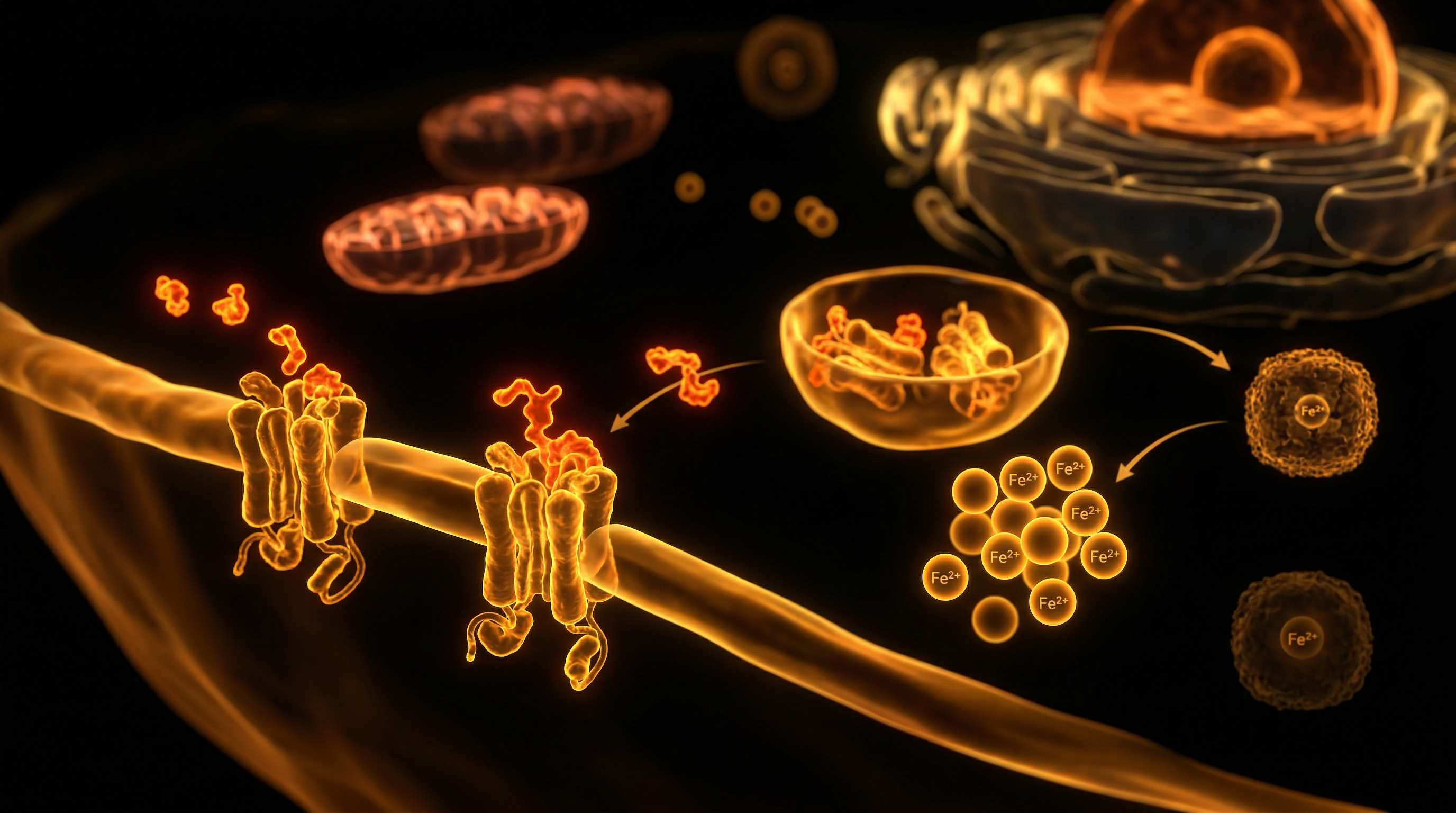
The majority of iron absorption occurs in the duodenum and the proximal jejunum. Under normal physiological conditions, dietary iron (in ferric or ferrous forms) is processed by gastric acid and then transported across the apical membrane of the enterocyte via the Divalent Metal Transporter 1 (DMT1). From here, it is either stored as ferritin within the cell or exported into the bloodstream via ferroportin, the only known cellular iron exporter.
The tragedy of SIBO is that it occurs precisely at this primary site of absorption. When the small intestine is colonised by excessive levels of *Escherichia coli*, *Klebsiella*, or *Enterococcus*, the ecological balance is shattered. These bacteria are not passive residents; they are aggressive competitors for nutrients.
The Molecular Theft: Siderophores
Microorganisms require iron for their own metabolic processes and biofilm formation. To acquire it in the competitive environment of the gut, they secrete siderophores—low-molecular-weight, high-affinity iron-chelating compounds. These bacterial molecules have an affinity for iron that is significantly higher than that of the human transport proteins like transferrin.
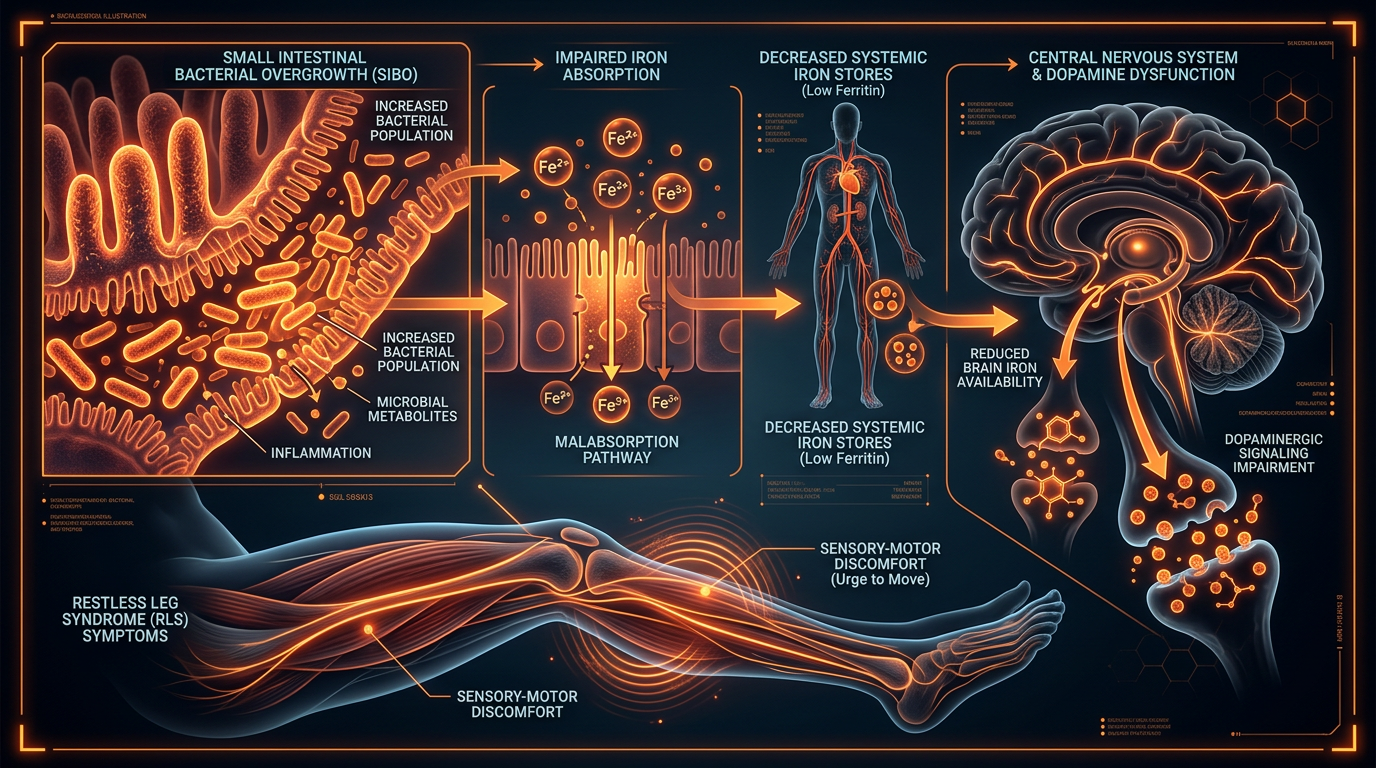
In a patient with SIBO, the small intestine becomes a "sink" for dietary iron. Before the human enterocytes can engage the DMT1 transporters, bacterial siderophores have already bound the available iron, sequestering it for microbial use. This leads to a state of localised iron depletion in the gut lining, which eventually translates to systemic and, crucially, neurological shortages.
The Barrier Dysfunction
Furthermore, the presence of SIBO induces a state of chronic, low-grade mucosal inflammation. This inflammation triggers the release of Hepcidin, the master regulatory hormone of iron metabolism. Hepcidin is primarily produced by the liver in response to inflammatory cytokines like Interleukin-6 (IL-6). When hepcidin levels rise, they bind to and degrade ferroportin. This effectively "locks" the iron inside the cells of the gut and the liver, preventing it from entering the plasma. This is a defensive evolutionary mechanism designed to starve invading pathogens of iron (nutritional immunity), but in the context of chronic SIBO, it results in a permanent "lockdown" of iron stores, starving the brain of the essential mineral required for dopamine regulation.
---
##
Mechanisms at the Cellular Level
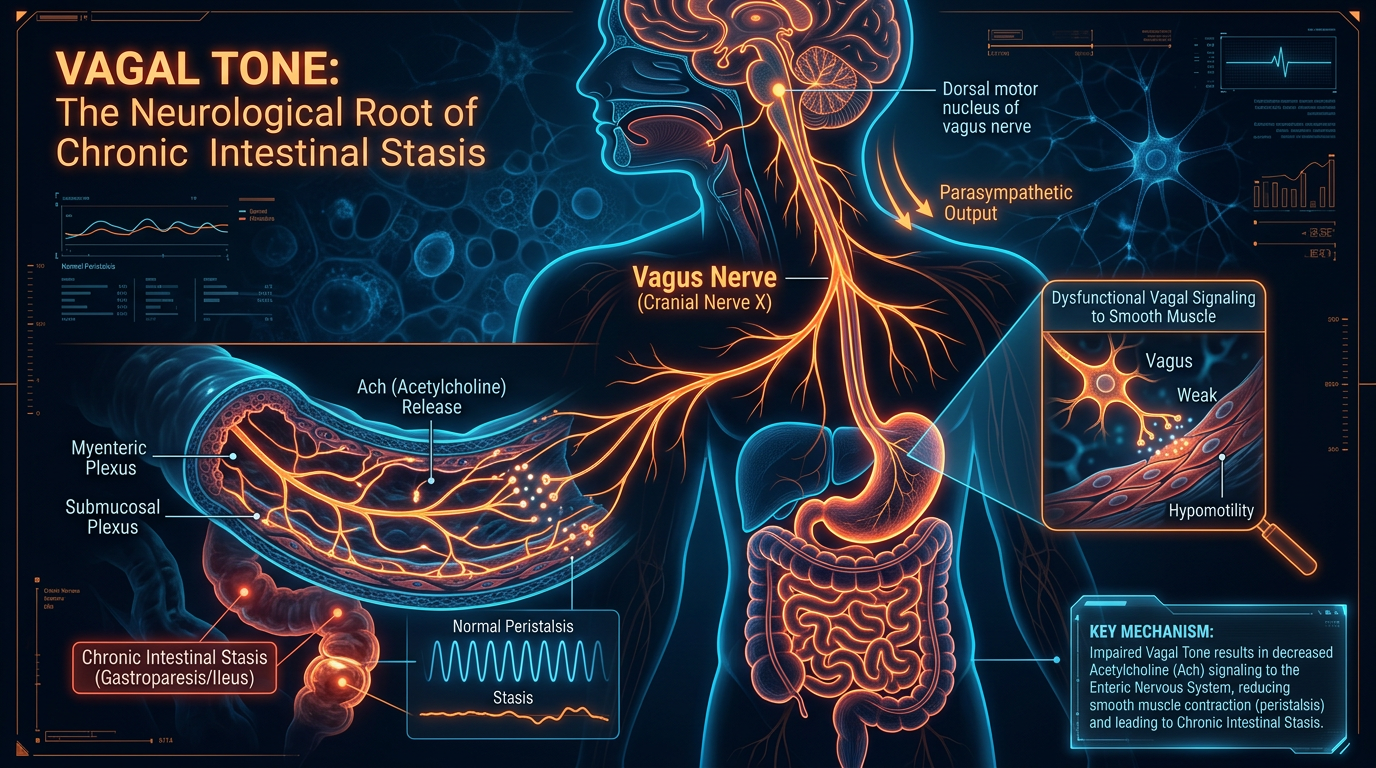
The transition from gut-based iron sequestration to the neurological symptoms of RLS involves a complex disruption of the Basal Ganglia and the dopaminergic pathways. To the senior researcher, the cellular mechanics reveal a clear path of causality that mainstream "symptom-management" models frequently ignore.
Iron as a Co-factor for Dopamine
The primary neurotransmitter implicated in RLS is Dopamine. Dopamine is responsible for the regulation of smooth motor control and the "reward" signals in the brain. The rate-limiting enzyme in the synthesis of dopamine is Tyrosine Hydroxylase (TH). This enzyme is strictly iron-dependent.
If the brain—specifically the substantia nigra—is deficient in iron, Tyrosine Hydroxylase cannot function optimally. This leads to a precipitous drop in dopamine production. The "restlessness" experienced by patients is, at its core, a desperate neurological signal resulting from fluctuating dopamine levels. Without sufficient iron to stabilise this process, the neural circuits governing movement become hyper-excitable, particularly during the evening hours when dopamine levels naturally dip.
The Blood-Brain Barrier (BBB) Paradox
One of the most confounding aspects of RLS for many clinicians is the presence of "normal" serum ferritin levels in patients who exhibit clear signs of iron-deficiency-driven RLS. This is where the cellular mechanism becomes critical. The brain regulates its own iron homeostasis independently of the systemic supply. Iron is transported across the blood-brain barrier via Transferrin Receptor 1 (TfR1).
In the state of chronic inflammation induced by SIBO, the "iron lockdown" mentioned previously (mediated by hepcidin) also affects the brain's endothelial cells. Research has shown that RLS patients often have a decreased expression of transferrin receptors in the substantia nigra. Essentially, even if there is iron in the blood, the "gates" to the brain are closed. This Cerebral Iron Deficiency is the smoking gun of RLS. The gut-brain axis, mediated by inflammatory cytokines from SIBO, effectively "blinds" the brain to the body's iron stores.
Mitochondrial Dysfunction in the Enterocyte
At the cellular level within the gut, the overgrowth of bacteria disrupts the mitochondrial function of the intestinal villi. Bacteria like *Proteus mirabilis* produce hydrogen sulphide and other metabolic by-products that interfere with cellular respiration. When the enterocytes are energy-starved, the active transport mechanisms required for mineral absorption fail. This creates a vicious cycle: SIBO causes malabsorption, and the resulting nutrient deficiencies weaken the gut's immune response, allowing the SIBO to proliferate further.
---
##
Environmental Threats and Biological Disruptors
The sudden surge in both SIBO and RLS cases over the last three decades suggests that this is not merely a genetic predisposition but an environmental catastrophe. Modern living has introduced several biological disruptors that directly facilitate the Iron-SIBO connection.
The PPI Epidemic
Perhaps the most significant disruptor is the widespread over-prescription of Proton Pump Inhibitors (PPIs) such as Omeprazole and Lansoprazole. In the UK, millions of prescriptions are issued annually for "acid reflux." However, stomach acid is the body's primary defence against bacterial ingress. Hypochlorhydria (low stomach acid) allows oral and colonic bacteria to survive the gastric pass and colonise the small intestine. Furthermore, iron requires an acidic environment to be converted into its absorbable ferrous form. By suppressing acid, PPIs simultaneously invite the "thieves" (SIBO) and remove the "keys" (acid) needed for iron absorption.
Glyphosate and Mineral Chelation
The ubiquitous use of Glyphosate in modern agriculture represents a direct threat to iron homeostasis. Glyphosate was originally patented as a chelator—a molecule designed to bind tightly to minerals. When consumed via the food supply, glyphosate binds to dietary iron, manganese, and zinc, rendering them unavailable for human absorption but often still accessible to certain pathogenic bacteria that have evolved glyphosate-resistant pathways. This creates an environment where the host is starved of minerals while the dysbiotic flora thrives.
Ultra-Processed Foods and Biofilm
The modern British diet, high in emulsifiers and acellular carbohydrates, provides the perfect substrate for bacterial biofilms. These biofilms are protective "shields" that bacteria build around themselves in the small intestine. They are composed of polysaccharides and, crucially, sequestered iron. Biofilms make SIBO incredibly difficult to eradicate with standard antibiotics and act as a permanent "iron trap," preventing the host from accessing the minerals contained within the food bolus.
Statistics indicate that individuals on long-term PPI therapy have a 50-80% increased risk of developing SIBO, which directly correlates with the rising prevalence of secondary Restless Leg Syndrome.
---
##
The Cascade: From Exposure to Disease
The progression from a healthy gut to a neurologically compromised state is not instantaneous; it is a multi-stage biological cascade. Understanding this timeline is essential for both prevention and reversal.
Stage 1: The Initial Insult
The cascade typically begins with an insult to the Migrating Motor Complex (MMC)—the "internal housekeeper" of the small intestine that sweeps bacteria toward the colon. This insult could be a bout of food poisoning (post-infectious IBS), chronic stress, or the use of medications like opioids or PPIs. When the MMC is impaired, the small intestine becomes stagnant.
Stage 2: Colonisation and Sequestration
Bacteria from the large intestine begin to migrate upwards. As they establish colonies in the duodenum, they begin the process of iron sequestration. At this stage, the patient may notice bloating, flatulence, or "brain fog," but the neurological symptoms of RLS have not yet manifested. The body is drawing upon its ferritin stores in the liver to maintain systemic balance.
Stage 3: The Inflammatory Switch
As the bacterial load increases, the intestinal barrier (the "tight junctions") begins to fail, leading to Intestinal Permeability (Leaky Gut). Lipopolysaccharides (LPS)—toxins from the cell walls of Gram-negative bacteria—enter the bloodstream. This triggers a systemic inflammatory response. The liver, sensing this "infection," ramps up hepcidin production.
Stage 4: Systemic and Cerebral Depletion
With hepcidin elevated, iron is no longer exported from storage. Serum iron levels drop, and the saturation of transferrin (the transport protein) decreases. The brain, sensing a shortage, attempts to upregulate its receptors, but the systemic inflammatory signals interfere with this process. The substantia nigra begins to experience true iron starvation.
Stage 5: The Symptomatic Threshold
Once the iron levels in the brain drop below a critical threshold, dopamine synthesis falters. The patient experiences their first "restless" night. Over time, as the SIBO persists and the iron theft continues, the symptoms become more frequent and more intense. The "creepy-crawly" sensations are the brain’s way of screaming for the iron it needs to synthesise the neurotransmitters of movement.
---
##
What the Mainstream Narrative Omits
The current medical approach to Restless Leg Syndrome is, in the view of many integrative researchers, fundamentally flawed. By focusing almost exclusively on dopamine agonists and oral iron supplementation without addressing the gut, the mainstream narrative fails to provide a long-term solution.
The Dopamine Agonist Trap
The standard of care for RLS often involves drugs like Ropinirole or Pramipexole. These drugs work by mimicking dopamine in the brain. While they may provide temporary relief, they frequently lead to a phenomenon known as Augmentation. Over time, the brain becomes less sensitive to dopamine, and the RLS symptoms actually worsen, spreading to the arms and occurring earlier in the day. The mainstream narrative omits the fact that these drugs do nothing to address the *cause* of the low dopamine—the iron-thieving bacteria in the gut.
The Fallacy of Oral Iron Supplementation
When iron deficiency is identified, the standard response is to prescribe high-dose oral iron (e.g., Ferrous Sulphate). However, in the presence of SIBO, this is akin to throwing fuel on a fire. Pathogenic bacteria thrive on supplemental iron. Much of the unabsorbed iron reaches the lower gut, where it further disrupts the microbiome, promotes the growth of virulent strains, and causes oxidative stress to the intestinal lining. This is why many RLS patients find that oral iron supplements cause extreme gastrointestinal distress without significantly improving their RLS symptoms or their ferritin levels.
The "Normal" Ferritin Mirage
Mainstream medicine often considers a ferritin level of 15-30 ng/mL as "normal." However, for a patient with RLS, these levels are often woefully inadequate. Evidence suggests that RLS symptoms may only resolve when ferritin levels are pushed above 100 ng/mL. Furthermore, the narrative fails to acknowledge that ferritin is an "acute phase reactant"—it rises during inflammation. A patient with SIBO might have a "normal" ferritin level of 50 ng/mL, but this may be artificially inflated by the inflammation in their gut, masking a profound underlying deficiency.
---
##
The UK Context
The United Kingdom presents a unique landscape for the RLS-SIBO connection. The structure of the National Health Service (NHS), while a pillar of British society, often struggles with the multidisciplinary approach required to treat complex gut-brain disorders.
The Diagnostic Gap
In the UK, SIBO is rarely tested for in a primary care setting. The standard "Gold Standard" for SIBO diagnosis—the Lactulose Breath Test—is often only available through private functional medicine clinics or specialised gastrointestinal centres in London and other major cities. Consequently, thousands of Britons are diagnosed with "idiopathic" RLS and placed on lifelong medication without ever having their small intestine assessed.
The Rise of PPI Usage
The UK has seen a dramatic rise in the use of acid-suppressing medications. According to NHS Digital, prescriptions for PPIs have increased year-on-year. This correlates with the rising "Westernised" diet and the high stress levels of modern British life. The consequence is a "perfect storm" for SIBO-driven iron deficiency. The lack of public awareness regarding the long-term neurological consequences of PPI use is a significant omission in British public health discourse.
Socioeconomic Factors and Nutrition
The "Cost of Living" crisis in the UK has forced many into a higher consumption of shelf-stable, ultra-processed foods. These foods are devoid of the "haeme" iron found in high-quality meats and are often fortified with inorganic, non-haeme iron that is difficult to absorb and easy for bacteria to sequester. This creates a socioeconomic divide where the most vulnerable are at the highest risk of developing SIBO and its subsequent neurological fallout.
Data from the UK’s NICE (National Institute for Health and Care Excellence) guidelines still focus heavily on pharmaceutical interventions for RLS, with minimal mention of investigating the microbiome or small intestinal health as a primary diagnostic step.
---
##
Protective Measures and Recovery Protocols
Recovery from RLS-induced by SIBO requires a sophisticated, two-pronged approach: eradicating the overgrowth and restoring iron homeostasis without feeding the pathogens.
Eradicating the Overgrowth (The "Kill" Phase)
To stop the theft of iron, the bacterial overgrowth must be addressed. While systemic antibiotics like Rifaximin are often used, many researchers favour a botanical approach that disrupts biofilms and kills pathogens while sparing beneficial flora.
- —Allicin (from Garlic): Highly effective against methanogenic bacteria.
- —Berberine: A potent antimicrobial that also helps restore the intestinal barrier.
- —Neem: Historically used in Ayurvedic medicine to clear the small intestine of dysbiotic organisms.
The Role of Lactoferrin
One of the most revolutionary "protective measures" is the use of Lactoferrin. Lactoferrin is a protein found in colostrum that has a dual function. It has an incredibly high affinity for iron—higher than bacterial siderophores. It "steals" the iron back from the bacteria, effectively starving them, but it then delivers that iron directly to the human host’s receptors. This makes it an ideal supplement for RLS patients, as it bypasses the bacterial "iron trap" and helps resolve the deficiency without feeding the SIBO.
Nutritional Strategy: The Low-FODMAP and Elemental Diet
To starve the bacteria, one must limit their food source. A Low-FODMAP diet (Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols) reduces the fermentable substrates available in the small intestine. In severe cases, an Elemental Diet—consisting of pre-digested nutrients that are absorbed in the first few inches of the duodenum—can be used for 14 days to literally "starve" the bacteria out while providing the host with essential minerals.
Restoring the Migrating Motor Complex
Preventing relapse is as important as the initial kill phase. Supporting the MMC ensures that bacteria do not migrate back into the small intestine.
- —Prokinetics: Natural agents like Ginger and 5-HTP can help stimulate the waves of the MMC.
- —Intermittent Fasting: Allowing at least 4-5 hours between meals (and 12 hours overnight) is essential, as the MMC only functions in a "fasted" state.
- —Vagus Nerve Stimulation: Techniques such as gargling, singing, or cold-water immersion can improve the "gut-brain" connection and enhance intestinal motility.
Iron Repletion: A Nuanced Approach
Once the SIBO is under control, iron stores must be rebuilt. Haeme iron (found in liver, red meat, and shellfish) is much more bioavailable and less likely to be utilised by bacteria than non-haeme iron. If oral iron is not tolerated, Intravenous (IV) Iron Infusion may be necessary to bypass the gut entirely and deliver the mineral directly into the systemic circulation, providing the brain with the immediate resources it needs to restart dopamine production.
---
##
Summary: Key Takeaways
The investigation into the Iron-SIBO Connection reveals that Restless Leg Syndrome is not a mysterious, incurable defect of the brain, but a logical biological consequence of a disrupted internal ecosystem. The theft of iron by bacterial siderophores in the small intestine creates a cascade of "nutritional immunity" and inflammation that ultimately starves the substantia nigra of the catalyst it needs to regulate movement and mood.
- —SIBO is a Primary Driver: Bacterial overgrowth in the small intestine sequesters dietary iron, leading to systemic and cerebral deficiencies.
- —The Siderophore Theft: Bacteria use high-affinity molecules to "out-compete" the host for minerals, making standard oral iron supplementation often ineffective or counterproductive.
- —The Dopamine Connection: Low iron in the brain inhibits Tyrosine Hydroxylase, the enzyme responsible for dopamine synthesis, triggering the symptoms of RLS.
- —Environmental Catalysts: The overuse of PPIs, the presence of glyphosate in the food chain, and the British "ultra-processed" diet have created a modern epidemic of SIBO.
- —Beyond Symptom Management: Treating RLS requires more than dopamine agonists; it requires a comprehensive protocol of gut eradication, biofilm disruption, and bioavailable iron restoration.
- —UK Healthcare Gap: There is an urgent need for the NHS and British medical institutions to integrate SIBO testing and microbiome analysis into the standard diagnostic workup for neurological conditions.
At INNERSTANDING, we believe that the path to true health lies in uncovering these hidden connections. By reclaiming the health of the small intestine and protecting our internal mineral stores from microbial theft, we can silence the "restless" signals of the nervous system and restore the profound rest that is the right of every human being. The twitching limb is but a messenger; the gut is where the solution resides.
This article is provided for informational and educational purposes only. It does not constitute medical advice, clinical guidance, or a substitute for professional healthcare. Information reflects cited research at time of publication. Always consult a qualified healthcare professional before acting on any health information.
RESEARCH FOUNDATIONS
Biological Credibility Archive
Research indicates a high prevalence of Small Intestinal Bacterial Overgrowth among patients with Restless Leg Syndrome, suggesting an inflammatory or malabsorptive link.
Systemic and brain-specific iron deficiencies are confirmed as key pathophysiological drivers in the development and severity of Restless Leg Syndrome symptoms.
The hormone hepcidin regulates systemic iron availability and is frequently elevated by the chronic low-grade inflammation often seen in intestinal dysbiosis.
The gut microbiota significantly influences host iron homeostasis by modulating intestinal transporters and competing for iron resources within the small intestine.
Antibiotic treatment for Small Intestinal Bacterial Overgrowth resulted in significant clinical improvement of Restless Leg Syndrome symptoms in a majority of study participants.
Citations provided for educational reference. Verify via PubMed or institutional databases.
Medical Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional before making any changes to your diet, lifestyle, or health regime. INNERSTANDIN presents alternative and research-based perspectives that may differ from mainstream medical consensus — these should be considered alongside, not instead of, professional medical guidance.
Read Full DisclaimerReady to learn more?
Continue your journey through our classified biological research.
DISCUSSION ROOM
Members of THE COLLECTIVE discussing "Restless Leg Syndrome: Investigating the Iron-SIBO Connection"
SILENT CHANNEL
Be the first to discuss this article. Your insight could help others understand these biological concepts deeper.
THE ARSENAL
Based on SIBO & Small Intestine Health — products curated by our research team for educational relevance and biological support.

Magnesium Blend – The Most Important Mineral

Clean Slate – Detoxes thousands of chemicals,heavy metals, pesticides, allergens, mold spores and fungus

Vegan Essential Amino Acids – Plant-Powered Protein Building
INNERSTANDING may earn a commission on purchases made through these links. All products are selected based on rigorous educational relevance to our biological research.
RABBIT HOLE
Follow the biological thread deeper